
Abstract
Objective:
Visceral adipose tissue (VAT) and hepatic fat deposition are the most important risk factors for women's health. Acupuncture, including electroacupuncture (EA), is used to treat obesity throughout the world. The effect of EA is evaluated mainly by body mass index (BMI) and waist circumference (WC). Few studies have assessed its effect in reducing VAT volume and hepatic fat fraction (HFF) based on an exact measurement method such as magnetic resonance imaging (MRI). This study aimed to resolve this issue.
Methods:
Thirty subjects were randomly divided into two groups. The control group (n = 15) did not receive any intervention and maintained a normal diet and their usual exercise habits. The treatment group (n = 15) received EA three times a week for 3 months. BMI and WC were measured using different devices. VAT and HFF were measured by MRI and calculated by related software before and after the intervention.
Results:
A marked difference was evident in group that received EA treatment in the following tests. The differences in BMI (U = 21.00, p < 0.001), WC (U = 40.50, p = 0.002), VAT volume (U = 13.00, p < 0.001), and mean HFF (U = 0.00, p < 0.001) before and after the intervention in the treatment group were distinct and significant compared with those of the control group. Three months later, the treatment group showed a lower BMI (W = 91.00, p = 0.001), WC (t = 4.755, p < 0.001), VAT volume (t = 5.164, p < 0.001), and mean HFF (W = 120.00, p = 0.001) compared with pretreatment levels. Compared with the control group, the treatment group showed a lower VAT volume (t = 60.00, p = 0.029) after 3 months of treatment. After 3 months, the control group showed higher mean HFF (t = −2.900, p = 0.012) and VAT volume (W = 11.50, p = 0.006) compared with their initial levels.
Conclusion:
Based on MRI evaluation, this randomized controlled study proved that EA treatment reduces BMI and WC as well as VAT volume and HFF in women with abdominal obesity.
Introduction
O
Health concerns regarding obesity take into account not just the amount of fat but also its distribution. Visceral fat tissue (VAT), located in the mesentery, omentum, and surrounding internal organs, provides free fatty acids (FFA) and results in fat deposition in the liver. 3,4 This increases the risk of cardiovascular disease, type 2 diabetes mellitus, insulin resistance, and even some cancers such as cancer of the breast, colon, endometrium, and prostate. 5 –11 Although hepatic fat deposition and VAT have different effects on the metabolism, they are closely related to each other. 8,12 –14
Early during the Qing dynasty in China, Fu Qingzhu, a famous gynecologist (1607–1684), indicated that abdominal obesity was associated with female infertility. 15 Many recent research has also suggested that obesity, especially abdominal obesity, is an important risk factor related to several gynecological disorders, including polycystic ovary syndrome, infertility, and menstrual disorders in addition to the above-mentioned diseases. 16,17 Hence, finding a way to control excessive abdominal fat in women is an urgent issue.
Acupuncture, including electroacupuncture (EA), is being used to treat obesity because of its beneficial effect on multisystem regulation, using multiple target points by acupoint stimulation. Many studies have reported that acupuncture has a positive effect on obesity control. 18 –20 However, few emphasized de qi (a special sensation experienced when the needle passes through the acupoint), which is an important concept in Traditional Chinese Medicine (TCM) and has been proven to be one of the most important factors in effect of acupuncture. 21 Furthermore, these studies evaluated the effect of EA on reducing BMI, waist circumference (WC), weight, hip circumference, or biochemical criteria such as blood glucose, total cholesterol, and so on. Few studies have included VAT volume or hepatic fat fraction (HFF), which is in fact the most important risk factor related to obesity.
Obesity is strictly defined as a condition in which there is an excess of body fat. BMI is the tool most commonly used to estimate overweight and obesity, but it does have some limitations. People such as muscular athletes may have a BMI in the obese category, even though they are not by definition obese. In addition, many studies have suggested that abdominal obesity may indicate higher risks of cardiovascular disease and death in women, despite normal weight or normal BMI. 22 –24
The WC is usually used to assess abdominal fat content. Belly fat includes subcutaneous fat and visceral fat inside the abdomen. The WC is more related to the thickness of subcutaneous fat. High visceral fat, however, is a more important determinant of carotid atherosclerosis than subcutaneous fat is, 25 and it is also an independent predictor for the future development of atherogenic dyslipidemia whereas BMI or WC are not. 26
Magnetic resonance imaging (MRI) avoids radiation exposure associated with computed tomography. MRI provides a reliable basis for comparing body fat distribution in different individuals, allowing for a fast and reliable quantification of total body fat and its distribution in different body regions. 27 The improved technique of iterative decomposition of water and fat with echo asymmetry and least-squares estimation quantitation sequence (IDEAL-IQ) and MRI-estimated proton density fat fraction help the imaging of fat grade to be achieved. By measuring the graph, a precise and quantitative evaluation of fat in the region-of-interest (ROI) of the liver can be achieved with a single breath-hold acquisition of about 18 s. 28 These techniques have been applied and been proven as superior methods to obtain VAT volume and to quantify hepatic adipose content in recent studies. 29,30
This study focused on the abdominal obesity in women, and a randomized controlled trial was conducted to examine the effect of EA on reducing VAT volume and HFF as well as BMI and WC based on MRI.
