
Abstract
Objectives:
To propose at the auriculotherapists a New Universal Nomenclature of Auriculotherapy, able to receive any mapping whatsoever.
Design:
We built this proposition by using electronic database search to find the different formulations of Auricular Acupuncture Points (AAPs), by studying neuroradiology methods describing reliable and reproducible marks able to adapt to all brain morphologies, by studying the analysis of brain dissections, showed us the internal organization of the brain; and after having proved the neurophysiological correlations between auricular displays and their brain correspondences.
Results:
Since the 1950s, the study of Auriculotherapy by Paul Nogier and his students regularly progressed. The World Health Organization recognized it in 1987 and developed the First International Nomenclature in 1990. The number of therapeutic zones of the ear, in proportion to the constant progress in neurophysiology, never stops growing. This growth presents a major problem: all the first classifications became inappropriate and unfit. We propose a Universal Nomenclature of Auriculotherapy which is a biomathematical model of the brain anatomic organization, with 189 areas on the lateral ear and 89 areas on the medial ear.
Conclusion:
The Universal Auriculotherapy Nomenclature we proposed to the World Federation of Chinese Medicine Societies and which approved it at its International Convention in September 2011 in London, gives accurate Cartesian Marks and is able to receive any mapping whatsoever. Dispatching around 57 countries (Europe, America, China, Russia and Africa) and 195 Acupuncture Societies, it will facilitate the work of auriculotherapists and allow a scientific progress of the subject worldwide. This progress will allow the largest number of people to have a common tool for education, research, and publications of the discipline.
Introduction
A
Since the rediscovery of Auriculotherapy by Paul Nogier in 1957 in Lyon (France), and his brilliant vision of a fetus curled up in the ear pavilion, presaging the understanding of his somatotopic bases, modern neuroscientific knowledge has allowed us, as neurophysiologists, to bring understanding of the neurophysiological bases of its action.
Since this scientific certification, its development, universal propagation, and academic education have never stopped developing, just like the multiplication of clinical and experimental study publications.
After Dr. Paul Nogier's initial cartography of the ear, multiple cartographies have been developed by different authors/countries/schools. Until recently, the construct of these cartographies was anatomically based. Basically, the ear was divided in anatomic zones (helix, Antihelix, Tragus, Lobule, etc.) and each zone was subdivided in areas. This led to the description of each point by a letter referring to the zone and a number referring to an area within the zone.
