
Abstract
Background:
Multiple sclerosis is considered a complex and heterogeneous disease. Approximately 85% of patients with multiple sclerosis indicate impaired gait as one of the major limitations in their daily life. Acupuncture studies found a reduction of spasticity and improvement of fatigue and imbalance in patients with multiple sclerosis, but there is a lack of studies regarding gait.
Design:
We designed a study of acupuncture treatment, according to the Heidelberg model of Traditional Chinese Medicine (TCM), to investigate if acupuncture can be a useful therapeutic strategy in patients with gait impairment in multiple sclerosis of relapsing-remitting type. The sample consisted of 20 individuals with diagnosis of multiple sclerosis of relapsing-remitting type. Gait impairment was evaluated by the 25-foot walk test.
Results:
The results showed differences in time to walk 25 feet following true acupuncture. In contrast, there was no difference in time to walk 25 feet following sham acupuncture. When using true acupuncture, 95% of cases showed an improvement in 25-foot walk test, compared with 45% when sham acupuncture was done.
Conclusions:
Our study protocol provides evidence that acupuncture treatment can be an attractive option for patients with multiple sclerosis, with gait impairment.
Introduction
M
The clinical manifestations of MS are highly variable and unpredictable. In this sense, gait dysfunction represents one of the most debilitating symptoms experienced by patients with MS. About 85% of individuals with MS report gait impairment as a major limitation of their lives. The majority of persons with walking difficulties also indicate activity restriction (80%), effects on emotional health (70%), and increased concern of falling and other safety issues (70%). 3
The main rehabilitation options for gait impairment in patients with MS are pharmacological treatment of symptoms and physical rehabilitation. Pharmacological treatment of target-specific symptoms has an influence on gait, but adverse side effects and cost are great disadvantages. On the other hand, exercise training can help to mitigate and restore some of the declines in walking function associated with the progression of disability in MS. 4 Symptomatic treatment must be carefully planned, suitable for each patient, as there are possible interactions between treatments for specific symptoms. Different pharmacological and nonpharmacological approaches may be included, but they always need the active involvement of the patient.
Acupuncture is considered to be effective in several diseases and further research is likely to uncover additional areas where acupuncture interventions will be useful. 5 Literature regarding the application of acupuncture in neurological diseases has reported reduction of pain, numbness, and tingling 6,7 ; significant improvement in sensory and motor function and less spasticity 8 ; enhanced motor function 9 ; and significant improvement in fatigue. 10 However, literature regarding gait impairment is scarce.
Based on the Heidelberg model of Traditional Chinese Medicine, an acupuncture prospective, randomized, and controlled study in crossover design was done to try to improve gait problems in patients with MS.
Material and Methods
This study had the collaboration of the two associations of patients with MS with facilities in Oporto region: the “National Association for Multiple Sclerosis” (ANEM) and the “Portuguese Multiple Sclerosis Society” (SPEM).
Patients with diagnosis of MS of relapsing-remitting type (RRMS), greater than 18 years of age, with stable symptoms in the last 2 months, and with an Expanded Disability Status Scale (EDSS) between three and seven were included in the study. Patients with diagnosis of other pathologies, with psychiatric diseases, severe cognitive deficiencies, or EDSS higher than seven, were excluded. After applying the inclusion/exclusion criteria, 20 patients were selected (12 females and 8 males).
After clinical and personal data collection, gait was evaluated in all patients by the 25-foot walk test (T25WF). Patients were not given any previous practice. The following instructions were given to patients for the completion of the test: “walk, as fast and safely as you can, across a clear marked linear 25-feet course. There are no turns, start is static and assistive device can be used.” Patients were then randomized into one of two groups (A and B). The intervention was divided into two moments (Time point 0 and I) (Fig. 1).
