
Abstract
Objectives:
This study was aimed to compare the effectiveness of aromatherapy and acupressure massage intervention strategies on the sleep quality and quality of life (QOL) in career women.
Design:
The randomized controlled trial experimental design was used in the present study. One hundred and thirty-two career women (24–55 years) voluntarily participated in this study and they were randomly assigned to (1) placebo (distilled water), (2) lavender essential oil (Lavandula angustifolia), (3) blended essential oil (1:1:1 ratio of L. angustifolia, Salvia sclarea, and Origanum majorana), and (4) acupressure massage groups for a 4-week treatment. The Pittsburgh Sleep Quality Index and Short Form 36 Health Survey were used to evaluate the intervention effects at pre- and postintervention.
Results:
After a 4-week treatment, all experimental groups (blended essential oil, lavender essential oil, and acupressure massage) showed significant improvements in sleep quality and QOL (p < 0.05). Significantly greater improvement in QOL was observed in the participants with blended essential oil treatment compared with those with lavender essential oil (p < 0.05), and a significantly greater improvement in sleep quality was observed in the acupressure massage and blended essential oil groups compared with the lavender essential oil group (p < 0.05).
Conclusions:
The blended essential oil exhibited greater dual benefits on improving both QOL and sleep quality compared with the interventions of lavender essential oil and acupressure massage in career women. These results suggest that aromatherapy and acupressure massage improve the sleep and QOL and may serve as the optimal means for career women to improve their sleep and QOL.
Introduction
M
Sleep is vital for individual health and well-being; it is also a key predictor of overall QOL. 6 Current clinical medical treatment is the main therapy for poor sleep quality. Although such therapy generates immediate effects, long-term use tends to cause daytime sleepiness, which increases the risk of accidents or falling. 7 Complementary and alternative medicines, such as acupuncture, massage, qigong, and aromatherapy, were recently used to improve the negative effects of poor sleep quality and mitigate sleepiness, anxiety, and fatigue. 8 Furthermore, Gupta et al. reported that acupressure, massage, and aromatherapy were several frequently used complementary therapies for improving their skeletomuscular disorders and job satisfaction. 9 These raise the possibility that using these complementary and alternative modalities might be effective in improving the qualities of sleep and life without adverse effects. However, there is still lack of evidence focusing on the effectiveness of these frequently used complementary therapies.
Aromatherapy involves using essential oils extracted from various parts of plants. Essential oils are applied to the human body through massage, bathing, oral ingestion, or inhalation, and absorption of essential oils through the respiratory tract, gastrointestinal tract, or skin activates the body's self-healing ability, producing an integrated effect in the body, mind, and spirit. 10 Empirical results have shown that aromatherapy is effective for calming, relaxation, and pain relief, thus improving both mental and physical conditions. 11 Moreover, administration of lavender and rosemary extract oil enhanced the QOL by alleviating pain unpleasantness in health young adults. 12 Recently, linalyl acetate, the main component of several essential oils (i.e., lavender, muskatellersalbei, and marjoram essential oils), has been reported to have positive effects on improving sleep quality. 12,13 In addition, sclareol, a chemical component enabling female endocrine system balance, is found in muskatellersalbei essential oil. 14,15 These led us to investigate the distressing effects of blended essential oil consisting of lavender, muskatellersalbei, and marjoram on QOL in career women.
Acupressure massage is derived from acupuncture and involves stimulating the pressure points to facilitate smoothing the meridians and the whole system to promote overall health. In recent years, acupressure massage has been applied to clinical care to improve physical and mental problems such as depression and fatigue and poor sleep quality. 16,17 Studies have verified that acupressure massage effectively enhances sleep quality in long-term care residents, 18,19 teenagers, 20 patients with end-stage renal disease, 21 and critically ill patients in intensive care units. 17 Moreover, existing evidence obtained from randomized controlled trials (RCTs) also reveals that acupressure massage and acupuncture are effective to attenuate menstrual stress symptoms in young adult women with dysmenorrhea 22 and improve sleep quality/QOL in menopausal women. 23,24
However, to our knowledge, no available scientific evidence exists in regard to the health benefits of these alternative modalities on ameliorating sleep quality and QOL in the career women population. Therefore, this study compared the effectiveness of aromatherapy and acupressure massage intervention strategies on the sleep quality and QOL in career women.