The World Health Organization (WHO) recognized it in 1987 and developed its first International Nomenclature in 1990 (Fig. 1). Its continuous development currently requires an update of its international standardization.
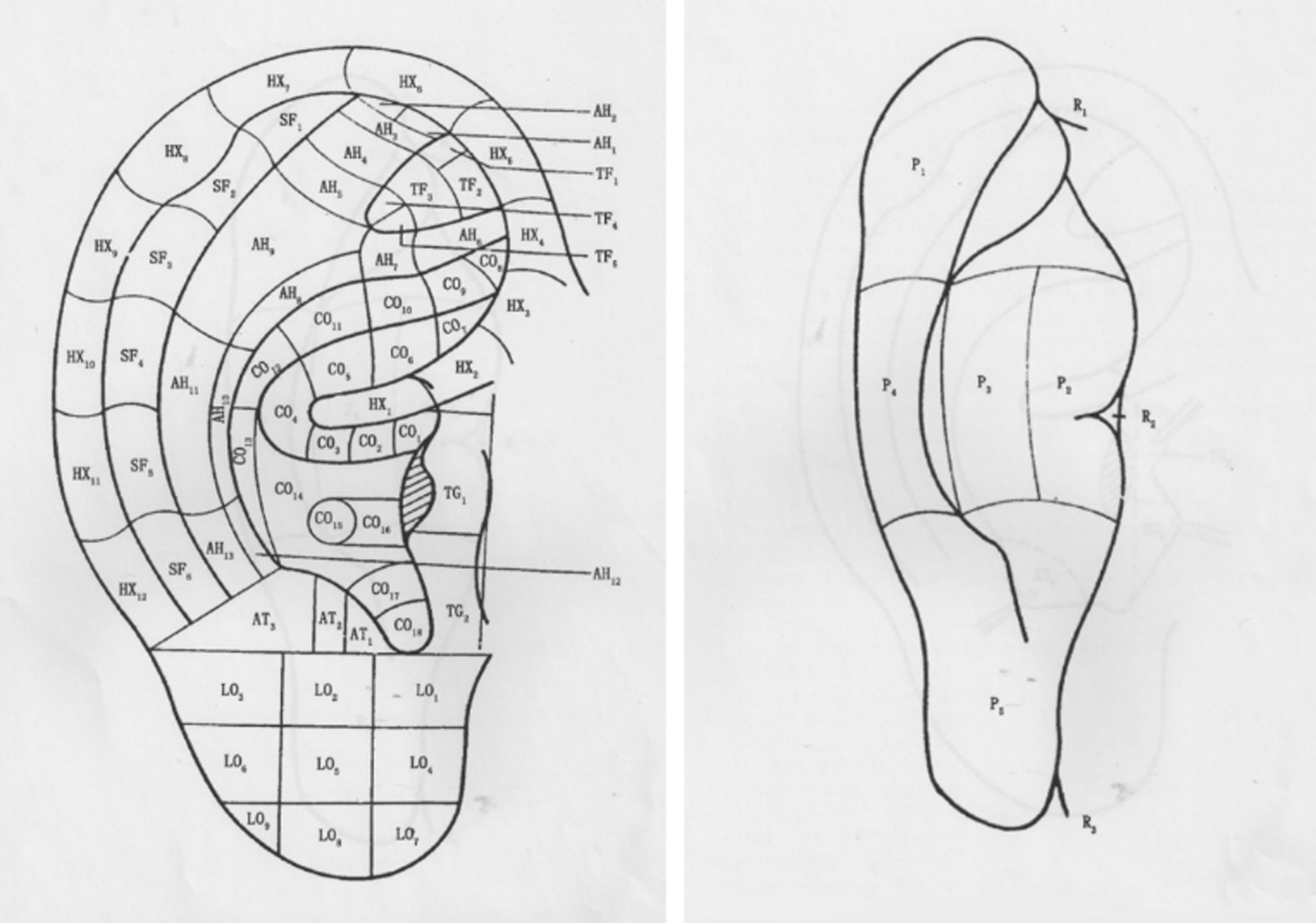
First International Nomenclature of World Health Organization, published in 1990.
The universal nomenclature we proposed is a biomathematical model of the brain neuroanatomic organization, on which the ear pavilions are connected. It was ratified by the World Federation of Chinese Medicine Societies (WFCMS) during its 8th Convention in London, on September 2 and 3, 2011, with the actual participation of Dr. Qi Zhang, MD, Coordinating of the Traditional Medicine Department, at the WHO.
Methods
We use three items: 1. Using electronic database searches, we try to find the different formulations of Auricular Acupuncture Points (AAPs) in the following: the Chinese National Knowledge, The National Science and Technology Library, the Western databases, PubMed, the German Journal of Acupuncture, and proceedings of International Symposiums of Auriculotherapy, from 1958 to 2012. Several different propositions of AAPs were formulated: method based on points for the anterior of the auricle, method based on subzones for the anterior of the auricle, method based on the divided subzones according to anatomy of the anterior of the auricle, method based on Nogier's point Zero for the anterior of the auricle, method based on both points and subzones of the anterior of the auricle, method based on smaller subzones of the anterior of the auricle, method based on subzones, points, and lines for the anterior and posterior of the auricle, and finally, method based on subzones, points, and lines for full cover of the anterior and posterior of the auricle. 2. The first persons to be interested in brain architectonics were the neurosurgeons, who absolutely needed reliable presurgical marks to damage as little as possible the brain structures, which are all noble. By studying neuroradiology methods, whose aim was to describe reliable and reproducible marks able to adapt to all brain morphologies, despite a certain level of interindividual and intraindividual variabilities. 3. By studying the analysis of brain dissections, made by one of our students, an anatomist, Mr. Jean Castellier, MD, showed us the internal organization of the brain. 4. At the same time, we proved the neurophysiological correlations existing between auricular displays and their brain correspondences.