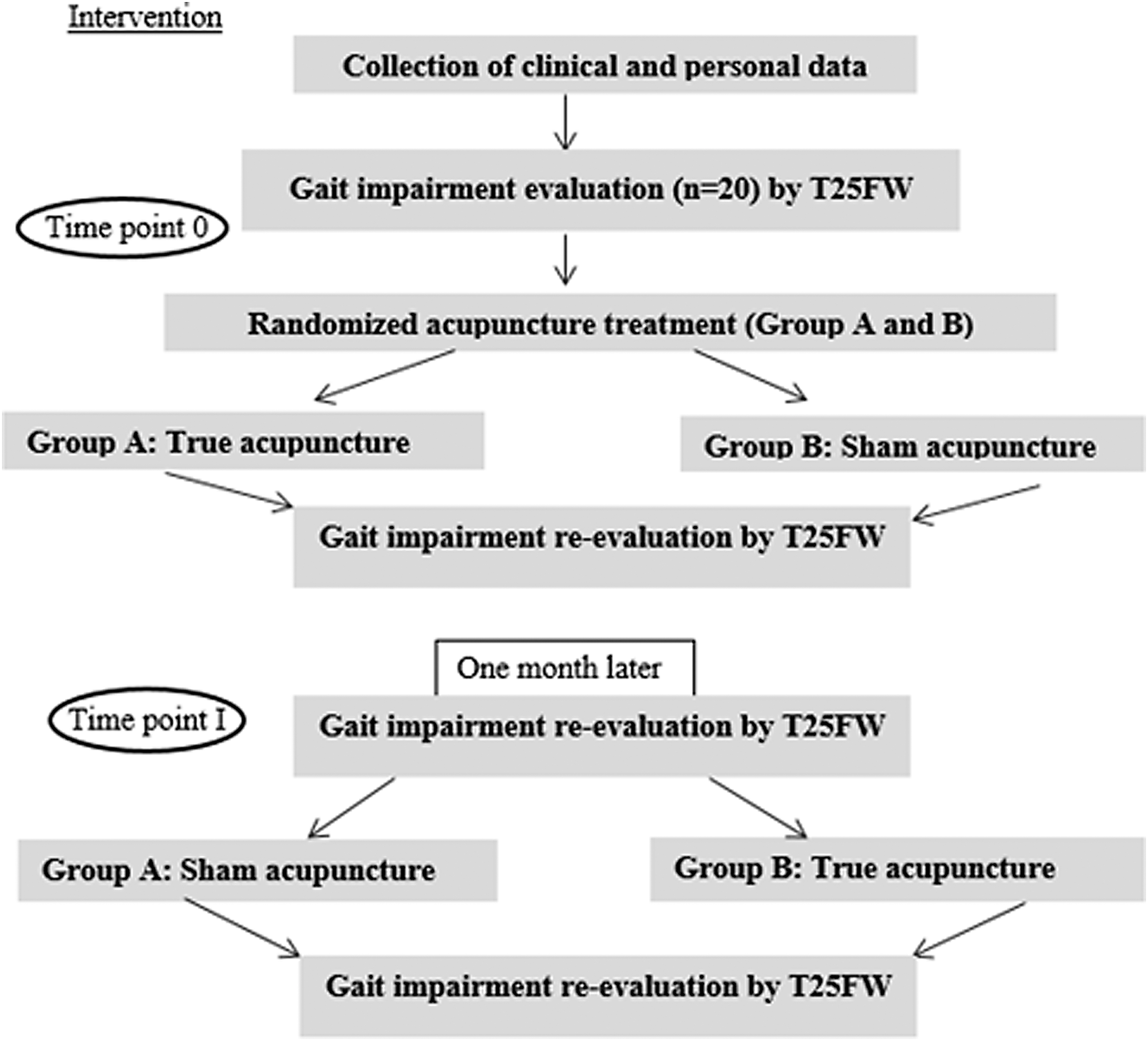
Flowchart of the intervention phase of the study.
In Time point 0, patients of group A received a “true acupuncture treatment” and patients of group B received “sham acupuncture treatment.” All patients of the study were blinded to randomization assignments. Just before and immediately after each treatment, gait impairment evaluation was performed, allowing to evaluate the immediate effect of the acupuncture treatment.
