
Abstract
Objective:
To summarize and evaluate evidence for the effect of yoga on menstrual disorders.
Methods:
PubMed, CINAHL/MEDLINE, Web of Science, AMED, and Scopus were searched for English-language literature relevant to the review question. All primary research studies were included.
Results:
Fifteen studies described in 18 papers were included in the review. A range of yoga interventions were used. Some studies used a combination of Asana, Pranayama, and other yogic relaxation or meditation techniques. All included studies reported some change in their outcome measures, suggesting reduced symptoms of menstrual distress following a yoga intervention; however, the heterogeneity and intensity of the interventions and outcome measures meant that findings have limited generalizability and applicability in practice settings.
Conclusions:
Further research on the relationship between yoga practice and menstrual disorders is warranted, but there must be both consistency in the methods, measures, and quality of studies and a shift toward research on yoga practices that are replicable outside of the clinical trial setting.
Introduction
T
Background
Yoga is a term used to describe a variety of practices, although its literal translation in Sanskrit means “yoke” or “union.” 10 Yogic practices may include physical exercises (Asanas), breathing exercises (Pranayama), relaxation techniques, and meditation or concentration practices, including yoga Nidra (a form of guided relaxation practice). There are many different types of yoga, according to different schools or traditions (for example the Asana-heavy styles of yoga practiced often in the West according to the teachings of three pupils of Krishnamacharya (1889–1989): the school of BKS Iyengar, 11 Ashtanga Vinyasa yoga of Patthabi Jois, 12 and the Viniyoga of Desikachar 13 ). Yoga practice in the modern context is primarily focused on Asana as a physical exercise regimen, whereas traditionally, and certainly before the mid-20th century, yoga has been more widely associated with spirituality and contemplation, with Asana practice being a less prominent aspect. 14
Research on yoga as a therapeutic intervention grows apace, 15 –17 although the variability in study quality, interventions, and outcome measures means that the extent to which yoga practice may positively affect health cannot yet be definitively stated. 15,16 The mechanism by which yoga may improve health is commonly considered to be its effect on the autonomic stress response. 18 Yoga-based practices affect a complex series of physiologic and cognitive mechanisms, which in turn may affect aspects of self-regulation of stress. 19 –21
A recent attempt to define a comprehensive theoretical framework from which hypotheses on how bottom-up neurophysiologic and top-down cognitive mechanisms may explain the effect of yoga on well-being has differentiated between the effects of the movement, breath and attention aspects of practice. 19 It has also differentiated between several neurologic and physiologic processes that may be involved in self-reported changes in the well-being of yoga practitioners. These include the effect of yoga movement on the basal ganglia and cerebella circuits; the influence of yoga breathing practices on concentrations of oxygen and carbon dioxide in the blood; and the effect of the attention element of practice, akin to other meditative activities, on structural changes in parts of the brain responsible for bodily awareness.
Alongside the exponential increase in yoga research, there has been “a parallel surge” in yoga practice. 16 Demographic surveys of yoga practitioners in the United States have found yoga practitioners to be more likely to be white, female, highly educated, and middle aged. 22,23 As well as the trial-based evidence showing that yoga may positively affect health, in particular the psychology and physiology of stress, there are practical benefits to suggesting yoga as an intervention for menstrual disorders: It is not costly, requires no equipment, and is readily available (there are classes in most cities, and yoga tutorials are available online). A recent meta-analysis of clinical trials found yoga to be as safe as usual care or exercise. 24
A relationship between yoga Asana practice and menstrual disorder symptoms has been established in both the nonacademic popular literature and in yoga manuals. In the grey nonacademic literature (namely, the plethora of yoga websites and magazines and mentions of yoga on health and well-being websites), there is evidently an association between frequent yoga practice and oligomenorrhea, and the possible effects of yoga on menstrual disorders (a Google search of “yoga AND menstrual disorders” yielded about 340,000 results on November 6, 2016, and a search of “yoga AND oligomenorrhea” yielded about 36,000 results on November 6, 2016).