Results
Analyzing a Chinese draft of International Standard of Auricular Acupuncture Points (ISAAPs): the location of AAPs is based on the anatomy of the surface of the ear, with combination of zones and points, based on studies from American and European countries.
Analyzing drafts of ISAAPs from western countries: Oleson, in 1983 1 and 1996, 2 proposed a method of auricle zone nomenclature, named the zones by English letters and numbers, but without AAP names. Wojak divided the zones into subzones using abscissa and vertical coordinates in 2010. This was difficult to use clinically because it was not convenient for manipulation. Romoli and Mazzoni, in 2009, 3 from Italy, also developed a grid with a variable number of sectors centered in point Zéro. However, no ears have exactly the same shape, so is difficult to serve as a repeatable standard location method.
Analyzing drafts of ISAAPs from international symposiums: the WHO discussed and approved 39 AAPs, in 1990. 4 Of them, 24 were based on nomenclature of Nogier and 15 were based on Chinese AAPs. Oleson put forward an English abbreviation with a number on these AAPs. The World Federation of Acupuncture-Moxibustion Societies (WFAS) 5 developed 93 AAPs; 34 were based on the nomenclature and location of Nogier, 21 were based on the anatomical terminology of the surface of the auricle, and 38 were based on Chinese AAPs. Of these 93 AAPs of WFAS, all of them were named with English abbreviations and numbers, 18 were named for the point rather than zone, and 75 were based on the zone nomenclature system put forth by Oleson. The WFCMS took sensibly the same AAPs, located 10 zones, while WFAS located 9 zones. 6 Finally, WFCMS locates 10 “zones” and identified 91 points in those 10 areas; WFAS locates 9 “divisions” and identifies 75 “areas” in these nine divisions.
Discussion
By reviewing these literatures, the method of developing ISAAPs, the same way of thinking as in developing body acupuncture points has been used, while the specialty of AAPs has been neglected.
The number of AAPs, in proportion to constant discoveries of neurophysiology, never stops growing. This increase presents a major problem: the first classification has become insufficient and unfit. In fact, dating back to more than 20 years, it can no longer report the quasi doubling of the number of points, resulting from the progress of the neurophysiological knowledge.
Most authors who publish on the topic make several remarks: • they confirm the pluripotency of points (“one point for several diseases, or one disease with several points”), while noticing a precise location of points is the key of efficiency and of its world distribution,
7
• they lament the diversity of used mappings and nomenclatures, and the lack of universal standardization, acting as a brake to the development of the discipline,
8,9
• or they regret the time spent to try and find the point location, on account of a lack of clarity and accurate and universal classification.
10
Others try to redefine the anatomic limits of ear pavilions, in the hope of discovering a new nomenclature. 11 Finally, others, by reviewing the indications and action mechanisms of auricular acupuncture, denounce the lack of international nomenclature, which may adapt to with any mapping whatsoever. Finally, the ultrastructural nature specifies targets reached by the contact with ear reflex zones, 12,13 the power of their action, 14 –16 their specific electrophysiological characteristics, 17 and the extent of age of patients who may benefit from possible auriculotherapy, 18 –20 rendering absolutely necessary the publication of an international nomenclature of auriculotherapy zones.