Materials and Methods
Study design and patients
The study was approved by the Human Research Ethics Board at Puai Hospital. Subjects, who were regularly attending the acupuncture specialist clinic of Puai Hospital for weight loss, consented and were enrolled onto the study. Subjects we enrolled who were aged between 21 and 53 years, with a BMI ≥23.0 kg/m2 and WC >80 cm, according to the WHO recommendation based on risk factors and morbidities in Asia, which are lower than the WHO criteria. 31 Obese individuals with known etiological factor such as endocrine disease, heart disease, immunologic diseases, pregnant and lactating women, or other contraindications for MRI were excluded. None of the subjects had received any therapy for reducing weight 3 months prior to the study.
The trial was conducted from January 2014 to February 2016. Of the 40 women screened at the acupuncture clinic, five did not meet the entry criteria. The 35 enrolled subjects were divided into three groups according to their BMI: BMI ≥30 kg/m2, 25 ≤ BMI <30 kg/m2, and 23 < BMI <25 kg/m2). A computer generated a random number for each subject, and odd numbers were chosen for the treatment group and even numbers were assigned to the control group. Thirty subjects completed the whole experiment (Fig. 1). Table 1 lists the baseline data for the two groups.
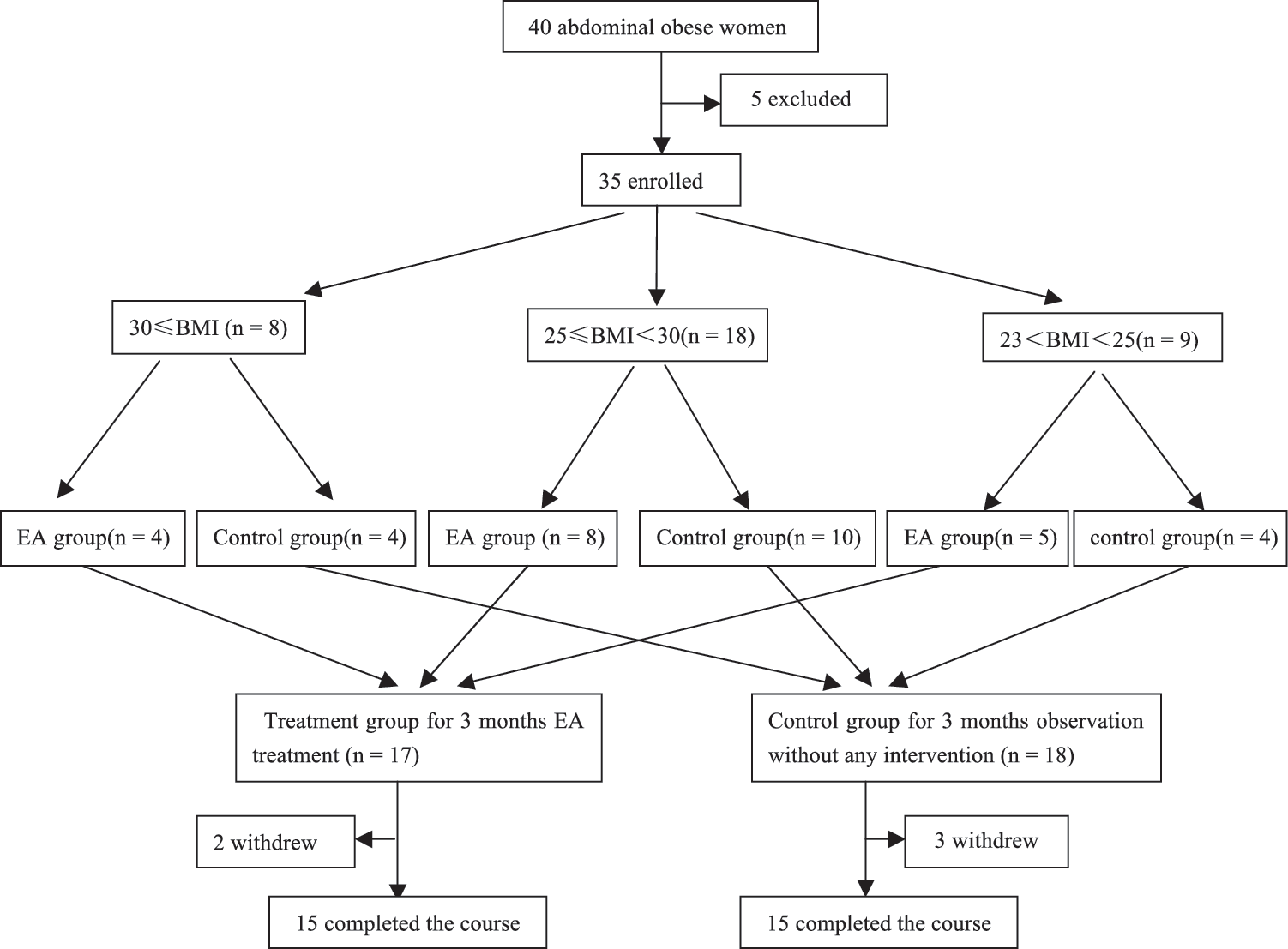
Trial profile and design.