Methods
Materials of aromatherapy
In the present study, we selected lavendel fein (Lavandula angustifolia) as the intervention medium for the lavender essential oil inhalation treatment. For the blended essential oil inhalation treatment, we mixed essential oil consisting of lavendel fein essential oil (L. angustifolia), muskatellersalbei essential oil (Salvia sclarea), and marjoram essential oil (Origanum majorana). All the essential oils used in this study were commercially available (Primavera Life GmbH, Oy-Mittelberg, Germany), and we also performed aromatherapy procedure in accordance with the instructions provided by the manufacturer.
Ethical considerations
This study was approved by the Institutional Review Board of the Behavioral and Social Sciences department of National Taiwan University (oil aromatherapy intervention: 201409ES010; acupressure massage: 201408ES019), and all the procedures were conducted in accordance with the IRB guidelines. The purpose and procedures had been clearly explained to participants before recruitment, and the written informed consent form was then signed by all participants.
Study design and participants
The RCT experimental design was used in the present study. Research participants were career women living in Taipei metropolitan area, Taiwan, who did not work on rotating night shifts. The potential participants attended volunteer recruitment fairs after responding to a participant recruitment advertisement. The overall recruitment period lasted for 3 months (February–May, 2015). Thereafter, we began the prescreening and intervention process when a sufficient number of potential participants were recruited, and the period of data collection was conducted between May and August, 2015. After prescreening, the aim and detailed experimental procedure were explained to the qualified participants, and informed written consent was obtained from all participants before the study began. The inclusion criteria were being aged 24–55 years, not having reached menopause, attaining a score of ≥5 on the Pittsburgh Sleep Quality Index, and not having received regular aromatic-related therapy or acupressure massage in the past 3 months. The exclusion criteria were having asthma or any diseases involving notable organ damage (e.g., heart, lungs, liver, or kidney failure or severe olfactory dysfunction), being pregnant, being allergic to essential oils, being unable to stop taking sleep medications during the research period, and inability to participate in the full