
Abstract
Objectives:
Various treatment options are available for the management of rosacea symptoms such as facial erythema, telangiectasia, papules and pustules, burning, stinging, and itching. Botanical therapies are commonly used to treat the symptoms. The objective of this review is to evaluate the use of polyphenols in rosacea treatment.
Design:
PubMed, Embase, Biosis, Web of Knowledge, and Scopus databases were systematically searched for clinical studies evaluating polyphenols in the management of rosacea.
Results:
Of 814 citations, 6 met the inclusion criteria. The studies evaluated licochalcone (n = 2), silymarin (n = 2), Crysanthellum indicum extract (n = 1), and quassia extract (n = 1). The studies only evaluated topical formations of stated polyphenols. Main results were summarized.
Conclusions:
There is evidence that polyphenols may be beneficial for the treatment of rosacea symptoms. Polyphenols appear to be most effective at reducing facial erythema and papule and pustule counts. However, studies included have significant methodological limitations and therefore large-scale, randomized, placebo-controlled trials are warranted to further assess the efficacy and safety of polyphenols in the treatment of rosacea.
Introduction
R
Despite the high prevalence and significant impact of rosacea, its pathogenesis is poorly understood. Several key contributing factors include altered innate immune response, dysfunctional epidermal barrier, and vascular hyper-reactivity. Environmental factors such as sun exposure, physical and emotional stress, cosmetics, alcohol, and various foods can also precipitate symptoms. 6 Demodex folliculorum, a species of mite found in the hair follicle, may contribute as well. 7 Overall, the pathologic mechanisms are most likely attributed to a combination of innate immune dysregulation and vascular changes, triggered and perpetuated by reactive oxygen species, UV radiation, and microbes, but aberrant inflammation appears to be a constant.
Rosacea is commonly treated with topical and oral anti-inflammatory therapies. The most commonly prescribed medications are topical metronidazole and oral tetracycline. 8 These treatments are thought to work via their anti-inflammatory properties, and are generally most helpful for patients with the papulopustular (PP) subtype, but may be less effective in the erythematotelangiectatic (ET) subtype. In addition, current treatments are often not totally effective, have side effects and in the case of systemic antibiotics may contribute to antibiotic resistance. 9 Taken together, there is a need for alternative treatments that target the inflammation and erythema associated with rosacea.
Polyphenols are plant-derived compounds that have antioxidant and anti-inflammatory properties, making them of interest to potential rosacea therapies. 10 Polyphenols are the most abundant antioxidants found in the human diet, and are present in fruits and plant-derived beverages such as juice, tea, coffee, and red wine. 11 Plant polyphenols are derived from the common intermediate phenylalanine, or its close precursor shikimic acid. A large variety of plant polyphenols exist, including cinnamic acids, benzoic acids, and flavonoids. 10
Current epidemiological studies strongly support a contribution of polyphenols to the prevention of cardiovascular diseases, cancers, and osteoporosis and suggest a role in the prevention of neurodegenerative diseases and diabetes mellitus. 11 These anti-inflammatory, antioxidant, antiangiogenic, antiparasitic, and photoprotective properties are postulated to be mediated via interactions of various polyphenols with a number of cellular signaling pathways, which are important in maintaining normal cellular function. 12 These properties make products made with polyphenols increasingly popular for skin conditions and in the case of rosacea polyphenols' anti-inflammatory and antiangiogenic properties may represent an untapped therapeutic potential.
This therapeutic potential did not go unnoticed and over the last decade, several clinical studies evaluated the role of polyphenols in treating rosacea. Critical analysis of the results of these studies may highlight the potential of polyphenols as rosacea treatment agents and direct future research. Therefore, we set out to review the current evidence for the efficacy and safety of polyphenol-based therapies for rosacea and inform healthcare professionals of the potential beneficial effects of polyphenols as adjuvants in rosacea management.
Materials and Methods
Search strategy
PubMed, Embase, Agricola, Biosis, Web of Knowledge, and Scopus databases were systematically searched for studies evaluating polyphenol therapies in the treatment of rosacea. The search included all studies published up to September 2, 2016. The search terms included “catechin,” “flavonoids,” “phytochemical,” “polyphenol,” “plant extracts,” “flavanones,” “flavonols,” “flavones,” “isoflavones,” “anthocyanin,” “theaflavin,” “face,” “rosacea,” “pimple,” “acne,” and “erythema.” Searches were filtered to include only those studies published in English language. Detailed search strategy is outlined in Appendix 1.