The second moment of intervention (Time point I) happened at least 1 month later. This time, group A patients received “sham acupuncture” and group B “true acupuncture.” So, the results of the study refer to paired samples. Right before and immediately after each treatment, gait impairment evaluation was also performed. As in Time point 0, this procedure allowed to study the immediate effect of the acupuncture treatment. The researchers engaged both in all T25 WF measures, and in the statistical analysis were blinded during the assignment.
Acupuncture treatments were administered only by one acupuncturist. For the study, a standardized acupuncture protocol was developed, based on Heidelberg Model of TCM. The Heidelberg Model of TCM was developed by Greten, supported by the pioneering works of Porket. In this model, the central postulates of classical Chinese Medicine are recompiled and explained as a logical model of system biology. This model unifies the contemporary medical–scientific knowledge with the concepts of different classical schools of Chinese Medicine. 11
True acupuncture was done using acupuncture points based on WHO definitions, anatomically located in the lower extremities: Stomach 34-ST34 (liáng qiü), Bladder 40- BL40 (wei zhöng), and Bladder 57-BL57 (chéng shän). Sham acupuncture was done using points located 2 cun laterally to true acupuncture points, between the main channels. The cun was calculated for each individual based on measurements using the width of the distal interphalangeal joint of the thumb. The “Leopard spot technique” of acupuncture was used both in true and sham treatments. In this technique, some drops of blood were let out from peripheral points by quickly stabbing the skin (five or six times) with the needle. 12,13 For this technique, sterile disposable needles with a size of 30G, 0,30 × 8 mm were used (BD Micro-Fine®). We chose this acupuncture technique because it is described in the literature as being adequate to increase the flow of qi and blood and to disperse blood stasis. 12,13
SPSS (Statistical Package for Social Sciences)® Statistics 20 was used for the statistical analysis of the data. Nonparametric Wilcoxon test for paired samples was used to assess the difference in the time to walk 25 feet before and after each acupuncture treatment. Nonparametric tests had to be used because of the lack of normality distribution of data. All p-values below 0.05 were considered statistically significant.
Results
Sample characterization
The study sample consisted of 20 individuals. All of them were recruited from the two MS associations that are operating in Oporto region, ANEM, and SPEM, as mentioned before. All the individuals had the diagnosis of MS of RRMS, without any relapse in the previous 2 months.
From the 20 patients, 12 were females (60%) and 8 males (40%). These results correspond to a female–male ratio of 1.5. With respect to quantitative variables, we observed a mean age of 46.3 years (±11.07), a mean of the time at diagnosis of 11.4 years (±8.25), and the mean age at diagnosis was 35 years (±12.44). We observed that both the mean age and the mean age at diagnosis were lower in males than in females. These data do not differ from those reported in the outpatient clinic of Braga Hospital with 235 patients enrolled, 14 suggesting that our sample is representative of the MS population in Portugal.
Females pointed out tiredness and misbalance as the main complaint (30% and 25%, respectively). In the male sample, fatigue, tiredness, and misbalance had the same importance (10% each). The use of assistive devices was only observed in the female sample (five women) and they used them in all the T25FW they performed.
Gait assessment before and after acupuncture treatment (25-Foot Walk test)
Results of the T25FW were measured in seconds. Table 1 shows the results obtained before and after each true acupuncture and sham acupuncture treatments. The corresponding percentage of improvement experienced by each patient is also shown for each treatment.
Statistically significant (p < 0.05).
Both group A and B patients did not show statistically relevant differences before intervention when comparing Time point 0 and Time point I results, indicating a sufficient washout period for the crossover.
As can be seen in Table 1, when true acupuncture was done, the differences in time to walk 25 feet before and after true treatment were statistically significant. On the contrary, the differences in time to walk 25 feet before and after treatment with sham acupuncture were not statistically significant. The same results were found when considering males and females separately.