course of the intervention courses. One hundred thirty-two qualified women participated, and they were randomly assigned to a placebo group, lavender essential oil group, blended essential oil group, or acupressure massage group. Each group contained 33 participants and was engaged in a 4-week intervention. However, two participants in the lavender essential oil group became pregnant in the early stage of intervention, three participants in the acupressure massage group withdrew from the research halfway because of work factors, and one participant in the placebo group discontinued for personal reasons. Thus, six participants were lost and the final research sample comprised 126 participants (31 in the lavender essential oil group, 33 in the blended essential oil group, 30 in the acupressure massage group, and 32 in the placebo group). See Figure 1 for the flowchart of experimental procedure and design.
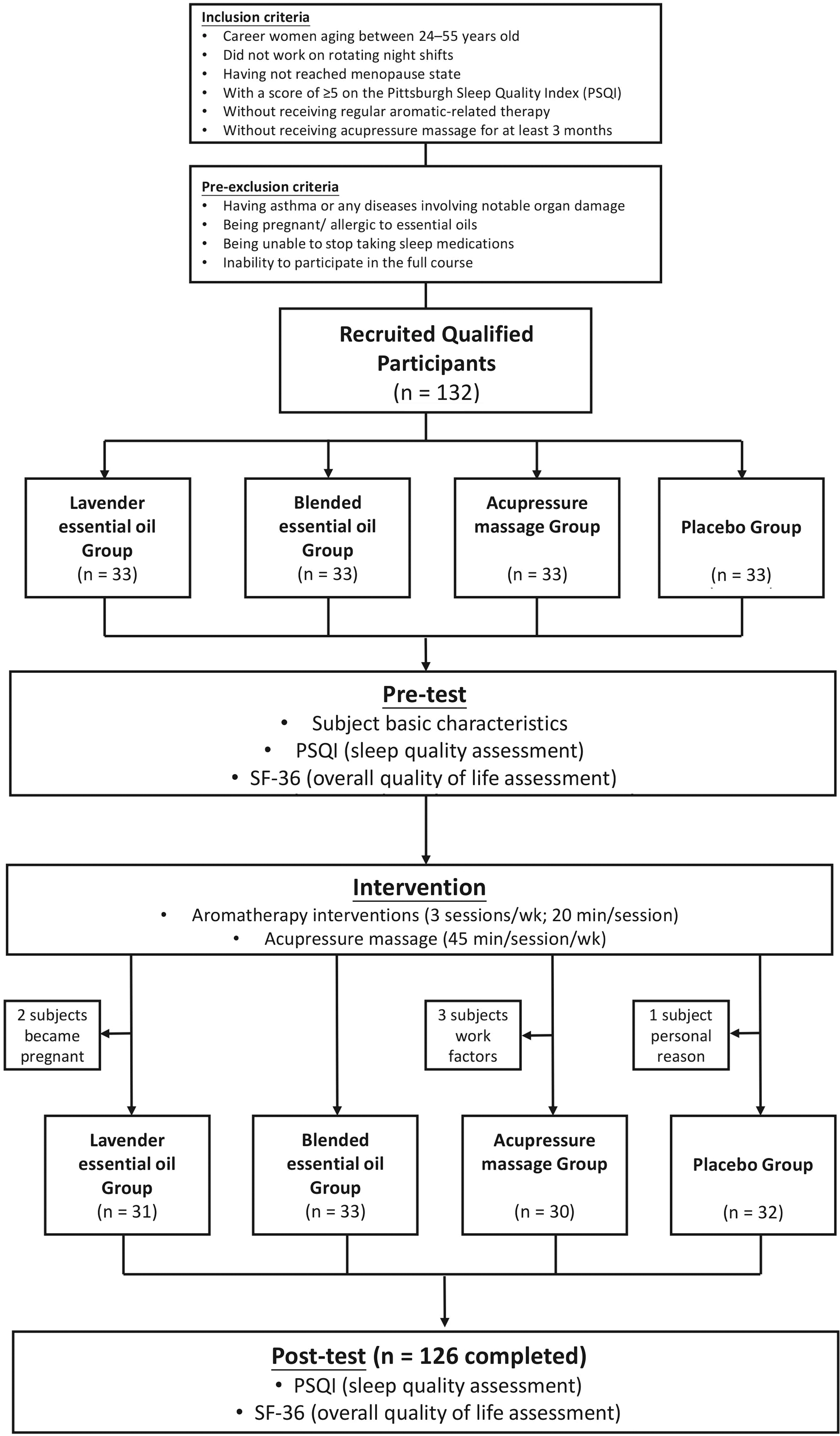
The flowchart of experimental procedure and design. PSQI, Pittsburgh Sleep Quality Index; SF-36, Short Form 36 Health Survey.
Aromatherapy interventions
After referring to related studies on insomnia treatment and anxiety reduction, 14,25,26 the present study selected lavendel fein (L. angustifolia; 0.25 mL) as the intervention medium for the lavender essential oil group; a 1:1:1 ratio of lavendel fein (L. angustifolia; 0.25 mL), muskatellersalbei (S. sclarea; 0.25 mL), and marjoram (O. majorana; 0.25 mL) (Primavera Life GmbH, Oy-Mittelberg, Germany) for the blended essential oil group; and distilled water for the placebo group. The present study adopted five drops (1 drop = 0.05 mL) as the intervention dosage according to the previous study. 27 Before the intervention, an essential oil allergy test was administered to the essential oil and blended essential oil groups to ensure the absence of allergic reaction. The participants placed an ultrasonic aromatherapy diffuser (Anion Detector/Inti ITC-201A, Andzen Enterprise Co., Ltd., Taiwan) in their own bedrooms at a distance of ∼30 cm from their heads. Subsequently, 160 mL of distilled water and five drops of intervention essential oil were infused in the chamber of the diffuser. The participants relaxed and rested quietly, either sitting by the bedside or lying on the bed, while the vapor diffused into the air. Each therapy session lasted for 20 min and was conducted three times a week for four consecutive weeks. The researcher monitored the intervention by placing regular phone calls each week.
