
Abstract
Objectives:
This study explored the models of services and experiences of coordinators and directors engaged in providing complementary and alternative medicine (CAM) or integrative medicine (IM) in oncology centers throughout Australia.
Design:
Fourteen leaders of IM programs from ten systematically selected Australian oncology centers were interviewed. Participants described their center's service model. Interview transcripts were thematically analyzed to identify underlying themes. Results were merged using the matrix technique for triangulation.
Results:
Ten oncology centers were reviewed. IM was perceived in the context of supportive care and wellness. IM program types provided included the following: body–mind programs (56%); body–energy programs (23%), and body programs (21%). All programs were outpatient focused, generally did not require a doctors' referral, were freely accessible to cancer patients and carers at no or minimal cost, were centralized by coordinators, and involved volunteers, nurses, allied health practitioners, third parties, and patients in their treatment planning. Interaction between medical and CAM/IM teams was limited and tended to be informal. The underlying structure comprised four main themes: cultural context, human components, systematic components, and resource availability. Human components and resources were considered important in influencing cultural context and systematic components in the IM structure.
Conclusion:
Australian integrative oncology models are based on the concept of wellness and individualized care, focused on patient empowerment and engagement. IM models are generally independent of conventional medical care. Building relationships and trust between stakeholders and open collaboration with conventional medical care will be important to integrate IM into the hospital system. Systemic changes to deliver patient centered care in the provision of IM healthcare will facilitate the incorporation of CAM and IM into cancer services in hospital settings.
Introduction
C
In Australia, 69% of people have used at least one form of CAM in the past 12 months. 4 Overall, 65–75% of cancer survivors have used at least one form of CAM therapy, 5 generally to support conventional treatment. 6 Many did not tell their physicians, and many physicians did not ask about CAM use. 7,8 In Australia, the majority of private health insurers offer rebates for CAM therapies, resulting in increased numbers of people accessing these services. 9,10
Use of CAM in people treated for cancer has been cautioned against due to its perceived risks and potential for adverse clinical effects 11 ; in particular, possible interactions between conventional and CAM treatments. 12,13 Furze et al. argued that CAM/IM may aid treatment tolerance, distress, and physiologic aspects of care, and increase patient empowerment by increasing motivation and understanding of their illness. They reported positive experiences of cancer patients using CAM and stressed the importance of listening to patients' opinions and perspectives on CAM. 3
The Australian Senate Community Affairs References Committee reported that the high prevalence of CAM use should not be ignored by health professionals. 12,14 It emphasized the need to educate physicians about CAM and to facilitate dialog between patients and health professionals by making CAM information easily accessible. Despite this, there is no formal policy for the integration of CAM into cancer care in Australia. 12
The aim of this study was to investigate the models of care, and examine the coordinators' or directors' perspectives on delivering IM services in oncology settings.
In this study, supportive care is defined broadly embracing CAM, allied health services, social support, and cancer education. IM refers to the incorporation of CAM into conventional medical care, and integrative oncology is the term for IM practiced in oncology hospital settings.
Methods
Study design
The authors used a convergent mixed method 15 approach to comprehensively explore the IM models underpinning CAM services associated with Australian cancer centers. Data were collected via a structured survey and a semistructured interview.
Study participants and procedures
The authors scoped the services available in Australian hospitals identified as having oncology/hematology departments (n = 124) in the Australian Hospitals and Aged Care Databases (2014) to report the availability of CAM services. 16 Ten centers providing IM, CAM, and supportive cancer care or wellness programs were identified, which had established CAM programs within the hospital or affiliated center (Table 1).
In No. 10, St. John of God Subiaco and Sir Charles Gardner hospitals are considered to be one IM centre as run by one organization, Solaris Care.
IM, integrative medicine.
The primary investigator (J.L.V.) invited the senior coordinator of the selected centers by e-mail to participate. Administration of the survey and in-person interviews took place between July and December 2015, during site visits, when information brochures were collected and observational tours undertaken. Interviews explored participants' views regarding their conceptualization of CAM/IM integration and factors associated with operating an IM program. Interview data were audiorecorded and transcribed verbatim. Interviewer/observer reflections were documented after each visit and formed part of the material for analysis. The study was approved by the University of Sydney Human Research Ethics Committee. All participants provided written consent.