Eligibility criteria
We included human clinical trials that used a polyphenol intervention. Additionally, we included studies that focused on subjects with rosacea with outcome measures evaluating the change in severity of rosacea symptoms.
We excluded reports that did not describe human clinical trials (such as reviews, abstracts, consensus talks, editorials, retrospective studies, and cross-sectional studies). We also excluded trials that did not study rosacea and did not evaluate a polyphenol.
Selection of studies
Titles and abstracts were reviewed based on inclusion and exclusion criteria. In some cases, full texts were reviewed to assess eligibility. Studies that met the above criteria were included in this review.
Extraction of data
The following information was extracted and summarized from each of the selected studies (Appendix Table A1): polyphenol; study design, duration; comparison; test subjects (N, rosacea subtype, age); relevant outcome measures; relevant results; side effects; and Jadad scale.
Results
Our search yielded 814 articles of which six articles met the inclusion criteria (Fig. 1). Polyphenols studied included silymarin—from Silybum marianum plant (two reports), licochalcone—from licorice plant Glycyrrhiza inflata (three reports), Quassia amara extract from Q. amara plant (one report), and flavonoids from Chrysanthellum indicum extract (one report). All six studies evaluated polyphenols in a topical formulation.
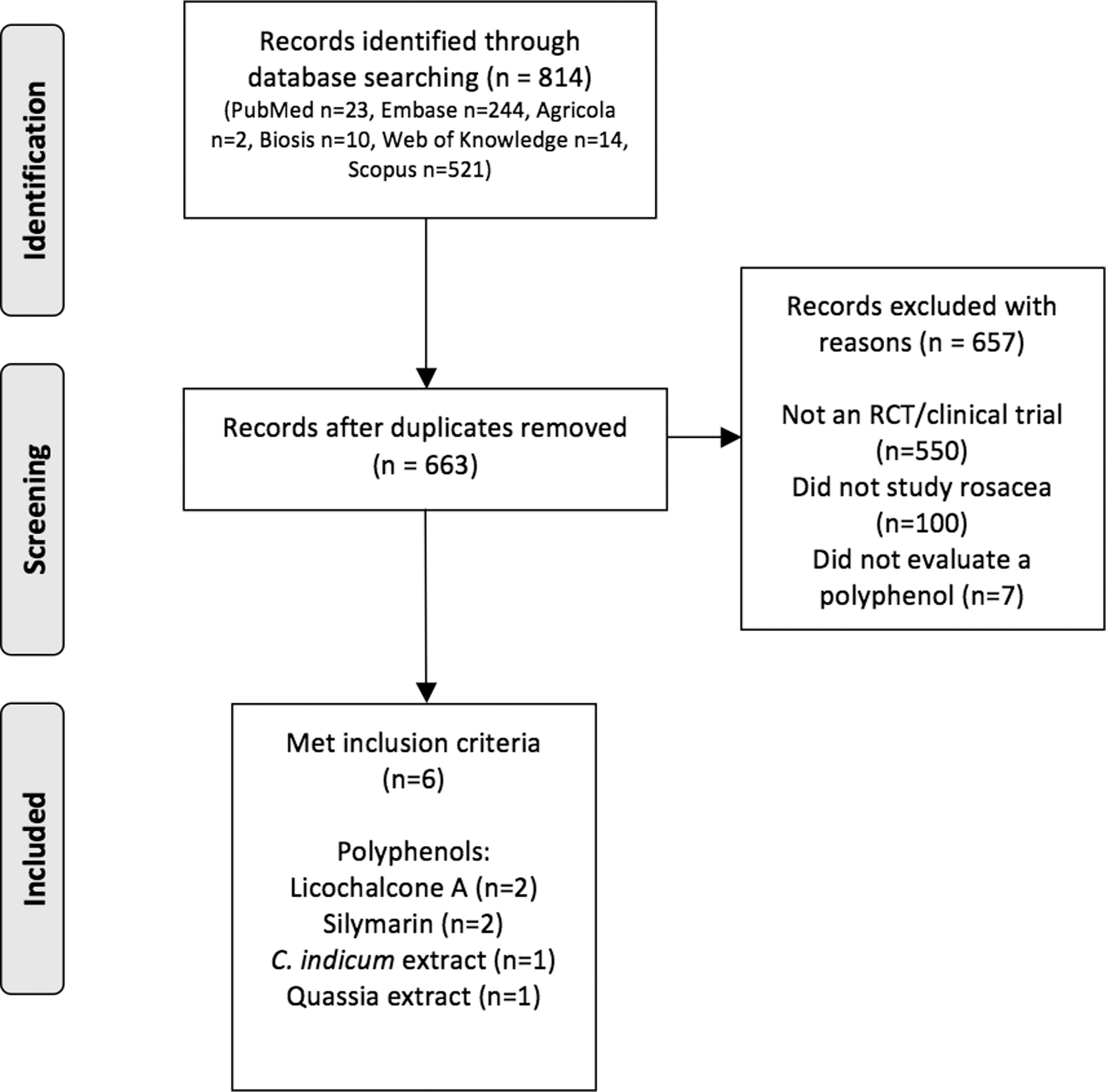
Search strategy and results.