Acupressure massage interventions
The acupressure massage intervention for the acupressure massage group was designed following related literature. 28,29 A masseur used both hands to exert pressure massage at a strength level of 3–5 kg, focusing on the meridians that facilitated improving sleep quality. Specifically, the acupressure massage intervention was focused on 17 acupuncture points (as shown in Appendix Table 1) located along various meridians, including the large intestine, triple energizer, small intestine, lung, pericardium, heart, and governor meridians, as well as meridians that effectively enhance head circulation and sleep quality. The operating procedure of acupressure massage was formulated according to the standards of World Health Organization, 30 and each acupressure massage session lasted for 45 min and was conducted once per week for four consecutive weeks. There was one experienced masseur with 5 years of practical experience performing all the acupressure massage procedures in this study. To ensure stability, consistency, and accuracy of the massage procedures exerted by the masseurs, their techniques were evaluated by the registered Chinese medicine physicians. A significant correlation was observed between the pressure exerted by both hands (r = 0.81; p < 0.05), and the results showed a content validity index of 0.95 (p < 0.05) by using the scores of accuracy ranging from 4 (very accurate) to 1 (very inaccurate).
Pittsburgh Sleep Quality Index
The Chinese version of Pittsburgh Sleep Quality Index (PSQI) translated by Tsai et al. was adopted in this study. 31 The questionnaire comprised nine questions divided into seven constructs: sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbance, use of sleep meds, and daytime dysfunction. The participants completed the questionnaire according to their sleep conditions over the previous month. The higher the scores they obtained, the poorer the sleep quality they experienced. The overall Cronbach's α of PSQI is 0.83. 32 The PSQI and a polysomnography test were applied to examine the validity of the Chinese version of PSQI, and the accuracy, sensitivity, and specificity of the questionnaire were 88.5%, 89.6%, and 86.5%, respectively (Kappa = 0.75; p < 0.001), indicating that the Chinese version of PSQI demonstrated satisfactory reliability and validity. 31,32
Taiwanese version of the Short Form 36 Health Survey
This study adopted the Taiwanese version of the Short Form 36 Health Survey (SF-36) scale translated by Lu et al. 33 The scale was translated according to the principles of the International QOL Assessment research project, 34 comprising eight constructs and 36 items that comprise 10 items on physical functioning, four items on role limitations of physical problems, two items on bodily pain, five items on general health, four items on vitality, two items on social functioning, three items on emotional role, and five items on mental health. The participants completed the items according to their physical and mental conditions in the previous month. Apart from social functioning (Cronbach's α = 0.65), Cronbach's α coefficients for all constructs in this questionnaire ranged between 0.70 and 0.93, exhibiting favorable reliability and validity.
Data analysis
Statistical analysis of the research data was conducted using SAS, version 9.2 (SAS Institute, Inc., NC). A chi-square test was performed to compare the between-group differences among the experimental (lavender essential oil, blended essential oil, and acupressure massage) and placebo groups. A generalized estimating equation (GEE) was employed to conduct comparisons between the pre- and post-test results of the experimental and placebo groups. The outcome measurements included PSQI summary, physical component summary (PCS), mental component summary (MCS), and summary of QOL (SF-36), and the within-group confounding variable was time (pre- and post-test). The significant levels for all the performed statistical tests were set as α = 0.05.
Results
Table 1 illustrates that the between-group differences in age, marriage status, educational attainment, work seniority, income, and the number of children were nonsignificant (p > 0.05). After 4 weeks of intervention, the pre- and post-test means and standard deviations among the lavender essential oil, blended essential oil, and acupressure massage groups in sleep quality, PCS, MCS, and QOL were calculated (Table 2).
NT$, New Taiwan dollar.
MCS, mental component summary; PCS, physical component summary; PSQI, Pittsburgh Sleep Quality Index; SD, standard deviation; SF-36, Short Form 36 Health Survey.