Commonly in yoga manuals and instructional articles, women are advised to refrain from certain Asanas, such as the inversion postures Sirsasana (headstand) or Sarvangasana (shoulder stand) during menstruation, 25 whereas in the Ashtanga Vinyasa tradition of Patthabi Jois, 12 women are advised to refrain from Asana practice in the first 3 days of menstruation off from practice. 26 Popular yoga manuals offer women specific sequences to be undertaken during menstruation. For example, Geeta Iyengar's Yoga: A Gem for Women 27 recommends a sequence including Upavistha Konasana and Baddha Konasana to ease dysmenorrhoea, and Judith Hanson Lasater offers a sequence for menstruating women in The Moon Club: Honouring the Monthly Cycle, 28 which aims to assist the body in releasing menstrual flow, reducing fatigue, and moderating hormonal shifts. Like Iyengar, her sequence is based around versions of Baddha Konasana and Upavistha Konasana. The sequence of postures recommended for menstruation on the online Yoga Journal site 29 include Baddha Konasana, Dhanurasana (the bow), Setu Bandha Sarvangasana (bridge pose), Ustrasana (the camel), dolphin, and Adho Mukha Svanasana (downward dog). The PopSugar lifestyle site article “Skip the Ibuprofen and Do These Yoga Poses to Ease Period Pain” 30 suggests a “half bound squat” (Malasana), arching pigeon (Kapotasana), one-armed camel (Ustrasana), a wide child's pose (Balasana), and a reclining twist, although the first three of these poses are rather advanced and would probably not be taught in a beginner's class.
The aim of this review was to assess the evidence for correlations between yoga practice and various forms of menstrual disorder and to identify which forms of yoga have been evaluated as interventions for menstrual disorders. The review also aimed to evaluate the published primary research evidence for the efficacy of yoga as an intervention for treating menstrual disorders. Does published research evidence accord with yoga wisdom, as reflected in journals, websites, and instruction manuals?
Methods
This study was a systematic literature review of primary research on the effect of yoga on menstrual disorders. A search was conducted of the English-language literature between 1996 and 2016. The following databases were searched: PubMed, CINAHL/MEDLINE, Web of Science, AMED, and Scopus. The following search terms were used: “Yoga AND menstruation OR menstrual period OR menarche; Yoga AND amenorrhea; Yoga AND dysmenorrhea.” Studies were included if the following criteria were met: primary research, on premenopausal women, and