Data analysis
Interview data were entered into HyperRESEARCH 3.7.3, and two authors (H.M.D., E.L.) conducted initial coding based on the code framework developed in a previous study evaluating international centers (Table 2).
IM, integrative medicine.
The framework consisted of structure, process, and outcome, 17 depicting the IM models. The framework was applied to the data using thematic analysis phases 3–6 as described by Braun and Clarke. 18 The quantitative survey data were analyzed numerically and synthesized into narrative codes. The datasets were merged using the matrix technique, 19 following the seven phases of the mixed method analysis process. 20
Results
Demographics
Table 3 describes the demographics of the 10 participating centers and 14 interviewees. All centers were established between 1993 and 2015, with most opening between 2010 and 2015. The interviewees' professional backgrounds varied, with the majority being allied health professionals and nurses: 11 were program coordinators, 3 center directors, and 12 provided CAM consultations and/or supportive educational programs.
Interview dates: July to December, 2015.
CAM, complementary and alternative medicine; GP, general practitioner; IP, integrative physician.
Survey results
Table 4 describes the programs run in each center. These were categorized according to Tataryn's medical practice paradigms. 21 The number of programs varied between 9 and 18, with most centers focusing on body–mind programs (56% of all programs).
Body–mind paradigm assumes that social support and psychologic coping style can influence the formation of health and disease (e.g., psychotherapy, meditation, support groups, relaxation therapies, counseling).
Body–energy paradigm assumes that health and disease are functions of the flow and balance of life energies (e.g., acupuncture, reiki, and homeopathy).
Body paradigm assumes that biological mechanisms are the primary causative agents of health and disease (e.g., diets, supplements, exercise, and physiotherapy).
Table 5 describes the results of the survey, exploring the level of integration of CAM/IM into cancer services, including service model structures.
MDT, multidisciplinary team; N, no—“no answer” or “not sure” is not included; P, partial—(Applied only to limited extent, or not systemized but informally done); Y, yes.
More than half of the centers were affiliated with a third party. IM centers were located either in the hospital (n = 4) or within the hospital grounds (n = 6). Four centers provided IM services for inpatients; mainly limited to music, massage, or acupuncture.
Four centers provided acupuncture service, mostly for outpatients. The CAM services were easily accessible to patients and family members, with IM services offered free or at subsidized cost (nine centers). Where costs to patients were incurred, most of the programs were reimbursable through Medicare (under Enhanced Primary Care Plans) or private health insurance. Six centers were funded through a mix of institutional funds and philanthropic fundraising, with most CAM programs relying on nongovernment grants or volunteer services.
None of the centers had written treatment protocols for individual CAM treatment. One center had a protocol for training volunteers. Three centers reported relying on individual practitioners' own practice experience. All centers incorporated service evaluation, most commonly an assessment of patient satisfaction, but indicated that a more systematic evaluation process is required.
The majority of centers had a systematic credentialing process for CAM/IM practitioners. This included a national registration board (where available), clinical experience, formal qualifications, and hospital orientation. Internal training was largely informal through peer interactions.
General practitioner (GP) and integrative physician (IP) were rarely involved in team meetings: except for two centers where acupuncture was provided by a GP and CAM consultation by an IP. Allied health practitioners (AHPs) provided CAM services, filling a dual role (allied health and CAM programs) (n = 3), and delivered supportive educational programs (n = 6). Six centers did not require GP/oncologist referrals: one required referral for allied health programs, two for exercise programs, and one for inpatient acupuncture. Patients generally self-referred to programs (n = 8), often guided by a central coordinator.
At four centers the CAM medical record was generally not shared with medical staff, and CAM practitioners had no access to the hospital medical record. Two centers shared information through the hospital's electronic medical record. Three centers recorded individual's treatment in a paper-based system and provided only rudimentary information to medical staff when required.
Involvement in multidisciplinary team (MDT) meetings with the medical team was limited to coordinators, AHPs, or CAM practitioners who provided inpatient services. Two centers organized supportive care MDT meetings, but reported these to be informal and more focused on general medical treatment than CAM services. Communication with medical staff was managed through a care coordinator/nurse at six centers. Six centers handled interactions between CAM practitioners informally through e-mails or occasional social meetings.