All the more so as current nomenclatures do not enable to locate precisely all zones of the modern scientific auricular mapping! For instance, the “AH8” location of the current standardization of WFAS and WFCMS, is called “abdomen,” yet modern scientific data locate this zone at the basis of 2 hemi-concha and locate in this “AH8” area no <8 points!
Another instance among others: the “GH6” location, positions “the collar bone,” whereas modern scientific data locate it on the external side of the cervical antihelix and locate in the “GH6” zone no <6 points!
Also, these current standardizations organize the “TG” tragus in 2 zones, whereas modern scientific data locate there are no <8 points! The “LO” lobule is organized in 9 zones, the modern scientific data place in it no <20 points! The medial face of the pavilion is divided into five parts (P1, P2, P3, P4, and P5), whereas we count no <28 points according to modern scientific data!
The French Academic Scientific School of Auriculotherapy, which I have the honor to run, identifies more than 190 zones: it is impossible to place them in the current nomenclatures!
The first persons to be interested in brain architectonics were the neurosurgeons, who absolutely needed reliable presurgical marks to damage as little as possible the brain structures, which are all noble.
In 1909, Korbinian Broadmann defined 52 brain cortex areas connected with different functions that he called “Cytoarchitectonics.” 21 In 1950, Wilder Penfield and Theodor Rasmussen developed the brain zone mapping, managing the body motor function and sensitiveness, which they called “Homunculus.” 22,23 In 1957, Jean Talairach and Pierre Tournoux, 2 French neuroradiologists introduced a reference document and published in 1988 an Atlas of brain cross sections, enabling accurate stereotaxic marks in neuroradiology. 24
Recently, Laird et al. proposed a new method called “Lancaster's Transform” to modernize these stereotaxic marks of neuroradiology. 25
We recorded for all these works that, their fundamental axes went through the middle of the corpus callosum.
The analysis of brain dissections, made by one of our students, an anatomist, Mr. Jean Castellier, MD, showed us that the middle of the corpus callosum was the epicenter of the somatotopic organization of the brain homunculus (Fig. 2) and the latter was divided into 20 segments. 25,26

Brain dissection showing that the middle of the corpus callosum is the epicenter of somatotopic organization of the brain homunculus.
At the same time, we proved the neurophysiological correlations existing between auricular displays and their brain correspondences. 27,28
We used all these data to finalize an “Auriculogram,” the Universal Nomenclature we proposed to the WFCMS is based on neuroembryological and neurophysiological data. 24 –33
We calculated the ideal angle of this auriculogram, by taking as a base is the anatomic structures of the ear which are constant in all human beings. Our works led us to record that the ties of the helix knee and the lobule to the face are always aligned on a perfect straight line, which always goes through the auricular representation of the corpus callosum (Fig. 3).
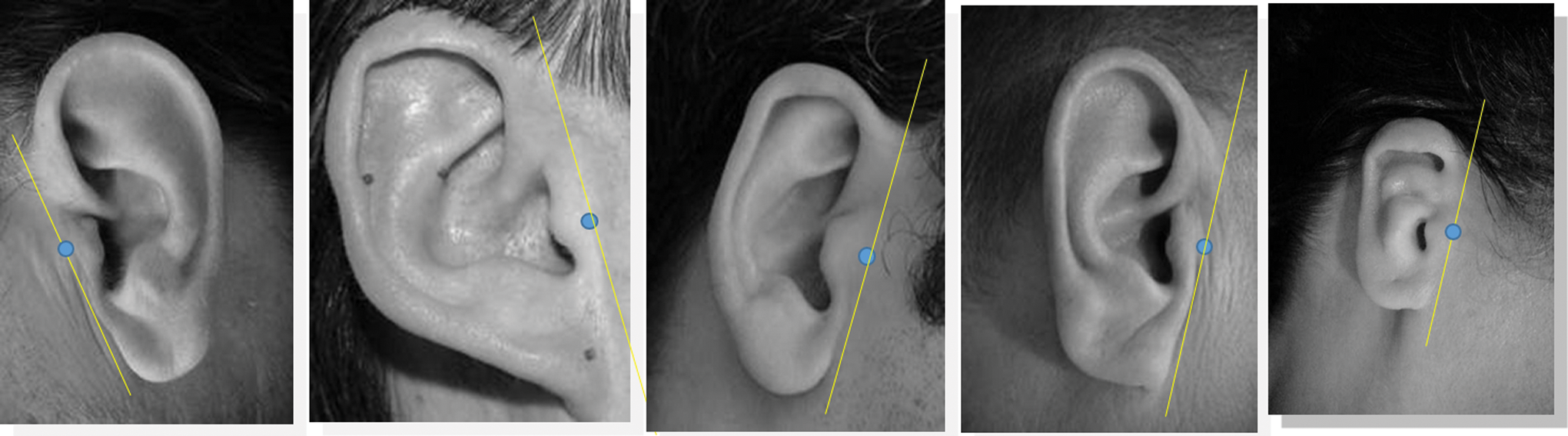
Face ties of the helix knee and lobule are always aligned on a perfect straight line, passing through the auricular representation of the corpus callosum.