Facial erythema
Weber et al. reported two trials using licochalcone A 13 (Weber I and Weber II hereafter). Weber I was an 8-week, parallel group trial to evaluate “skin compatibility” of licochalcone A containing skin care line on facial redness in patients with mild to moderate erythematotelangiectatic (ET) rosacea (n = 32). These patients were compared to non-rosacea subjects with facial erythema (n = 30). Both groups used licochalcone A-containing skin products (cleanser, moisturizer with green pigments, concealer with pigments, and night cream) at least once daily. The subjects were evaluated at baseline and after weeks 4 and 8. Facial erythema was graded on a 4-point scale (0 = none, 1 = mild, 2 = moderate, 3 = severe). The products that contained green concealing pigments helped neutralize facial erythema. The non-rosacea group had a significant improvement in facial erythema after week 4 (9% improvement, p ≤ 0.05) and week 8 (23% improvement, p ≤ 0.05). The rosacea group had significant facial erythema improvement only after 8 weeks of treatment (7% improvement, p ≤ 0.05). The authors postulated that the difference in improvement between the two groups could be due to a difference in erythema severity at baseline, the variation in efficacy time course, and a different etiology to rosacea-based erythema compared to non-rosacea-based erythema. The results in this study, although statistically significant, demonstrated minimal absolute differences and therefore the clinical utility is unclear. The product line used in this study included moisturizers, sunscreens, and red tint—all play an objective role in the treatment of rosacea. Therefore, in the absence of a placebo arm, the effects of the polyphenol, if any, could be masked. In addition only women were included in this study and therefore conclusion about men cannot be made. Finally, there were no reports of adverse events suggesting safety.
Weber II was a 4-week clinical trial comparing the use of the licochalcone A containing skin care line as an adjuvant to metronidazole 0.75% with patients' own skin care product. Patients included in the trial had ET rosacea (n = 25) and PP rosacea (n = 8). All patients used metronidazole during the 4-week trial. However, subjects used their usual skin care products during weeks 1 and 2, and they were given licochalcone A-containing products to use in weeks 3 and 4. Facial erythema was evaluated at baseline, weeks 2 and 4 on a 4-point scale. In the ET rosacea group there was a significant decrease in erythema score at week 2 (p ≤ 0.05) and week 4 (p ≤ 0.05) compared to baseline. It is difficult to assess the specific effects of the polyphenol used in this study since the comparison is unclear. No adverse events were reported.
Broniarczyk-Dyła et al. 14 conducted an 8-week single-group trial to evaluate two licochalcone-containing face creams. All subjects (n = 35) had ET rosacea and one subject also had PP features. The day cream contained SPF 15, while the night cream had panthenol; both creams contained licochalcone. Facial erythema was evaluated via skin colorimetry. The mean erythema severity was significantly decreased after 8 weeks of treatment with licochalcone creams (p = 0.002). Sixteen patients experienced improvement in erythema severity after 6 weeks of treatment. The notable weakness of this study was the lack of a control group, which could mean that the effect seen is simply due to use of a sunscreen. In addition, the study only included two men. Of note, the products were well tolerated suggesting a good safety profile.
In a randomized, double-blind, placebo-controlled trial by Berardesca et al. 15 46 subjects with ET and/or inflammatory rosacea used silymarin-methylsulfonylmethane (S-MSM) cream or placebo vehicle twice daily for 30 days. Erythema severity was assessed at baseline and days 10, 20, and 30 and was graded using a 5-point clinical score (0 = no symptoms, 4 = very severe). Skin colorimetry measured the erythema index. The S-MSM group experienced a significant reduction in clinical erythema score at day 30 compared with baseline (p < 0.001) and placebo group (p < 0.001). Additionally, the S-MSM group experienced a significant decrease in erythema index after 30 days of treatment compared with baseline (p < 0.001) and placebo (p < 0.01).