BMI, body mass index.
Treatment group
The standard acupuncture points were chosen based on the theory of TCM and clinical experience. The main acupoints included: on the abdomen—bilateral Huaroumen (ST-24), Tianshu (ST-25), Wailing (ST-26), Shuidao (ST-28), Fujie (SP-14) and Daheng (SP-15); and on both lower legs—Zusanli (ST-36) and Fenglong (ST-40). Additional acupoints were included and selected according to TCM diagnosis and experiences: abdominal region—Guanyuan (RN-4) and Shuifen (RN-9); on lower legs—Yanglingquan (GB-34); on both feet—Neiting (ST-44): and both arms: Zhigou (SJ-6).
The method
Stainless-steel acupuncture needles (0.25 mm × 30 mm; Huatuo brand) were inserted to a depth of approximately 25 mm after skin sterilization (75% alcohol). The needles in the arm and lower legs were manipulated by rotating them back and forth until the subjects felt heavy or sore (de qi) in the area surrounding the acupoints.
The acupuncturist adjusted the top of needles in the abdomen along the reversed direction of the meridian and put the needle body into the fat layer. Needles on the abdomen were connected to an electrical stimulator (Model: G6805-2A; Huayi, Shanghai, People's Republic of China) and were applied with electricity, of which four needles served as the positive pole and the other four as the negative pole to allow the electrical circuit to be set as right Huaroumen (ST-24) to right Shuidao (ST-28), left Huaroumen (ST-24) to left Shuidao (ST-28), right Fujie (SP-14) to right Daheng (SP-15), and left Fujie (SP-14) to left Daheng (SP-15). Electricity was generated as an output of programmed pulse with a voltage of 6 V, a frequency of 50 Hz, and width of 0.5 ms continuous wave. Subjects adjusted the control to a maximal tolerable intensity to obtain the warm response or weak muscle twitch (de qi) in the abdomen during the electrical stimulation.
EA treatment was performed daily for 30 min three times a week for 3 months by an experienced acupuncturist. Special nutritionist follow-up visits were included in the treatment protocol in order to guarantee no reduction in weight due to diet change or exercise.
Control group
The control group did not receive any intervention and kept their former life-style during the study period. Special nutritionist follow-up visits were included in the treatment protocol to guarantee no reduction in weight due to diet change or exercise.
Assessment
The results were evaluated as reductions in BMI, WC, VAT volume, and HFF after 3 months of intervention. Body weight and height were measured on all subjects, with minimal clothing, to the nearest 0.1 kg and 0.1 cm. BMI was calculated as body weight (in kg)/height (in m2).
WC was measured to the nearest 0.1 cm according to the WHO recommended methods. Measurement was taken midway between the inferior margin of the last rib and the crest of the ilium on a horizontal plane.
All subjects were examined on a 3.0 T MRI system (Discovery MR750; GE Medical Systems). VAT was determined by MRI, and HFF was determined by IDEAL-IQ. Both were identified by an experienced radiologist in quantifying VAT and HFF.
MRI acquisition
For all subjects, abdominal MRI examination was performed on a 3.0 T system. A 32-channel torso phased-array coil or HD cardiac coil was used depending on the shape of the body. Three breath-hold axial Lava-Flex sequences and a sagittal breath-hold Lava-Flex sequence were done to estimate fat volume. An IDEAL-IQ (GE Healthcare) was obtained to estimate the HFF. Transverse Lava-Flex imaging was performed using the following imaging parameters: repetition time (TR) 3.7 ms; echo times (TE) 1.1 ms; flip angle (FA) 12°; bandwidth 200 Hz/pixel; matrix 272 × 200; slice thickness 5 mm; field of view 40 cm × 36 cm; scan time 16 s.
Sagittal Lava-Flex imaging was performed using the following parameters: TR = 3.65 ms; TE = 1.67 ms; FA = 12°; slice thickness 5 mm; FOV 40 cm × 40 cm; scan time 13 s.