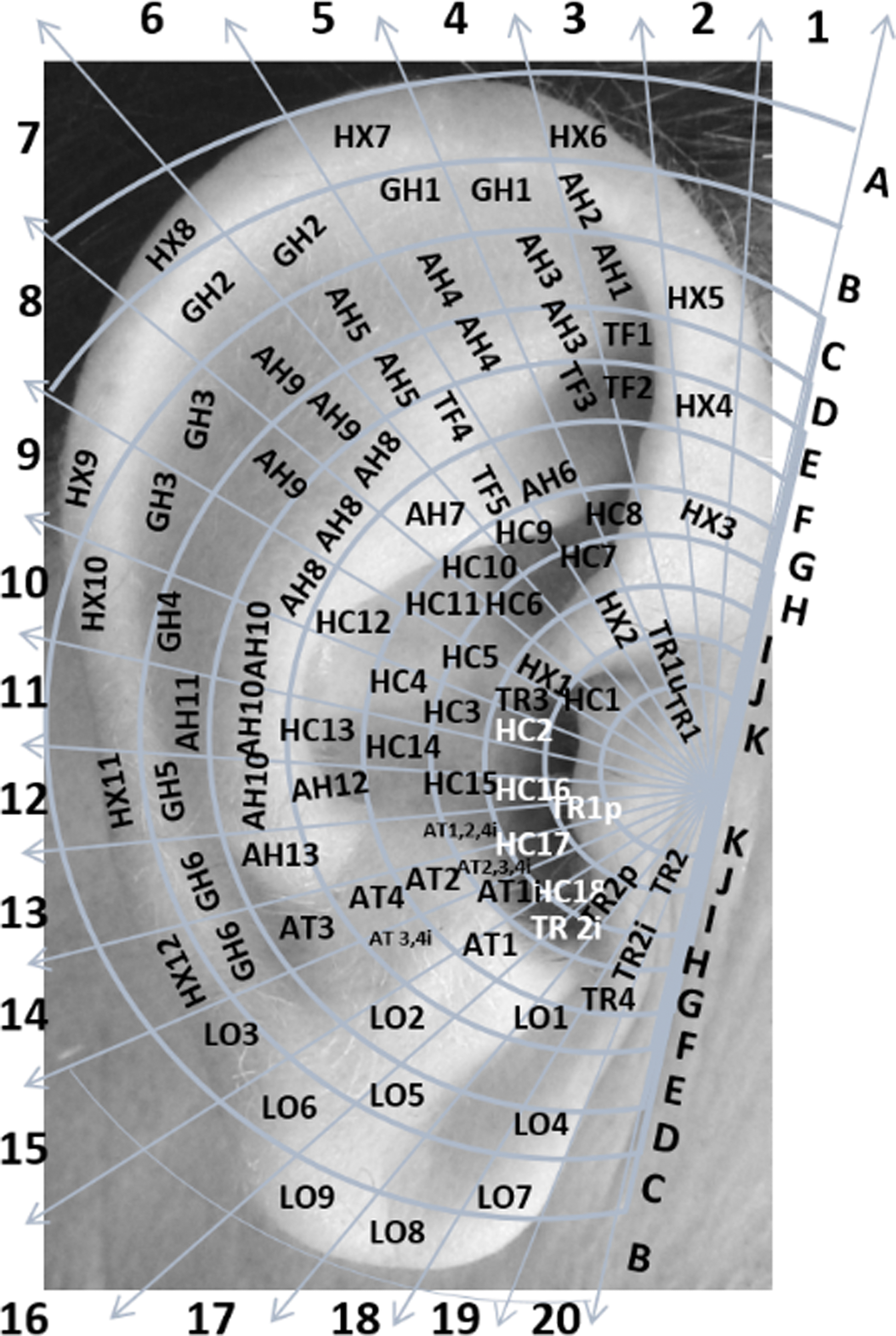
So we have from this point pulled tangents in these ties. We so obtained a semicircle of an angular value of 180°, which we divided into 20 equal angles that is 9°, the obtained group, we named “Segmentogram,” recovering the totality of the surface of the auricle.
These abacus divide the lateral ear in 189 areas and the medial ear in 89 areas (Figs. 4 and 5).

Lateral auricular Segmentogram.

Medial auricular Segmentogram.
This Universal Nomenclature enables to receive any mapping whatsoever, as zones are not designated by their anatomic marks (which does not allow to place them all), but by Cartesian coordinates (x, y) corresponding to their precise locations.
We added different symbols for zones in their loci, which enables to precisely locate them in relationship with ear reliefs: on the lateral side, under an anatomic relief, on the lower face of an anatomic relief, on the medial face (full point, point surrounded by a circle, cross surrounded by a circle, square).
Thus, the transfer from the old to the new auricular mapping of the WHO, and the one of the French Scientific Academic School, clearly appear with precise orthogonal marks, which are easily identified (Figs. 6 –9).
Translation between old and new World Health Organization nomenclature.

Cartography of French University scientific school of Paris (right lateral auriculogram). “Cosmonaut” refers to the sympathetic gangliotome of T12 (approximately equivalent to the Shenmen of Chinese auricular acupuncture); C2 and C7 refer to relevant sensory spinal cord segments; I, II, V1, V2, V3, and IX refer to sensory functions of relevant cranial nerves and their branches; TMJ refers to the sensory aspect of the TMJ; FSH, LH, ACTH, and TSH refer to pituitary hormones, which are, respectively, FSH, LH, ACTH, and TSH. ACTH, adrenocorticotropic hormone; FSH, follicle-stimulating hormone; LH, luteinizing hormone; TMJ, temporomandibular joint; TSH, thyroid-stimulating hormone.

Cartography of French University scientific school of Paris (left lateral auriculogram). VIII refers to cranial nerve VIII; C7 refers to the sensory spinal cord segment of C7.