Seven centers provided ongoing educational activities for public/patients and/or medical staff. Education sessions for patients/general public were workshops, public fora, and provision of higher education courses primarily for AHPs engaged in IM services. The sessions include lectures on understanding of CAM and how it can support cancer patients, a tour of the IM center with provided CAM program information for medical staffs to inform their patients about CAM. Those centers were actively involved in CAM research within their center or were in collaboration with other academic researchers.
Three centers reported having no academic activities due to low clinician interest.
Interview results
In applying the coding framework to the Australian interview data, four of the themes listed in Table 2 were emphasized in interview results.
Cultural context
IM was considered to be individualized and able to support the whole person across physical, psychologic, spiritual, and social domains. All interviewees emphasized the importance of adhering to a complementary model of care, rather than alternative medicine models. Interviewees preferred the term “supportive care” to IM or CAM, reflecting their perception of these services within the conventional medicine model of care and the role in ongoing care and recovery of patients beyond the acute cancer period.
Flexibility and adaptability were identified as important components of service delivery. The ability to offer appropriate services at different times in the patients' disease trajectory was seen as important in individualizing care to patient needs. Peer support, social connection, sharing information, and care for the individual within the hospital environment were highlighted as important.
Interviewees indicated that their hospitals had shifted to a greater acceptance of IM, within the concept of wellness. This was perceived as stemming from medical staff, better understanding patient's IM experience after receiving feedback about it directly from patients. Interviewees reported that IM should be preventive or promoting health, rather than focusing on disease, with a broader approach to cancer or chronic illness management. All centers valued the role of IM in empowering patients, giving them choice and control over health decisions. Four interviewees placed a high value on patient experience or feedback.
Two interviewees believed that medical paternalism and hierarchical scientific evidence did not constitute patient empowerment, while three signified the importance of scientific evidence for better quality control of CAM, and convince conventional medicine practitioners to change their perception of CAM.
AHPs and nurses were very involved in the centers, including practicing CAM and running programs/centers; thereby bridging the two medical paradigms. CAM/IM services were limited by hospital governance; IM coordinators approached oncologists and GPs carefully, being conscious of the constraints applied within the hospital system.
Human component of integration
Interviewees believed that building trust with conventional medicine practitioners was critical and required teamwork over time. Even so, they reported a lack of GP referrals and collaboration. The interviewees emphasized that acknowledgment from the medical team of the value of CAM was important. Having a cancer specialist as champion gave some centers the imprimatur of mainstream medical approval and safety. Two interviewees stated that having a coordinator from a nursing background helped increase doctor referrals. At all centers, the coordinator interfaced among stakeholders, CAM practitioners, and patients, working as a navigator. Generally, the interaction between teams or practitioners was informal, without organized meetings or limited to certain members. Preferences were for a unified, nonhierarchical, and collaborative approach.
All centers emphasized the importance of patient engagement in IM. The patient was seen as an expert and an equal contributor to his/her own care. Engaging patients and helping them take the lead in managing their own health is a form of empowerment. The relationship between CAM practitioners, patients, and the coordinator was important in delivering patient-centered care. Patient-centered care occurred through iterative informal processes and was dependent on an individual practitioner's approach to providing care.
Systematic components of integration
Five aspects of systems within IM were investigated as follows: patient screening, accreditation of practitioners, sharing patient information, standardized clinical protocols, and outcome assessment. Systems varied from informal guideline/training, semistandardized programs, to formal reporting of IM treatment to medical staff. Few centers had systematic approaches to the delivery of IM programs due to their limited scope of CAM. Most centers focused on ensuring accreditation of practitioners to guarantee quality and safety. Interviewees agreed that there was a need to regulate IM delivery. Comprehensive application of various CAM/IM programs was desired by all centers. One center was more clinically focused, with a strategic referral system, but most provided programs through an informal pathway based on a comprehensive supportive care assessment and communication with patients.
A few centers had hospital-based AHPs time released to enable them to run CAM/IM programs. If no AHPs were available, patients were referred to community-based practitioners. A high number of referrals from medical staff were considered an indicator of successful integration in some centers.