Nield and Ippersiel 16 conducted a single-group, open label, 12-week trial to evaluate a silymarin-containing cream in the management of facial erythema. The subjects (n = 32) had rosacea with erythema score of 3 in at least one area on the face. They applied the cream twice daily for 12 weeks. Erythema was evaluated at baseline, weeks 6 and 12 on a 6-point scale (0 = no redness, 5 = persistent severe redness). Compared to baseline, the mean erythema score reduced by 40% at 6 weeks (p < 0.001) and 58% by week 12 (p < 0.001). The mean erythema score was lower after 12 weeks of treatment compared to 6 weeks (p < 0.001). Telangiectasia was scored from 0 = none to 5 = severe but it did not decrease significantly over the study period. Notably, 16 patients were using various prescription strength creams to treat their rosacea while participating in the trial. The investigators also provided subjects with a sunscreen with a physical blocker. Therefore, drawing conclusions about the effect of silymarin on redness in this trial is difficult. Notably, one patient experienced stinging, burning, and increased redness leading to discontinuation.
Rigopoulos et al. 17 conducted a multicenter randomized, double-blind, parallel group, placebo-controlled trial comparing a 1% flavonoid-rich cream (n = 125) to a placebo (n = 121) over 12 weeks, applied twice daily. The extract was derived from a plant called C. indicum. At enrollment, all subjects had rosacea corresponding to grade 2–4. After 12 weeks, 73% of subjects in C. indicum group had an improvement in at least one erythema score, compared to 68% of subjects in placebo group. Additionally, there was a 41% reduction in the mean erythema score in C. indicum group compared to 33% reduction in placebo group compared to baseline. Clearing or marked improvement (rosacea 0–2 on a 7-point scale) was seen in 81% of subjects treated with C. indicum and 61% in placebo group. Erythema surface (calculated using investigator's sketch and running a computerized area calculation) was improved in 91% of subjects in C. indicum group and 87% in placebo group, without significant difference between the two groups. Overall, the C. indicum cream was statistically more effective at reducing facial redness than placebo. However, considering the absolute values of the effects in all parameters questions the clinical utility of this difference. This also suggest a strong effect of the vehicle and confirms that at baseline the subjects were not treated at all (patients had 6-week run in phase without any treatment). A notable number of patients in the intervention (10.4%) and the placebo groups (6.6%) experienced adverse effects. The investigators noted in post hoc analysis that the intervention group included higher number of patients with self reported sensitive skin. This finding speaks to the active effect of the placebo and objective difficulty of treating patients with rosacea.
In a 6-week open label, single-group trial, Ferrari and Diehl 18 evaluated a 4% quassia extract topical gel in the treatment of rosacea. Subjects (n = 30) had rosacea type I–IV and applied the topical in the morning and evening for 45 days. Subjects were evaluated at baseline, days 15, 30, and 45. There was a continuous decrease in the mean erythema score from baseline to day 45, with a significant overall decrease of 56% (p < 0.001) at the end of the treatment period. The telangiectasia score decreased by 50% by the end of treatment period (p < 0.001). No adverse effects were noted.
Papule and pustule count
The second Weber study included subjects with PP rosacea (n = 8) who were instructed to use metronidazole 0.75% and their usual skin care products for 2 weeks and metronidazole and licochalcone-containing products during weeks 3 and 4. 13 Compared to baseline, the papule count decreased significantly after 2 weeks of metronidazole use (3.87 point decrease, p ≤ 0.05). Additionally, after using the licochalcone and metronidazole combination during weeks 3 and 4, the papule count was significantly lower compared to baseline (p ≤ 0.05). There was no significant decrease in pustule count after using metronidazole alone for 2 weeks. However, results after week 4 indicated a significant decrease in pustule count (p ≤ 0.05).
In a randomized, double-blind, placebo-controlled trial by Berardesca et al., 30 days of S-MSM cream resulted in a significant reduction of papules compared to baseline (p < 0.001). 15 Additionally, compared to the control group, after 30 days of treatment the S-MSM group had a significantly lower pustule count (p < 0.001). Quassia extract gel resulted in a decrease in papule score by 84% (p < 0.001) while pustules decreased by 100% from baseline to day 45.