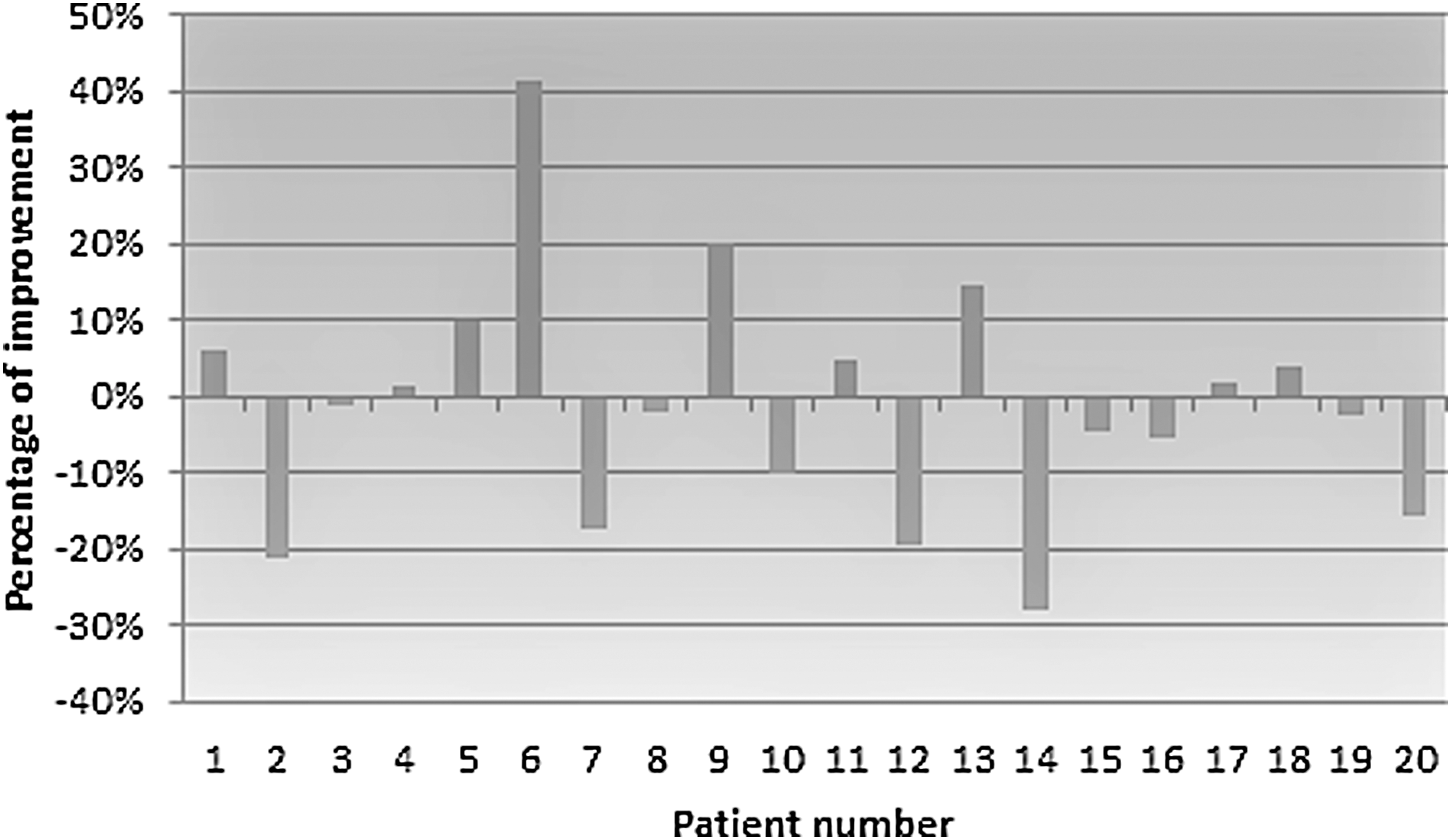
Figure 2 shows the percentage of improvement for each patient when true acupuncture was done, and Figure 3 when sham acupuncture was done. With true acupuncture treatment, all except three patients improved the performance of the test (Fig. 2). The mean percentage of improvement for the whole sample was 13.9%. Analyzing males and females separately, we found that for females the mean percentage of improvement was 17.5% and 8.6% for males. When sham acupuncture was done, although some patients improved the performance of the test, we cannot see a positive mean percentage of improvement (Fig. 3).

Percentage of improvement in the T25FW when true acupuncture was done.
Percentage of improvement in the T25FW when sham acupuncture was done.