Resources
All centers stressed funding was one of their biggest challenges. Lack of resources, such as treatment spaces, availability of AHPs/nurses, doctors, and qualified CAM practitioners limited the expansion of services in the hospital and wider community and challenged the sustainability of services. Nine centers indicated that the strength of their centers was the provision of free services (full or partial) to reduce financial burden on patients and open services to the public, including patients' families/caregivers. The majority of centers used volunteer service providers, but retaining volunteers proved challenging.
Despite education and promotion of programs, the majority of patients were not aware of existing CAM services.
Most centers aimed to introduce patients to supportive care or CAM/IM programs in hospital settings, before guiding them to community centers to sustain or improve their health behavior. Table 6 describes selected interviewees' statements that illustrate these points.
Interviewee identifying numbers are unrelated to the center numbers.
Synthesis of the results
Figure 1 describes the conceptual link between the four themes: human components were seen as the key between all the themes. How the care providers perceive CAM influences each of the themes. The impact of individual values from within their cultural context influences resources, while the level of structural integration effects both staff and patient awareness of services.
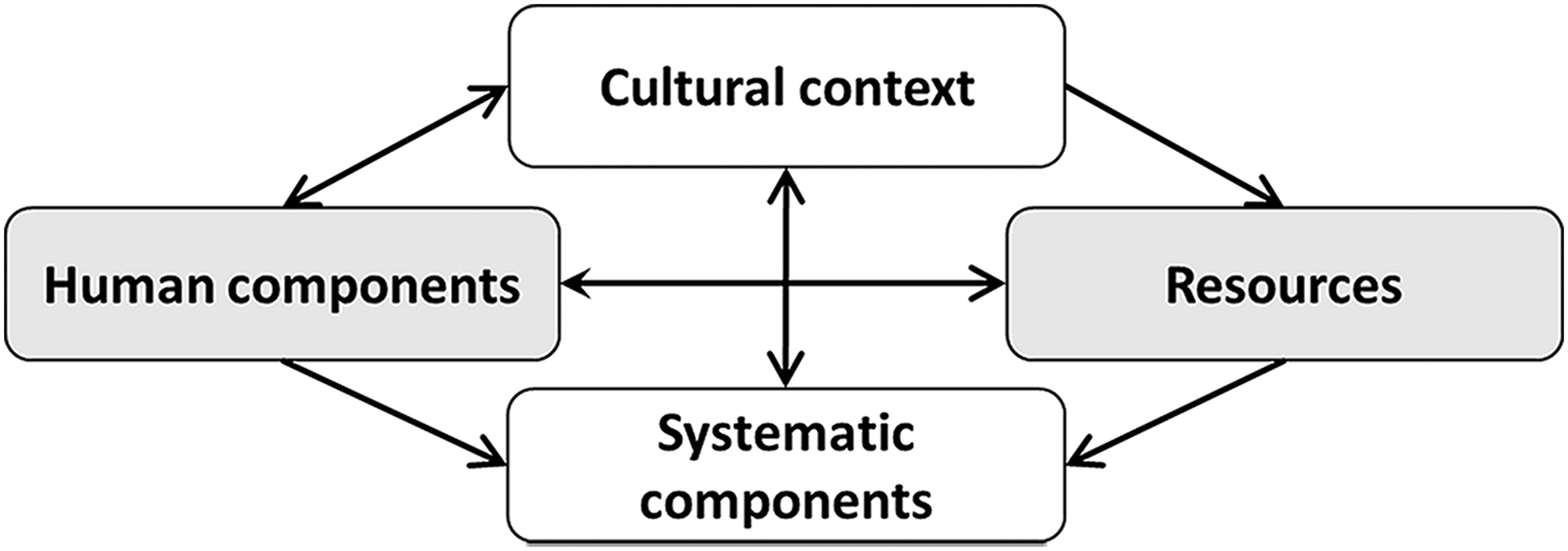
Thematic schema underpinning the perspectives on Australian models of IM. IM, integrative medicine.
Discussion
This mixed method study describes the IM models operating at 10 Australian oncology centers. The existing literature is limited to general populations or small case studies, generally investigating patterns of CAM use, or CAM practitioners' and doctors' perceptions of IM. This study is unique in its investigation of the key elements of IM services for hospital oncology patients that may lead to effective integration of care.
The authors found two important philosophical components in the delivery of IM healthcare in Australia: (1) the concept of wellness and supportive care, including social support, with a holistic focus on patient health, and (2) building relationships between IM providers and patients, as IM is highly individualized and informal in its processes.