Skin hydration
Broniarczyk-Dyła et al. 14 showed that the use of twice daily licochalcone cream significantly increased skin hydration after 6 and 8 weeks compared to baseline (p = 0.008). Additionally, the transepidermal water loss (TEWL) decreased significantly after 6 weeks of licochalcone treatment (p = 0.014).
In a different study evaluating S-MSM cream versus vehicle control, skin hydration increased in both groups over the 30-day period (p < 0.01) and no differences between S-MSM and control group were detected at day 30. 15
Quality of life
In the first Weber study, two groups of subjects (those with rosacea and those with red skin not due to rosacea) completed a seven-item quality of life (QoL) questionnaire at baseline and after 8 weeks of treatment with four daily skin care products containing licohalcone A. 13 The weighted average of all QoL responses was determined and called the Quality of Life Index (QOLI). The QOLI significantly improved (p < 0.05) after 8 weeks of treatment with licochalcone A (QOLI 1.37) compared to baseline (QOLI 1.56). However, since the investigators reported the results as a combination of both rosacea and non-rosacea patients, specific conclusions relating to rosacea cannot be made.
Adverse effects and skin tolerance
In the Weber I study 89% of subjects reported that licochalcone A products were gentle on their skin, while 5% disagreed. 13 Additionally, 87% of subjects reported that the products were well tolerated, while 5% disagreed. In the study by Broniarczyk-Dyła et al., the day cream containing licochalcone was well tolerated by 70% of subjects and night cream by 82% of subjects. 14 None of the subjects reported irritation or hypersensitivity, and a small number experienced lacrimation, which resolved after a few minutes of application. Nield and Ippersiel, found that one of 29 subjects who completed the study experienced burning, stinging, and increased erythema and thus discontinued use of the topical after 2 weeks. 16 On the other hand, 27 of 29 patients (93%) were highly satisfied with the cream and reported that they would continue using it.
In the study that evaluated C. indicum cream, 61% of patients in the treatment group reported positive judgment about cream efficacy after 12 weeks of treatment, compared to 39% in placebo group (p = 0.01). Adverse events occurred in 13 of 125 subjects in C. indicum group and 11 of 121 in placebo group and were rated mild or moderate. Specific side effects were not reported. The authors concluded that the C. indicum cream was fairly safe and well tolerated. The 4% quassia extract study showed no side effects (i.e., itching, burning, stinging, edema) and tolerance was reported to be excellent. 18 Thirty-seven percent of subjects had excellent improvement or complete remission of rosacea, 22% marked improvement, 30% moderate improvement, and 11% no improvement over the 45-day study period.
Subjective skin irritation scores
The Weber I 13 study reported no increase in subjective irritation score after 8 weeks of treatment with the four topical products containing licochalcone A compared to baseline. In the Weber II 13 study, subjects used metronidazole 0.75% and had a significant decrease in burning, stinging, and tingling with each value reaching zero after 2 weeks of treatment (p ≤ 0.05). The values remained at zero after addition of licochalcone A. Itching and tightness both improved significantly after 2 weeks on metronidazole compared to baseline (p ≤ 0.05) and showed continued improvement after addition of licochalcone A during weeks 3 and 4.
Berardesca et al. 15 showed that 30 days of S-MSM treatment lead to a significant reduction in severity of itch (p < 0.001) and stinging (p < 0.001) compared to baseline. Additionally, at day 30, the S-MSM group had significantly lower itch (p < 0.01) and stinging severity (p < 0.01) compared to control group. S-MSM had no effect on burning sensation.
Discussion
Based on the studies reviewed here, licochalcone A, silymarin, C. indicum, and quassia extracts may be beneficial for improving facial erythema of rosacea. Additionally, licochalcone creams may play a role in improving skin appearance, and QoL in people with rosacea. 13
Silymarin and quassia extract may have a role as adjunct treatments in decreasing the papule counts in PP rosacea. 15,18 Interestingly, quassia extract was successful in reducing 100% of pustules in the study. 18 Conversely, C. indicum reduced the papule count, but had no effect on pustule count. 17 Quassia extract is the only polyphenol that decreased the telangiectasia score. 18
Polyphenol mechanism of action
These clinical data are consistent with earlier results demonstrating a role for polyphenols in improving rosacea symptoms through their anti-inflammatory, antioxidant, antiangiogenic, and photoprotective properties (Table 1).