The IDEAL-IQ sequence was also used for HFF estimate in the axial plane using the following imaging parameters: TR = 5.8 ms; first TE 0.9 ms; last TE 4.4 ms; echo train length = 3; readout echo bandwidth = 111.11 Hz/pixel; matrix = 160 × 160; FOV = 44 × 44; slice thickness = 6 mm; FA = 3°; scan time 18–22 s.
Imaging analysis
Contiguous slices (55–60) of fat phase of axial Lava-flex
32
between the inferior margin of the fourth lumbar vertebra (L4) and the third sacral vertebrae (S3) based on the characteristic of the abdominal fat distribution among Chinese
33
were selected and adjusted for the best contrast between fat and other tissue by the software (Radi Ant DICOM viewer 64-bit; Fig. 2). VAT was extracted from the original image using Adobe Photoshop (Fig. 3). Pixels in each area for each slice were scored as VAT using MATLAB. The VAT volume between L4 and S3 was calculated as follows
29
:
where V is volume, Ai is each scan's cross-sectional area, h is the between-slice interval, t is the thickness of each slice, and N is the number of total slices.
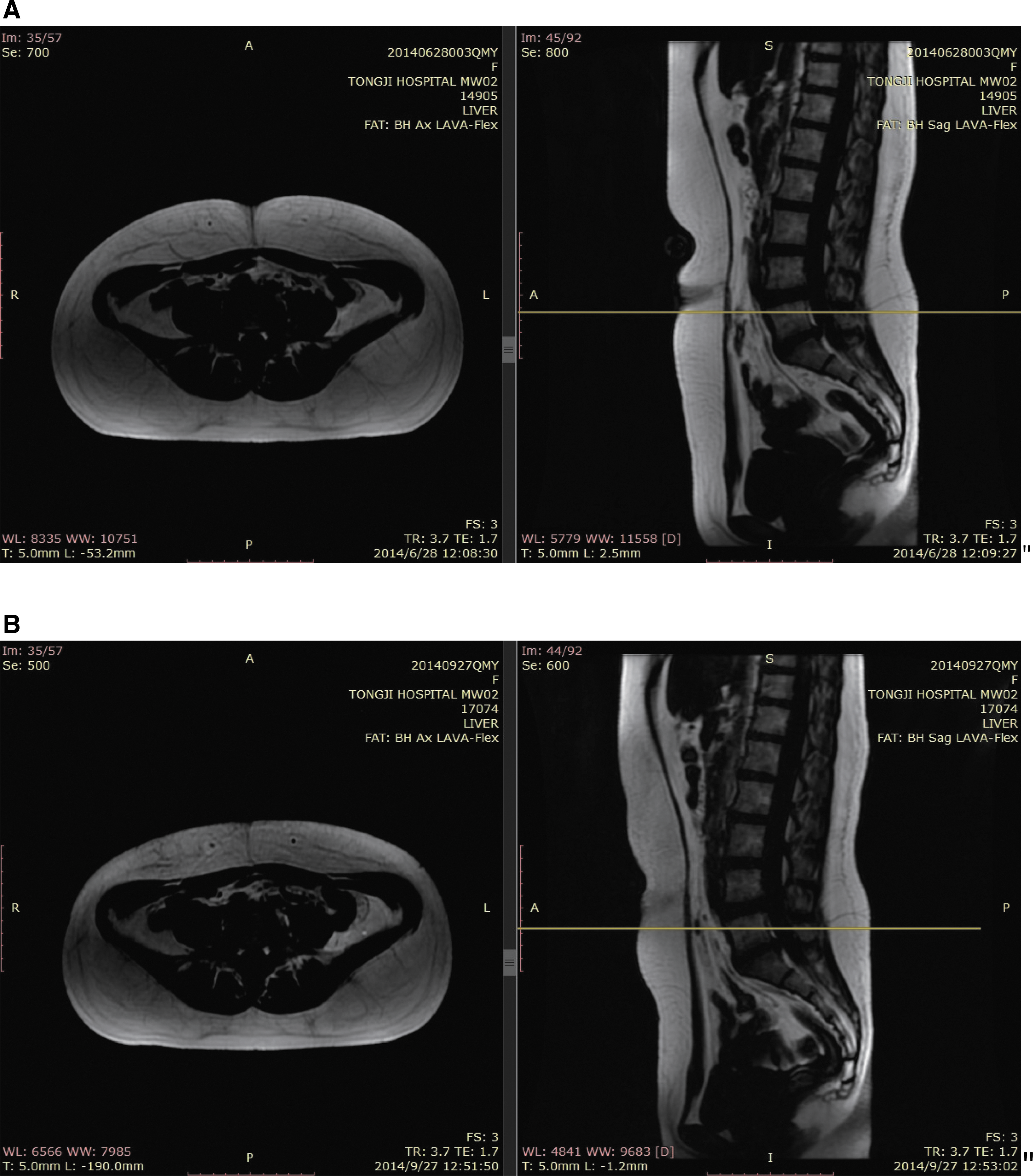
Slices of the fat phase of the sagittal Lava-Flex (right) and the fat phase of the axial Lava-Flex (left) at the upper margin of L5. All fat phases of the axial Lava-Flex were adjusted to obtain the best contrast between fat and other tissue by the software. The white part is fat tissue. Each scan's cross-sectional fat area was analyzed, calculated, and summed using MATLAB. (
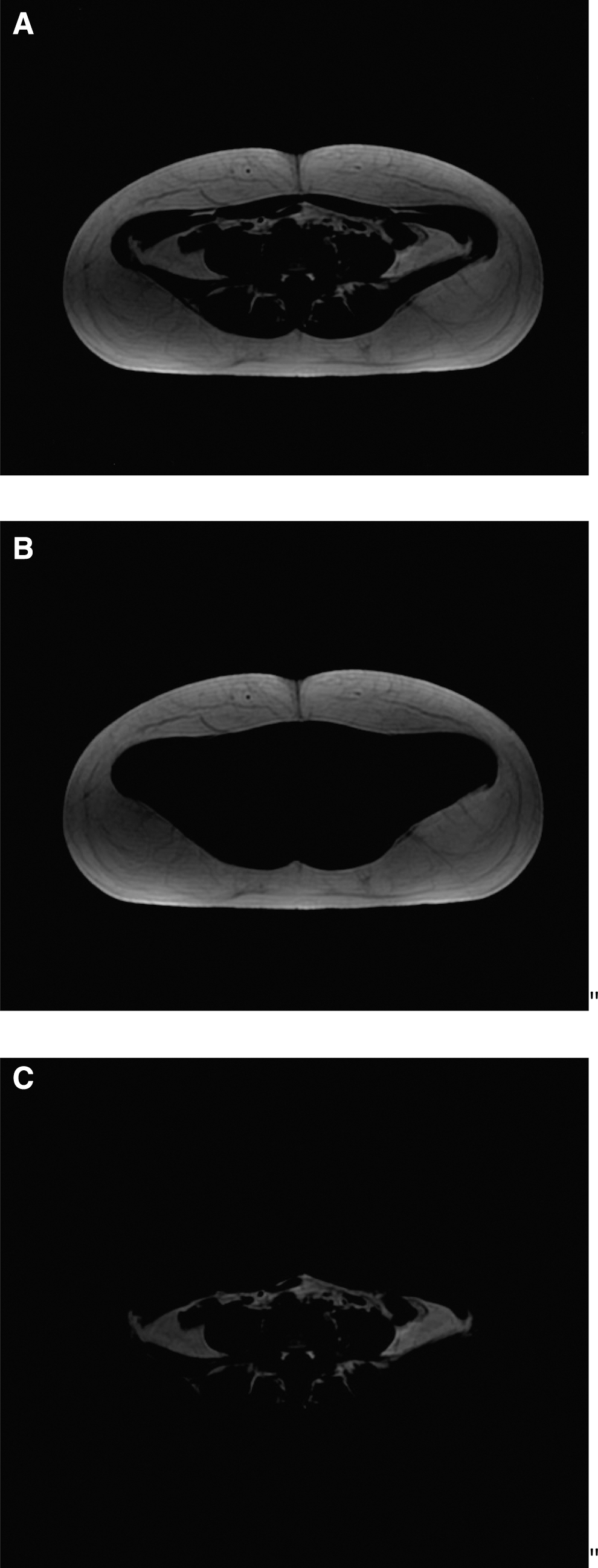
(
To estimate the HFF, a ROI was selected by two observers who were unaware of the patients' clinical information. Hepatic ROIs were defined on Lava-Flex water image series and were mirrored onto the IDEAL-IQ fat fraction images. Three ROIs (ROI1, ROI2, and ROI3) were chosen with the same 300 pixels in the liver avoiding visible blood vessels and artifacts. The measuring software automatically calculates the HFF (%) on each series selected ROI. The mean values of the three parts were averaged for each series (Fig. 4).