Table 3 displays the overall effects of sleep quality measured by the PSQI, and a statistical model of GEE was employed to analyze variations in PSQI scores of the four groups after the intervention. GEE model is a statistical estimation method based on generalized linear models (GedLM) for analysis, and this method is another well-recognized analytical method for the mixed design interventional study (comparing groups with pre- and post-test). In this study, an examination of the interaction effect between the group and time (pretest vs. post-test) factors revealed that the lavender essential oil group attained 1.68 points less in the pretest–post-test difference in the PSQI overall score compared with the placebo group (LAV vs. CON × pretest vs. post-test) (p < 0.01). The blended essential oil group attained 4.32 points less in the pretest–post-test difference in the PSQI overall score compared with the placebo group (p < 0.001). The acupressure massage group attained 4.01 points less in the pretest–post-test difference in the PSQI overall score compared with the placebo group (p < 0.001). These results verified that compared with the distilled water placebo group, the lavender essential oil, blended essential oil, and acupressure massage interventions significantly improved the overall sleep quality. The acupressure massage group attained 2.33 points less in the pretest–post-test difference in the PSQI overall score compared with the lavender essential oil group (p < 0.01). By contrast, the acupressure massage group obtained 0.30 points more in the pretest–post-test difference in the PSQI overall score compared with the blended essential oil group (p > 0.05). Finally, the blended essential oil group attained 2.63 points less in the pretest–post-test difference in the PSQI overall score compared with the lavender essential oil group (p < 0.001).
p < 0.01; *** p < 0.001.
ACU, acupressure massage; BLE, blended essential oil; LAV, lavender essential oil; PLA, placebo group; time, pretest versus post-test; SEM, standard error of mean.
Table 4 presents the effects of the interventions on QOL (i.e., PCS, MCS, and overall SF-36 summary), and a statistical model of GEE was employed to analyze variations in the SF-36 scores of the four groups after the intervention. An examination of the interaction effect between the group and time factors revealed that compared with the placebo group, the lavender essential oil group attained 34.08 more points in the pretest–post-test difference at the physical level (PCS, p < 0.05), 48.01 more at the mental level (MCS, p < 0.05), and 82.09 more in the overall QOL (SF-36 summary, p < 0.05). Compared with the placebo group, the blended essential oil group attained 93.04 more points in the pretest–post-test difference at the physical level (PCS, p < 0.001), 118.69 more at the mental level (MCS, p < 0.001), and 211.73 more in the overall QOL (SF-36 summary, p < 0.001).
p < 0.05; ** p < 0.01; *** p < 0.001.
Compared with the placebo group, the acupressure massage group attained 45.34 more points in the pretest–post-test difference at the physical level (PCS, p < 0.05), 78.74 more at the mental level (MCS, p < 0.01), and 124.08 more in the overall life quality (SF-36 summary, p < 0.01). These findings suggest the positive effect of acupressure on improving QOL above placebo treatment. However, compared with the lavender essential oil group, the acupressure massage group attained 11.25 fewer points in the pretest–post-test difference at the physical level (PCS, p > 0.05), 30.72 more at the mental level (MCS, p > 0.05), and 41.98 more in the overall QOL (SF-36 summary, p > 0.05). Compared with the blended essential oil group, the acupressure massage group attained 47.70 fewer points in the pretest–post-test difference at the physical level (PCS, p > 0.05), 39.95 less at the mental level (MCS, p > 0.05), and 87.65 less in the overall QOL (SF-36 summary, p > 0.05). Compared with the lavender essential oil group, the blended essential oil group attained 58.95 more points in the pretest–post-test difference at the physical level (PCS, p < 0.05), 70.67 more at the mental level (MCS, p < 0.05), and 129.63 more in the overall QOL (SF-36 summary, p < 0.01).
Discussion
To our knowledge, this is the first study comparing the effectiveness of the most popular complementary and alternative modalities, aromatherapy and acupressure massage, on sleep quality and QOL in career women. The primary findings of this investigation are that aromatherapy interventions involved applying lavender or blended essential oil (consisting of L. angustifolia, S. sclarea, and O. majorana; three times/weeks; 20 min each session) and acupressure massage (45 min/session/weeks) had positive effects on improving sleep quality and QOL in career women. Moreover, our results also further verified that blended essential oil aromatherapy had greater benefits on promoting both sleep quality and QOL, but acupressure massage only showed the effect on improving sleep quality in this population.