Discussion
Most of the clinical manifestations of MS represents causes of disability that lead to severe difficulties in the daily life of these patients, and gait dysfunction represents one of the most weakening symptoms. 3 Gait is a complex process involving coordination of multiple systems of the body. Thus, several factors, such as weakness and spasticity, loss of co-orientation, and cerebellar lesions, together with visual and cognitive dysfunction, pain, and also environmental and personal factors can contribute to walking disability. 15 –17
One of the priorities managing with MS is to define strategies to control the symptoms and to prevent secondary complications and increased disability associated with the disease. Acupuncture represents a potential useful therapeutic option to consider within the overall management of symptoms of these patients. Scientific literature regarding the application of acupuncture in neurological diseases has been reported. 6 –10 However, literature regarding gait impairment is scarce and, therefore, additional studies, using appropriate outcome measures, are required.
Taking this into account, the present study was designed to investigate if acupuncture treatment, according to the Heidelberg model of TCM, can be a useful therapeutic option in patients with gait impairment in MS of RRMS.
With respect to sample characterization, our results do not differ from that reported for other populations. 18,14 Our results refer to paired samples. Frequent problems in research of acupuncture have to do with finding an adequate control group 19 and distinguish how much of the total effect may be represented by the associated context/spontaneous effects and how much is attributable to the effect of the therapy. In this context, the use of paired samples offers the benefit of controlling extraneous factors that can influence the results.
For the evaluation of the treatment, we used the 25-Foot test. Although assessing gait disability is of great importance in MS, there is no consensus regarding the most appropriate tool. 20,21 In this sense, the results obtained in the present study can support the idea that the T25FW is sufficiently sensitive to changes that occurred as a result of treatment and can therefore be a useful tool as a clinical measure of gait in studies involving acupuncture. This is an important aspect as appropriate outcome measures (objective and measurable parameters) need to be carefully considered to contribute to the credibility of the effectiveness of acupuncture treatments.
With respect to the evaluation of the acupuncture treatments, our results produce evidences that the treatment protocol used for true acupuncture is significantly more effective in improving gait impairment than sham acupuncture. When analyzing the results by gender, it seems that the effect of true acupuncture is stronger in females than in males. In female sample, misbalance and tiredness were the main complaints of female sample, whereas in males we observed more variability.
The review of literature revealed a lack of studies regarding gait and acupuncture in MS. In a review, 22 including all studies that used acupuncture to treat any symptom of MS, fifteen articles were found, and none of them examined mobility measures such as gait. The results obtained in the majority of articles regarding MS symptoms point in general to beneficial effects of acupuncture. Also, in another review concerning the use of complementary therapies in MS, including acupuncture, 23 patients with MS described it as generally relaxing. Reduced pain, increased flexibility, and improved balance were also referred. Nevertheless, not all the studies show that acupuncture had a meaningful impact on MS. This can be explained by the fact that many of the studies are case reports, and others have no randomization, adequate measures, poor statistics, and little use of controls. 22
To our knowledge, this is the first controlled clinical study on the effects of acupuncture on gait problems in patients with MS. Although our results must be interpreted carefully, mainly due to sample size, we found consistent improvement on mobility in patients with MS of RRMS when true acupuncture treatment was used, contrary to what was observed for sham acupuncture.
Conclusions
In summary, our study protocol provides evidence that acupuncture treatment, according to Heidelberg model of TCM, can result in improvements in mobility in MS population. Of course, larger studies are needed to confirm the clinical application and cost-effectiveness of acupuncture treatment, but our results suggest that acupuncture can be an attractive option for intervention for patients with MS with gait impairment symptoms looking for an effective therapy.
Footnotes
Acknowledgments
The authors thank the “Sociedade Portuguesa de Esclerose Multipla” (SPEM) and “Associação Nacional de Esclerose Múltipla” (ANEM) for their collaboration.
This research was partially financed by Portuguese Funds through FCT—Fundação para a Ciência e a Tecnologia, within the Project PEstOE/MAT/UI0013/2017.
Author Disclosure Statement
None of the authors has a financial or property stake in the Heidelberg model.