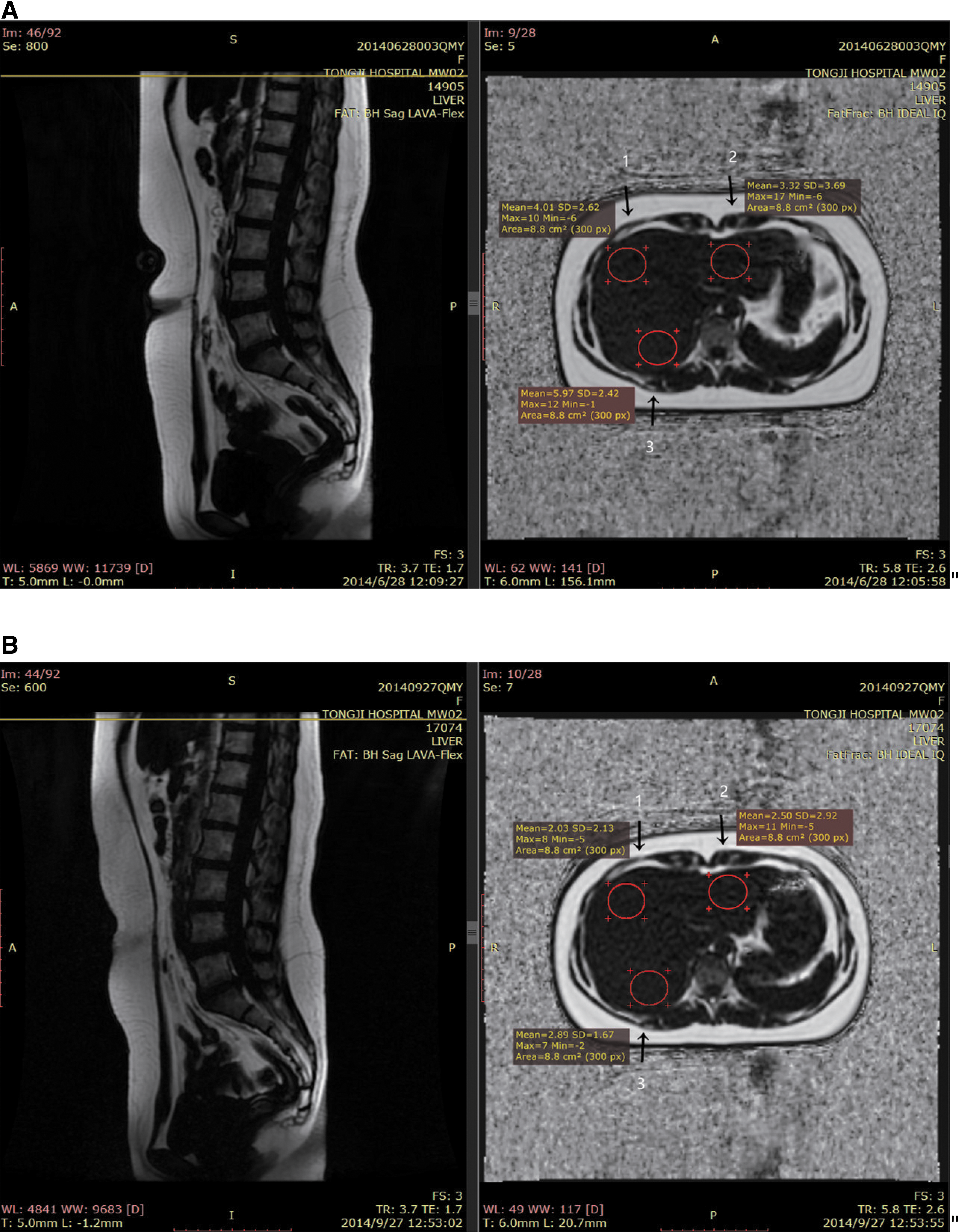
Original fat phase of the sagittal Lava-Flex (left) and fat fraction phase of the IDEAL IQ at an inferior margin of T10 (right). Three circles (arrows 1, 2, and 3) with the same pixels (300px) were the chosen regions of interest (ROI). The software automatically calculated the hepatic fat fraction (HFF; %) in selected areas (ROI1, ROI2,and ROI3), and the mean value of the three parts was averaged for each series ROI. (
Data analysis
All data from subjects who had completed the experiment were included. SPSS Statistics for Windows v21.0 (IBM Corp.) was used for all data analysis. The distribution of the data was tested using the Shapiro–Wilk 34 normality test. Two independent sample t-tests, paired t-test, and nonparametric test (Wilcoxon signed-rank test, Mann–Whitney U-test) were used to detect the effects of EA on obesity. A p-value of ≤0.05 was considered significant.
Results
A total of 30 subjects were included, and there were no significant statistical differences before intervention for the baseline data of age, duration of disease, BMI, WC, VAT volume, and HFF (Table 1 and Fig. 5).