Our current results revealed that lavender and blended essential oil inhalation both significantly improved the QOL in career women. In agreement with previous studies, 12,27,35 the lavender and blended essential oil interventions were both effective in improving their QOL compared with the lavender essential oil inhalation intervention. However, several scholars have indicated that aromatherapy did not show improvement on the emotions, physical syndromes, or QOL. 36,37 Of note, our data verified that lavender essential oil intervention significantly improved overall QOL as well as physical/mental functions in career women. Inconsistency in observing the effects of aromatherapy on overall QOL could be attributed to the disruption of pain or emotional factors that patients experienced during the course of their diseases in these clinical studies.
In this study, we observed that blended essential oils exhibited greater effectiveness on improvement of sleep quality than lavender essential oil. The varied effectiveness of these two essential oils might be due to distinct chemical compositions. Lavender essential oil mainly comprises linalyl acetate, it effectively improves sleep quality, further verifying the sedative and sleep-induced effects of this compound. 12,13 However, the blended oil in the present study comprised lavendel fein (L. angustifolia), muskatellersalbei (S. sclarea), and marjoram (O. majorana) essential oils, all of which contain linalyl acetate. In addition, muskatellersalbei contains 1%–3% sclareol, which is chemically similar to estrogen; hence, it enables balancing the female endocrine system. 14,15 In line with our recent findings, a previous study, comparing the effects of lavender and a blended oil (20:10:15:2 ratio of lavender, marjoram, ylang-ylang, and neroli), reported that the blended essential oil displayed more favorable effects on sleep quality enhancement in middle-aged women with insomnia. 38 Moreover, postoperative patients exhibited more satisfactory sleep quality after administrating blended essential oil (12:4:1 ratio of lavender, roman chamomile, and neroli oils). 39 However, it has to be noted that there are still very limited number of studies focusing on the biochemical and physiological mechanisms underlying the effectiveness of aromatherapy in the literature. Based on existing evidence and our results, we speculate that the blended oil might alleviate the physical and mental discomfort through correcting the endocrine imbalance, thereby enhancing QOL.
Acupressure massage has been proven to enhance sleep quality and/or QOL in various populations (e.g., hemodialysis patients, patients with end-stage renal disease, elderly nursing home residents, and menopausal women), 19,21,23,40 whereas there are no studies focusing on the effectiveness of acupressure massage on QOL and sleep quality in career women. In this study, we provided direct evidence that acupressure massage is effective in improving the overall QOL and sleep quality. Similar to previous findings, acupressure and meridian massage are effective in improving life quality and physical function. 41,42 Furthermore, acupressure massage has been reported to enhance the participant's vitality and emotional balance, thereby improving mental health. 42,43 In addition, several studies demonstrate the effectiveness of acupressure massage on ameliorating overall QOL. 42,44,45 However, Liang et al. reported that acupressure massage has no effect on sleep quality in nursing personnel with a rotating roster. 29 In this study, we must note that this is the first study involving career women and there are very limited studies with this population to make comparisons between results, although the distressing effect of both complementary modalities had been widely reported in women with cancer or menstrual cramps. Moreover, the existing studies for the effects of acupressure therapy on sleep quality are still inconclusive among varied populations. Further studies are thus warranted to determine whether their poor sleep quality was due to rotating shifts.
In this study, only 4 weeks of intervention were investigated, and it was still unknown how long these positive benefits on sleep quality and QOL would last. Another primary limitation of this study was the difficulty to perform blinding experimental design due to the distinguished nature of the selected interventions. Of note, our findings also raised a significant practical question whether the combination of acupressure and blended essential oil inhalation (consisting of L. angustifolia, S. sclarea, and O. majorana) would result in a synergistic effect to further improve sleep quality and QOL. Therefore, future studies are needed to investigate the combining effects of acupressure and aromatherapy and to compare the lasting effects of these complementary modalities using follow-up experimental design.
Conclusions
In this study, we demonstrated that the aromatherapy interventions in this study, which involved applying lavender or blended essential oil (consisting of L. angustifolia, S. sclarea, and O. majorana; three sessions/weeks; 20 min/session), and the acupressure massage (45 min/session/weeks) were effective to improve sleep quality and QOL in career women. Our results also further verify that blended essential oil aromatherapy has greater benefits on promoting both sleep quality and QOL, but acupressure massage only shows the effect on improving sleep quality. Taken together, our present findings provide scientific evidence-based information for the benefits of using various alternative modalities, including aromatherapy and acupressure massage, on improving sleep quality and overall QOL in career women.