undertaking yoga practice. Studies were excluded if their participants were menopausal women, if yoga was not the intervention being undertaken. and if the study did not consist of primary research. This study aimed to comprehensively review all research literature on the effect of yoga on menstruation, not just evidence from randomized controlled trials (RCTs), so all types of primary research study were included.
One reviewer reviewed each paper by using a standardized data extraction form. Extracted data included authors, year of publication, sample size, interventions, main outcomes, and adverse events. The data extraction process is detailed in Figure 1.
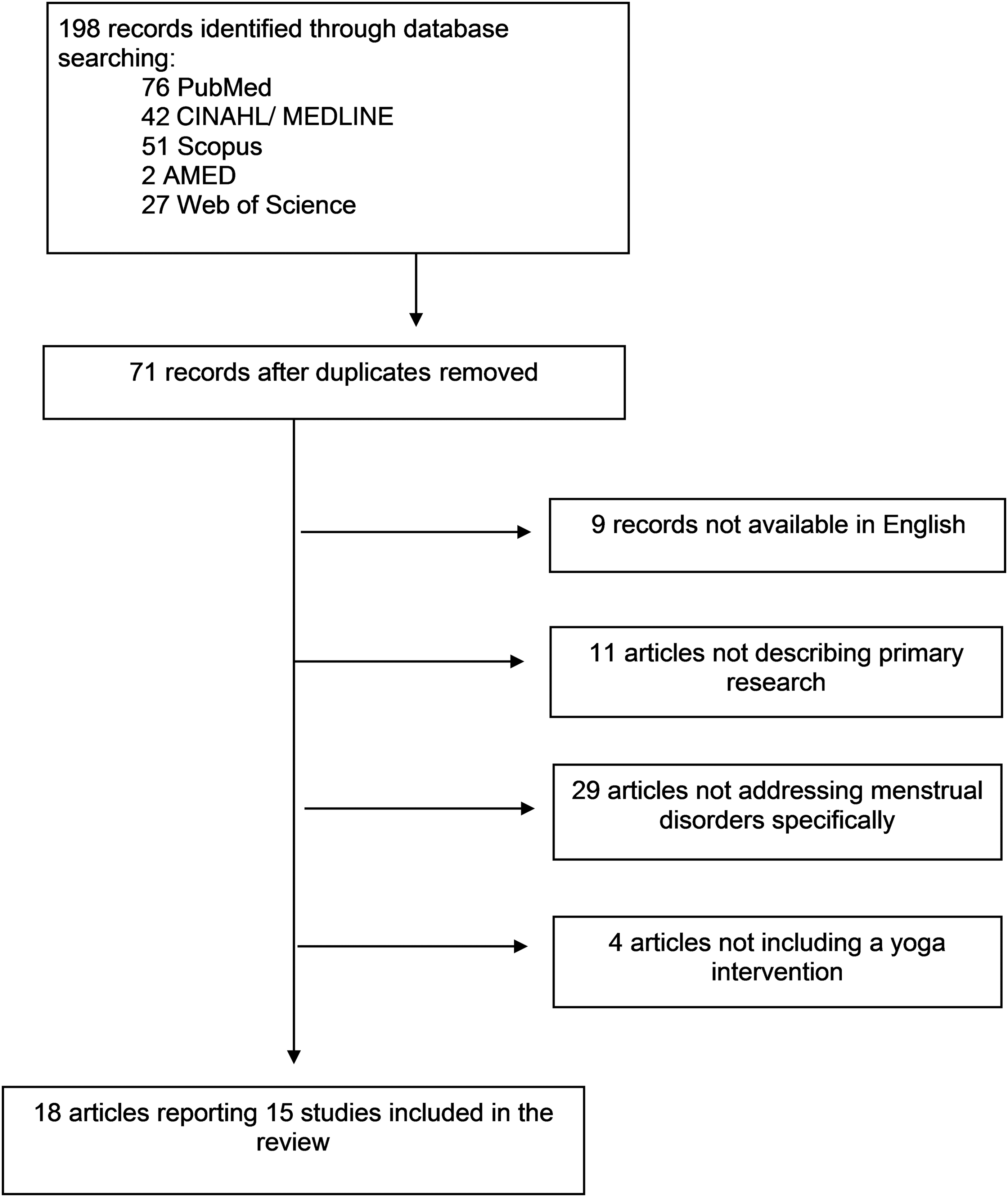
Flowchart of the results of the literature search.
The methodologic quality and risk of bias of the included studies were measured by using the Critical Appraisal Skills Programme (CASP) criteria 31 and the Cochrane Handbook for Systematic Reviews of Interventions (version 5.0.2). 32 The following domains of bias were reviewed: random sequence generation, allocation concealment, blinding of participants and personnel, incomplete outcome data, selective reporting, and other sources of bias.
Results
Fifteen studies described in 18 papers were included in the review. The year of publication, authors, study design, sample size, age of participants, intervention modality, intervention dosage, outcome measure, and salient findings for each study are reported in Table 1. Three were case-control trials comparing women with menstrual disorders and healthy women. Nine studies were RCTs. Three were intervention studies. Eight studies were conducted in India; three were conducted in Taiwan; and one each was conducted in Iran, Japan, and Korea. The included studies measured the effect of yoga on premenstrual symptoms and menstrual distress. No studies measured the effect of yoga on amenorrhea or oligomenorrhea. No studies measured the effect of yoga on menstruation in women who were regular yoga practitioners.
MDQ, Menstrual Distress Questionnaire 51 ; RCT, randomized controlled trial; WHAQ, Women's Health Assessment questionnaire (original source not given by Choudhary and Mishra 40 ); QoL, Quality of Life scale (original source not given by Ganesh et al 42 ); PSS, Perceived Stress Scale 57 ; LH, luteinizing hormone; FSH, follicle-stimulating hormone; BMI, body–mass index; VASP, Visual Analogue Scale for Pain 52 ; TSH, thyroid-stimulating hormone; GHQ30, General Health Questionnaire (Japanese version) 58 ; SF-36, Short-Form Health Survey 59 ; EEG, electroencephalography.