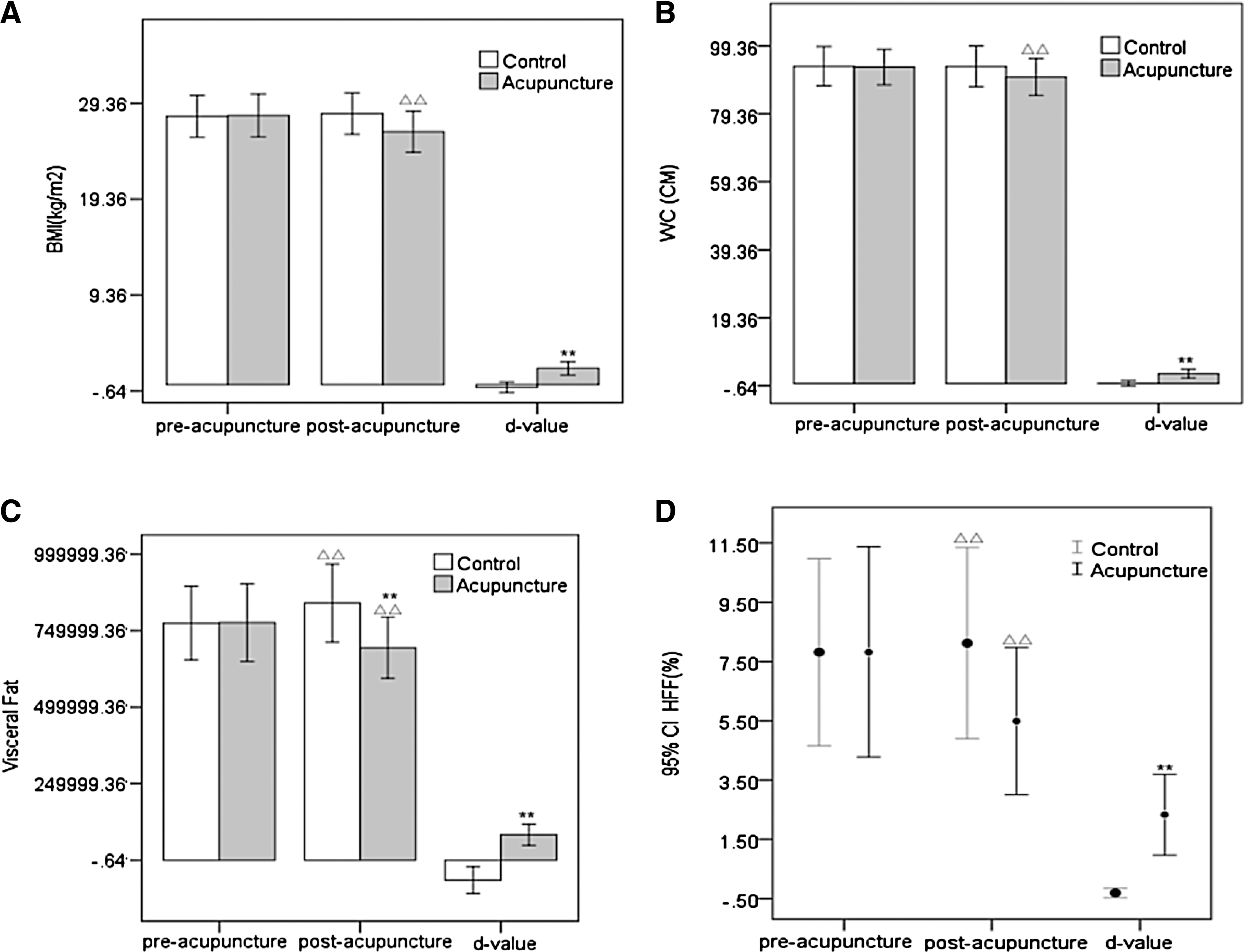
Changes in the two groups before and after the intervention. (**p < 0.01 vs. the control group; ΔΔ
p < 0.01 vs. before the intervention in the same group). (
Three months later, for the treatment group, the difference values (D-values) for BMI, WC, VAT volume, and mean HFF before and after the intervention were noticeably larger compared with those of the control group (Fig. 5). VAT volume reduced more dramatically compared with that of control group (Fig. 5C). BMI, WC, VAT volume, and mean HFF reduced compared with pretreatment levels (Fig. 5). Figure 4 shows the HFF in the different ROIs (ROI1, ROI2, and ROI3) and the mean HFF of a subject before and after EA treatment as: ROI1 4.01 vs. 2.03; ROI2 3.32 vs. 2.50; ROI3 5.97 vs. 2.89; and mean HFF 4.43 vs. 2.47.
For the control group, VAT volume and the mean HFF increased after 3 months compared with pre-observation levels (Fig. 5C and D).
Discussion
An increase in abdominal fat in women brings about serious health risks such as preeclampsia and delayed initiation of breastfeeding, 35,36 which will impact the health of future generations.
Acupuncture is being used to treat obesity worldwide. However, besides BMI and WC, few studies have assessed the effect of EA based on MRI, or have had methodological limitations. 37 MRI is now considered a highly accurate way and the gold standard for measuring VAT, 27 but there has not been a unified evaluation criterion until now. A previous study reported a high correlation between a single abdominal image area at L4–L5 and the total volume of VAT. 29 Most investigators use a single cross-sectional image at several different levels such as the umbilicus, L3, L4–L5, or the mid-lumbar L4 vertebral body (Mid-L4) 33,38 –43 as a surrogate measure of total VAT volume, which is regarded as a compromise between accuracy and cost.