Interviewees agreed that patients needed access to supportive care services, emphasizing patient engagement and empowerment in IM care. Similarly, another study evaluating an Australian integrative oncology center identified empowerment, support, and relaxation as key themes, with empowerment driven by the relationship between practitioners and patients. 3,22 The interviewees emphasized the importance of communication between IM providers and patients in enabling patients to openly discuss CAM and become partners in their own healthcare. Other studies reported oncologists need to communicate with patients about CAM use, to enable them to make informed choices. 23
Structural components of IM healthcare are important. The Australian oncology IM models contained characteristics of both the open and parallel models. The process of delivering IM services was adaptable to individual needs, with those accessing services doing so without a referral—a characteristic of the open model. The tendency toward independent CAM/IM practice within hospital settings is characteristic of the parallel model. Interviewees expressed common concerns about current service models and experienced some difficulties engaging and interacting with mainstream medical teams; particularly gaining access to patients, implementing new programs, and dealing with hospital governance and state health systems. There was consensus regarding the need for open collaboration and teamwork with the hospital medical team. A mainstream advocacy (oncologist or nurse as “champion”) helped provide a bridge between systems. A key issue for integration of CAM/IM into the hospital system was trust between teams.
The interviews revealed two distinct cultural views of IM practice; one emphasized the need for scientific evidence for CAM efficacy, while the other focused on safety of practice, patients' beliefs, and feedback from patients concerning outcomes from CAM treatments and healing/caring support. Clinical guidelines for integrative therapies in symptom management of patients with breast cancer published by the Society of Integrative Oncology (SIO) 22 report Grade A evidence for the use of meditation, yoga, and relaxation with imagery, for anxiety and mood disorders. 22 According to these guidelines, the majority of the CAM treatments offered in the 10 centers are based on Grade A evidence. However, demonstrating efficacy based on scientific principles for CAM/IM can be challenging as it uses a different perspective to understand the human body and illness and different philosophical and theoretical approaches to treating patients. 11,13
Lack of written treatment protocols may be perceived as a barrier to quality care by some within the convention healthcare system, but may be due to CAM being highly individualized treatment and requiring flexibility to cater for the complexity of individual needs, while incorporating patient's preferences regarding the choice of treatment modalities.
The strength of the Australian IM models was the no- or low-cost provision of IM services facilitating access, minimizing financial burden, and supporting continued care. On the contrary, these added challenges to funding and resourcing of programs, with many centers reliant on fundraising and volunteers. 24
This study also shows that having medical staffs (cancer specialist, medical doctors, or nurses) as the leaders of IM teams serves to link both medical paradigms and improves the level of trust in CAM practice. It also facilitates the provision of the services. It implies that perception of legitimacy of CAM practice is important in delivering IM services. Conversely, the autonomy of CAM practice may remain as a challenge for the general progress of the field.
Therefore, the results of this study suggest that IM has an impact beyond its clinical approach. The importance of human components and resources within the Australian IM models explored in this study suggest that IM is a complex social nexus between stakeholders. It is clear that successful IM requires incorporation of CAM into conventional medicine within the broader context of healthcare services.
This study has a number of limitations. The authors only evaluated 10 IM oncology centers during a 1-day visit, so findings may not fully represent the IM system at each institution, or be generalizable to other IM centers. This study was not designed to assess the superiority of one model, so the authors can comment only on the models themselves, rather than the impact on patient, professional, and systemic outcomes.
Conclusions
Australian oncology IM models are characterized by separation from conventional medical care, but are responsive to patient demand, within the context of wellness/supportive care services, bridged by a mainstream coordinator. Challenges include acceptance by hospital governance and sustainable funding. The importance of CAM education and the need for a systemic approach to delivering IM services are evident. A collaborative approach involving trust, patient empowerment, and valuing of relationships between stakeholders was considered achievable. To effectively provide integrative healthcare for cancer patients, it is crucial to consolidate cultural beliefs between medical and CAM teams.
Footnotes
Acknowledgments
The authors sincerely thank all the interviewees from the 10 selected Australian IM or wellness centers who participated in this study.
Author Disclosure Statement
No competing financial interests exist.