Participant characteristics and recruitment
The age range of female participants in the studies varied between 13 and 45 years. In two studies, participants were adolescent girls who attended residential colleges. 33,34 Other studies recruited participants through referral from and attendance at gynecology clinics, 35 –40 on students at a metropolitan college, 41 students on a physiotherapy course, 42 female volunteers with no stated specific origin, 43 unmarried medical students, 44 students, 45 nursery and kindergarten teachers, 46 staff and students at a university, 47 female workers at an electronics factory, 48 college students, 49 and nursing college students. 50
Interventions
A range of yoga interventions were used. Some studies used a combination of Asana, Pranayama, and other yogic relaxation or meditation techniques. Two studies 35 –39 measured the sole impact of Yoga Nidra practice. One study 46 measured the effect of three specific yoga Asanas (cobra, cat, and fish). In other studies, a range of Asana were practiced. The length of the yoga practice sessions differed between studies, from 10 minutes 42 to 90 minutes. 40 Frequency of practice ranged from daily for 16 weeks 40 to 20 minutes for 14 days. 45 In one study, 46 participants were taught the Asana routine and then given a DVD to use for home practice. In the other studies, instruction was provided in a class setting. One study 42 compared the efficacy of two Pranayama techniques. In another study, 34 the control group undertook nonyogic exercise, breathing and resting at the same time as the yoga intervention group. The control groups in the other RCTs and case-control studies did not take part in a control intervention.
Outcome measures
There was little consistency between studies in the outcome measured used. Some studies used versions of the Moos Menstrual Distress Questionnaire (MDQ); 51 others used pain scales, primarily the Visual Analogue Scale for Pain 52 and general quality of life and stress scales (Table 1). Mood scales and mental health scales were also used. In some studies, physiologic assessments were used as objective measures of impact and to identify underlying mechanisms for the potential effect of yoga on menstrual distress. These included the use of resting electrocardiography, body mass index, hand grip and reach tests, autonomic function tests, and serum levels of hormones at certain points in the menstrual cycle.
Findings
All studies reported a beneficial effect of yoga as an intervention for menstrual disorders. Yoga practice was associated with lower MDQ scores, 41,50 lower serum homocysteine, 41 lower negative affect, 40 reduced pain scores, 42 –44,48 increased well-being scores, 38,43 autonomic system changes, 33,35 –37 a heightened relaxation response, 47 and decreased menstrual disorder symptoms. 48 No study concluded that yoga had no effect on menstrual disorder symptoms.
Only one study 38 reported an adverse effect of the yoga intervention; namely, one participant dropped out because of “nonrestorative sleep” following the yoga Nidra practice. Only three studies confirmed no adverse effects of the practice (because of reporting of the included studies). 40,45,49 In all other studies there was no mention of adverse effects or affirmation of their being no adverse effects.
Quality of studies
The quality of studies was assessed by using CASP criteria. 31 All studies gave clear statements of their methods and aims. Recruitment strategies, data collection, and analysis methods were stated. Two studies 39,40 did not state that it had been approved by an ethics committee or institutional review board. All studies described the use of appropriate statistical analysis techniques.
While the research methods and aims were replicable, description of the yoga intervention used varied, limiting the replicability of the intervention in future research. Most studies described the specific Asana used in their intervention, with the exception of Nidhi et al. 34 and Sakuma et al. 46 The studies focused on Yoga Nidra as an intervention 35 –37,39 did not give detail of how Yoga Nidra was instructed or performed. There was limited discussion of the rationales for the specific Asana and Pranayama chosen for the interventions.
High risk of bias was identified in three studies 33,40,48 (Table 2) due to high attrition rates, lack of description of randomization methods, and sole use of subjective self-report methods to measure outcomes. Given the nature of the interventions, it was not possible to blind participants to their allocation or the intervention. Where several studies used self-report measures, such as pain analogue scales, there was a risk of bias in outcome assessment.
NA, not available.
While all studies reported some positive effect of yoga on menstrual distress, as reported by participants and as found by assessing physiological correlates of menstrual distress, the external validity of the studies is limited by the frequency of the interventions used, with daily practice under instruction being an unrealistic expectation of most working-age women. This concern has also been raised in a review of yoga for menopausal symptoms. 53 No studies included long-term follow-up, meaning that the continued effect of the intervention was not measured.
Discussion
Yoga is a term used to describe a range of practices, following a number of traditions of schools. 10 The findings of this review mirror those of systematic reviews of yoga for other health conditions, in that the positive outcomes of individual studies must be countered by concerns about their lack of replicability and their heterogeneity. 12,48,49 Yoga practice is growing exponentially, 24 particularly in the population most likely to experience menstrual distress: women of childbearing age.
The complex mechanisms by which yoga practice may affect the person cognitively and physiologically, with an assumed impact on the stress response, have been noted earlier. 19 –21 The effect of yoga specifically on the underlying mechanisms of menstrual disorder is therefore hard to determine here. The reduction of menstrual disorder symptoms (as reflected in pain or well-being scores) may be due to a generic effect of yoga on pain tolerance and stress reduction, rather than an impact on underlying causes of menstrual disorder, such as hormone imbalance, for example.