In the present study, subjects completed MRI scans from thoracic vertebra T10 to S5. A total of 55–60 consecutive images between the inferior margin of L4 and S3 were taken as the research area. In the course of image analysis, it was found that VAT was removed and redistributed after EA treatment, and the total volume reduced after treatment. However, some of single-slice fat areas increased. There are limitations in selecting only a single-slice fat area to evaluate the EA effect, which could lead to a false result.
Recently, Zhang et al. 37 reported scanning seven slice areas above and below the hilus of the kidney to a total 15 slice areas, which were summed to estimate the effect of acupuncture. Brown et al. 44 reported that the measurement site for abdominal adipose tissue has a significant influence on the relationships with total VAT in obese adolescents before and after an exercise intervention. A single-slice fat area at any vertebral body level is a compromise for the most time- and cost-efficient method for assessing total VAT volume. It is not, however, a good marker for evaluating the change in VAT by therapy methods such as EA.
For the treatment group, after the intervention, both the D-values of BMI, WC, and VAT volume and the mean HFF were significant compared with those of the control group, and changes in BMI, WC, VAT volume, and mean HFF were observed compared with pretreatment levels (Fig. 5). These results demonstrate that EA treatment is effective in reducing BMI, WC, VAT volume, and HFF. However, compared with the control group, only change in VAT volume, not changes in BMI, WC, or HFF, were obvious after 3 months of treatment (Fig. 5). While collecting the experimental data, VAT volume reduction with no weight or WC change was found in a few subjects. A comprehensive analysis suggested that reduction of VAT by EA treatment might be superior to BMI and WC, which further suggests that no weight or WC change does not mean no VAT reduction.
It is very important that a reduction in VAT, even with no weight change, may result in significant risk reduction. 3,31 VAT reduction with EA treatment is a potentially useful strategy in the prevention of risks in the obese population.
Excess fat in obese individuals damages the ability to take in and store the FFA subcutaneously, increasing fat deposition in the internal organs. EA reduces the VAT volume prior to BMI, WC, and even HFF might be related to the sequence of fat deposition and the smaller density of adipose tissue, but more studies are needed.
For the control group, after 3 months of observation, BMI and WC were unchanged, whereas the VAT volume (Fig. 5C) and mean HFF (Fig. 5D) increased compared with initial levels. These results indicate that the visceral fat and intra-hepatic fat had been deposited earlier than the weight or WC. No increase in weight does not mean no increase in fat. It is important us to pay early attention to a change in VAT volume and HFF than to an increase weight or WC. The risk of fat accumulation on health has possibly is present before an increase in weight.
During the treatment, there was an emphasis on de qi with continuous weak electric current stimulation connected to the acupuncture needles at points (abdominal acupuncture point around the umbilicus), line (abdominal stomach meridian and spleen meridian), and plane (whole abdomen) combining to obtain an intensified qi sensation. The umbilical vein, abdominal arteries, deep lymphatic vessels, and intercostal or lumbar nerves may provide a rich material base for the treatment of abdominal acupuncture. Thus, a further study is needed to clarify underlying mechanism.
Acupuncture is a manual operation performed by acupuncturists who have to be aware of the method applied. Due to the Chinese special diet and patterns, a double-blind design and a suitable control group cannot really be applied in the investigation of acupuncture.
Despite the encouraging results from this study, longer follow-ups after 3 months of experiment and further observation should be continued. The improvement of irregular menstruation and fertility after EA treatment based on a larger sample and better control group should also be investigated.
Conclusions
This randomized controlled study demonstrates that EA treatment is more effective than no intervention in reducing BMI, WC, VAT volume, and HFF. Further study is warranted to investigate EA as an alternative treatment option for BMI, WC, VAT volume, and HFF to control abdominal obesity in women.
Footnotes
Acknowledgments
This work was supported by a grant from the clinical program of Health and Family Planning Commission of Wuhan Municipality, China (WZ14D02) to Hong Lei. We thank Dr. Guangying Huang, Dr. Daoyu Hu of the Tongji Medical College, and Dr. Lixing Lao of the University of Hong Kong for their critical reading of and comments on the manuscript. We also wish to thank Chaojie Li of the Swiss Federal Institute of Technology Zurich (ETH Zurich) and Tongchen Feng of the University of Saskatchewan, Saskatoon, Canada, for English editorial assistance. We also thank Dr. Christopher Chinna, a retired general practitioner from the United Kingdom for English editing.
Author Disclosure Statement
No competing financial interests exist.