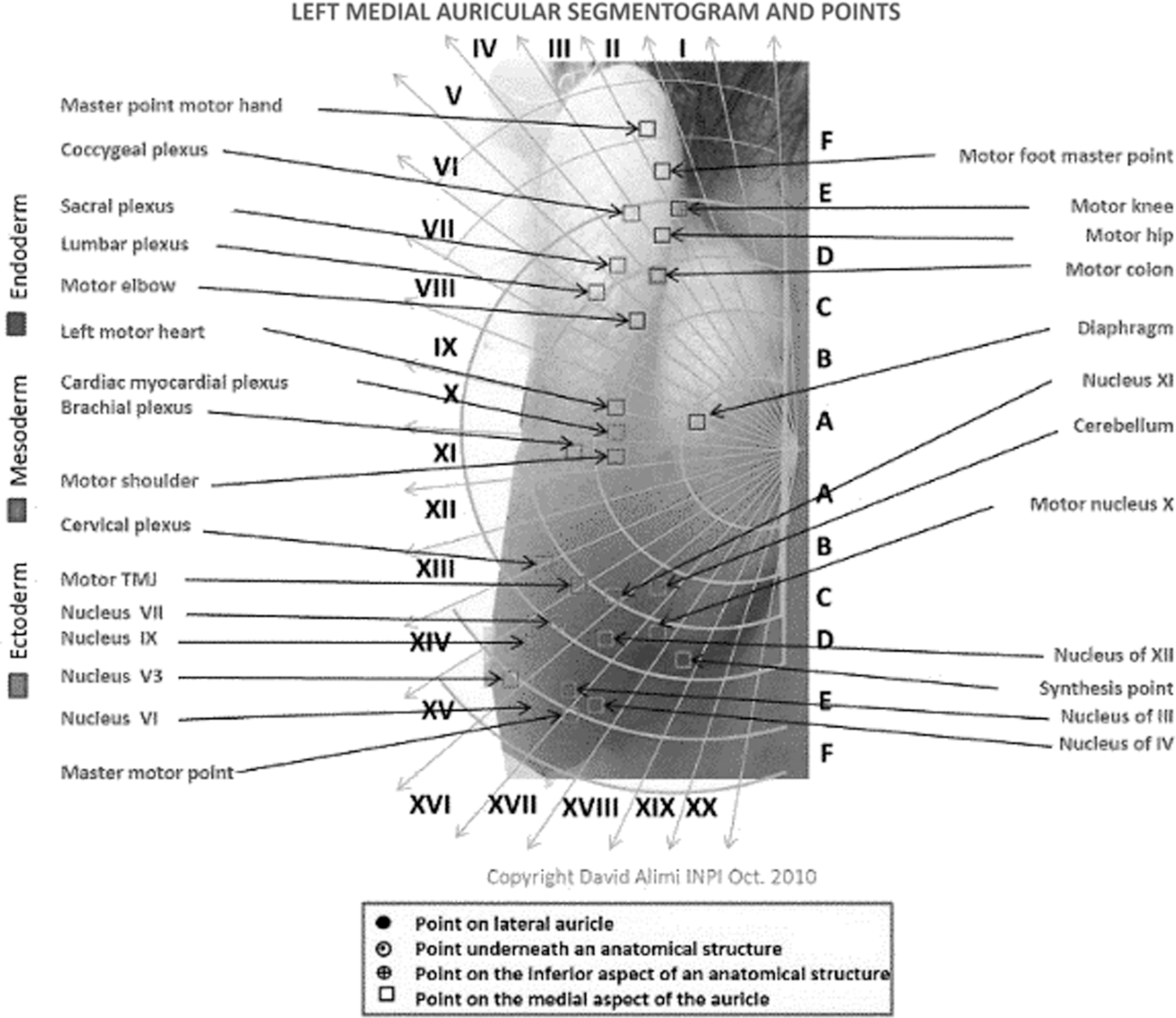
Cartography of French University scientific school of Paris (left medial auriculogram). TMJ refers to the motor functions of the TMJ; III, IV, V3, V1, VII, IX, X, XI, and XII all refer to motor functions of relevant cranial nerve nuclei and their branches. TMJ, temporomandibular joint.
Conclusion
This International Auriculotherapy Nomenclature, approved by the WFCMS, allows 57 countries (Europe, America, China, and Russia) and 195 societies to be represented. It allows homogeneity in the education, research, and publication fields; gives accurate Cartesian marks; and is able to receive any mapping whatsoever. It will facilitate the work of auriculotherapists and allow a scientific progress of the subject worldwide.
Footnotes
Author Disclosure Statement
No competing financial interests exist.