While the studies did discuss the possible and previously trialed benefits of yoga, there was no rationale for the specific regimens that were followed: neither the sets of postures used in the interventions nor the duration and frequency of the intervention. In the studies that used a limited and specific practice, for example, Yoga Nidra 35,36 –39 or the comparison of two types of Pranayama ,42 there was not a justification for these practices over others in the yoga pantheon. The exception is Rakhshaee and colleagues' study 45 using three specific poses. Their use is justified because of the action of the cobra pose on spinal flexibility and muscular strength, the cat pose on movement and breath coordination, and the fish pose on relief of stiffness and improvement of flexibility. The mechanism by which these proposed effects address menstrual disorder requires further inquiry, however.
All included studies reported some change in their outcome measures suggesting reduced symptoms of menstrual distress following a yoga intervention; however, the interventions and outcome measures used varied considerably. Several studies documented the effect of intensive programs of daily yoga that may be difficult to sustain outside of the college or industrial settings of the studies, whereby the same groups of women could be present in the same place for several days in a week. Among the 18 studies there was limited parity of intervention or outcome measure. Most studies measured the effect of yoga on an intervention group with no prior experience of yoga practice, meaning that the influence of yoga on menstruation over the long term or in regular practitioners was not gauged. Frequency of practice is a predictor of good health and high subjective well-being in established practitioners; 22 however, the regimens described for yoga novices in some studies in this cohort were particularly intensive. 33,34,40,43,44 There is scope for future research that both controls for the effect of frequency and duration of practice on menstrual disorders and explores the specific influence of frequency and duration.
Another main methodologic drawback is lack of comprehensive reporting of trial methods and heterogeneity of interventions, as has been identified in reviews of yoga for depression, 54,55 weight management, 56 and menopausal symptoms. 53 A recent comprehensive review of research on yoga 2010 to 2016 concluded that RCTs should compare yoga to other forms of exercise and that physiologic tests to identify underlying mechanisms should be used rather than self-reported measures. 15 Recent systematic review and meta-analyses of yoga intervention studies for physical and mental health conditions have also called for a more sophisticated approach, whereby aspects of the practice and characteristics of different practitioners are explored.
Strengths and weaknesses
This was the first systematic review of studies of yoga and menstrual disorders in women of childbearing age, including RCTs. A limitation of this review was the lack of eligible studies and lack of similarity between studies. Another limitation was the restriction to English-language studies. There was no research available on amenorrhea and yoga or oligomenorrhea and yoga. Evidence from yoga manuals, Internet searches, and the nonacademic literature suggests that the effect of yoga practice on menstrual disorders may well extend beyond it being a possible treatment, and that frequent practice may be implicated in the genesis of menstrual disorders as well as potentially relieving them. Such a relationship has not been explored in primary research.
Implications for further research
The results of the studies included here suggest that further research is warranted. There is a need for consistency of measurement and intervention in studies of the efficacy of yoga for menstrual disorders. Long-term follow-up should be included in research designs. The effect of different aspects of yoga practice (Asana, Pranayama, Yoga Nidra, relaxation, and meditation) as well as the different styles of yoga should be compared, rather than treated as one intervention. Yoga interventions should be designed to be realistically followed by working-age women so that they may be generalized to the wider population. There have been no studies in this field on western women. No baseline studies have measured the presence of menstrual disorders in regular yoga practitioners. Of particular interest is the extent of amenorrhea or oligomenorrhea in frequent practitioners of the more strenuous forms of yoga, such as Ashtanga.
Future studies should follow rigorous reporting and methodologic standards, meaning that their design should address risks of bias, particularly in randomization, outcome measures used, and reporting bias. The challenge of allocation concealment and blinding of participants should be acknowledged.
Conclusion
This systematic review found several studies presenting evidence for the effectiveness of yoga as an intervention for symptoms of menstrual disorder. The lack of consistency in the interventions and outcome measures used precluded meaningful meta-synthesis. No studies have looked at the long-term effects of yoga practice on menstrual disorders or the prevalence of menstrual disorders in long-term yoga practitioners. The results of this review suggest that further research on yoga for menstrual disorders is warranted, so long as both methodologic standards are met and the study design enables generalizability to the target population.
Footnotes
Author Disclosure Statement
No competing financial interests exist.