Anti-inflammatory properties
Flavonoids, a subgroup of polyphenols, are known to have anti-inflammatory properties. Licochalcone, derived from licorice root and traditionally used in the treatment of inflammatory conditions, 19 contains flavonoids and isoflavonoids giving it its anti-inflammatory, anti-irritant, and antierythema properties. In vitro studies on licochalcone A show that it is a potent inhibitor of cells' proinflammatory responses. 20 Licochalcone A also inhibits T cell proliferation and cytokine production. 21 After keratinocytes are exposed to UVB radiation, Licochalcone A is able to inhibit the release of prostaglandin E2. 22 The mechanism of action of Licochalcone A is still not fully understood at a molecular level, but when applied to irritated and sensitive skin licochalcone A has shown to have therapeutic effects. 20 Additionally, it has antimicrobial 23 and antiparasitic 24 properties and improves the skin barrier function by improving skin hydration and decreasing the TEWL. 14
Quassia extract, derived from Q. amara plant that originates in South America, also has anti-inflammatory effects on the skin. It inhibits tumor necrosis factor-α, interleukin-1β, and nitric oxide. 18 Like Licochalcone A, Quassia extract also has antiparasitic effects. 18 Silymarin also acts as an anti-inflammatory by inhibiting the release of inflammatory mediators prostaglandin E2 and interleukin-1β. 25
Antioxidant properties
Antioxidants are compounds that protect cells from the damaging effects of free radicals or reactive oxygen species (ROS). Silymarin possesses strong antioxidant properties that allow it to eliminate ROS and thus prevent lipid peroxidation and cell damage. 25 Silymarin is also able to inhibit certain enzymes and in this way prevent the formation of free radicals. 26 Additionally, it is able to activate other antioxidants and antioxidant enzymes via transcription factors. 26 Other sources of polyphenols that have antioxidant properties include a flavonoid-rich plant that grows in West Africa called C. indicum, and Quassia extract derived from Q. amara plant that originates in South America. 17,18
Impact on vascular wall permeability
In ET rosacea, capillary walls become more permeable due to inflammatory stress; there is also an associated loss of endothelium and damage to vasculature. 15 Flavonoids have the ability to inhibit proteolytic enzymes, elastase and hyaluronidase, and thus decrease permeability of the vascular endothelium. 27
Antiangiogenic properties
Silymarin inhibits the vascular endothelial growth factor preventing angiogenesis and the matrix metalloproteinase-2 release modulating the destruction of vascular matrix. 28,29
Polyphenol adverse reactions
Most studies reviewed in this article reported mild to moderate adverse reactions, including lacrimation, burning, stinging, and erythema. However, no serious adverse effects were reported and the topical formulations were generally well tolerated. There were no side effects reported in association with the 4% quassia extract topical and it was reported to have excellent tolerance. Future studies examining various concentrations of polyphenols are warranted.
Limitations
The results of this review shed light on the potential for a clinical benefit for polyphenols in the treatment of rosacea symptoms. However, significant caution should be exercised in the interpretation of the results included in this review since the majority of the studies represent initial open label investigations. In addition, methodological flaws make it hard to distinguish the specific role a polyphenol played in achieving the claimed results. Additionally, most studies reviewed here had small sample and included significantly more women limiting the ability to generalize their results. More studies of high quality are needed to establish efficacy of various types of polyphenols in the management of rosacea.
Conclusion
Many plants contain polyphenols including S. marianum, G. inflata, Q. amara, and C. indicum as reviewed here. There is evidence that polyphenols may be beneficial for skin health and for the treatment of rosacea and initial data suggest topical application is well tolerated. Overall, polyphenols may have a role in reducing facial erythema and papule and pustule counts in rosacea. Polyphenols may be used to complement existing regimens and may even offer an alternative to current treatment options especially in patients sensitive to other medications. Our search produced a limited number of studies on polyphenols and how they may be used in rosacea treatment. All studies evaluated only topical formulation of polyphenols. Large-scale clinical studies are warranted to further assess the efficacy and safety of polyphenols in the treatment of rosacea. Regardless of the findings presented here, the best approach to rosacea management begins with identification of individual triggers, use of sun protection, and patient education.
Footnotes
Acknowledgment
We thank Bruce Abbott for his assistance with the systematic search.
Author Disclosure Statement
R.K.S. serves as a scientific advisor to Dermveda. The other authors have no conflicts of interest.