Footnotes
Acknowledgments
The authors genuinely appreciate all those who participated in this study. They also sincerely thank the National Taipei University of Nursing and Health Sciences (NTUNHS) for providing the necessary resources and administration support throughout the study.
Authors' Contributions
Y.-H.K., Y.-C.H., U.-L.C., and Y.-H.L. conceived and designed the experiments. W.-N.H. and Y.-T.T. performed the experiments. Y.-H.K., Y.-C.H., U.-L.C., and Y.-H.L. analyzed the data. U.-L.C., W.-N.H., and Y.-T.T. contributed reagents/materials/analysis tools. Y.-H.K., Y.-C.H., and Y.-H.L. wrote the article.
Author Disclosure Statement
No competing financial interests exist.
Appendix
| Steps | The location of acupuncture points (WHO meridian alphabetic code) a | Massage methods × time(s) | Duration (minutes) | |
|---|---|---|---|---|
| 1 | Head | Bladder Meridian/Gallbladder Meridian: Tianzhu (BL10)/Fengchi (GB20) Wangu (GB12) | Pressing at a fixed point × 1 | 1 |
| 2 | Head | Governor Meridian: Yamen (GV15) to Baihui (GV20) | Toggling × 2 | 3 |
| 3 | Head | Bladder Meridian: Tianzhu (BL10) to Baihui (GV20) | Toggling × 2 | 3 |
| 4 | Head | Gallbladder Meridian: Fengchi (GB20) to Baihui (GV20) | Toggling × 2 | 3 |
| 5 | Head | Gallbladder Meridian: Wangu (GB12) to Baihui (GV20) | Toggling × 2 | 3 |
| 6 | Back | Governor Meridian: Dazhui (GV14) to Zhiyang (GV9) | Toggling × 2 | 3 |
| 7 | Back | Bladder Meridian: Dazhu (BL11) to Gushu (BL17) | Toggling × 2 | 2 |
| 8 | Back | Bladder Meridian: Fufen (BL41) to Geguan (B46) | Toggling × 2 | 2 |
| 9 | Neck and shoulder | Small Intestine Meridian: Jianzhongshu (SI15) to Tianzong (SI11) | Toggling × 2 | 2.5 |
| 10 | Neck and shoulder | Triple Energizer Meridian: Tianliao (TE15) | Toggling × 2 | 1.5 |
| 11 | Neck and shoulder | Gallbladder Meridian/Large Intestine Meridian: Jianjing (GB21)/Jugu (LI16) | Toggling × 2 | 3 |
| 12 | Arm | Large Intestine Meridian: Jianyu (LI15) to Shangyang (LI1) | Toggling × 2 | 3 |
| 13 | Arm | Triple Energizer Meridian: Jianliao (TE14) to Guanchong (TE1) | Toggling × 2 | 3 |
| 14 | Arm | Small Intestine Meridian: Naoshu (SI10) to Shaoze (SI1) | Toggling × 2 | 3 |
| 15 | Inner arm | Lung Meridian: Tianfu (LU3) to Shaoshang (LU11) | Toggling × 2 | 3 |
| 16 | Inner arm | Pericardium Meridian: Tianquan (PC2) to Zhongchong (PC9) | Toggling × 2 | 3 |
| 17 | Inner arm | Heart Meridian: Jiaquan (HT1) to Shaochong (HT9) | Toggling × 2 | 3 |
Along the aforementioned acupressure massage paths, each of the following acupuncture points is pressed for 3 sec: Wangu (GB12), Baihui (GV20), Tianzhu (BL10), Chengling (GB18), Fubai (GB10), Dazhui (DU14), Feishu (BL13), Xinshu (BL15), Jianzhongshu (SI15), Tianliao (TE15), Jianjing (GB21), Hegu (LI4), Waiguan (TE5), Houxi (SI3), Shaoshang (LU11), Neiguan (PC6), and Shenmen (HT7).
Data resource: World Health Organization (WHO, 2015).