
Abstract
Objectives:
Vasomotor symptoms (VMSs) are the most common symptoms reported during menopause. Although hormone therapy is effective for reducing VMSs, its use is restricted in some women. Many women with VMSs thus seek nonhormonal, nonpharmacologic treatment options such as acupuncture.
Design:
An umbrella systematic review (SR) was conducted, supplemented by a search of published randomized controlled trials (RCTs), that assessed the effectiveness of acupuncture for VMSs, health-related quality of life (HRQOL), and adverse effects of treatment in perimenopausal or postmenopausal women. Meta-analyses were conducted using a random-effects model when data were sufficient.
Results:
Three SRs and four new RCTs were identified that met eligibility criteria. Meta-analyses of this study revealed statistically significant standardized mean differences (SMDs) associated with acupuncture compared with no acupuncture at reducing VMS frequency (SMD −0.66, 95% confidence interval [CI] −1.06 to −0.26, I 2 = 61.7%, 5 trials) and VMS severity (SMD −0.49, 95% CI −0.85 to −0.13, I 2 = 18.1%, 4 trials) and improving HRQOL outcomes (SMD −0.93, 95% CI −1.20 to −0.67, I 2 = 0.0%, 3 trials). SMDs were smaller or not statistically significant when acupuncture was compared with sham acupuncture.
Conclusions:
Evidence from RCTs supports the use of acupuncture as an adjunctive or stand-alone treatment for reducing VMSs and improving HRQOL outcomes, with the caveat that observed clinical benefit associated with acupuncture may be due, in part, or in whole to nonspecific effects. The safety of acupuncture in the treatment of VMSs has not been rigorously examined, but there is no clear signal for a significant potential for harm.
Introduction
A
Hormone therapy is an effective treatment for reducing VMSs, but use of this therapeutic approach must be individualized by weighing benefits against known risks, such as cardiovascular events, liver disease, thromboembolism, or uterine and breast cancers. The median total duration of menopausal transition is >7 years. 6 Therefore, given the potential health risks posed by long-term hormone therapy use and the simultaneous need to alleviate persistent bothersome VMSs, nonhormonal treatment may be the only option for many women who experience moderate to severe VMSs.
Many perimenopausal and postmenopausal women are already using nonpharmacologic agents to manage VMSs, including herbal and nonhormonal medications. In 2015, the North America Menopause Society released a position statement providing recommendations for many such intervention types and graded the level of evidence for their recommendations; however, this was not a formal systematic review (SR) of the literature. 7 Also, a 2015 Agency for Healthcare Research and Quality (AHRQ) SR examined the comparative effectiveness of estrogens, isoflavones, selective serotonin reuptake inhibitors/serotonin–norepinephrine reuptake inhibitors, gabapentin, black cohosh, and ginseng for menopausal symptoms, including VMSs. 8 However, the AHRQ review did not address nonpharmacologic interventions such as acupuncture. Several randomized controlled trials (RCTs) and some SRs of acupuncture for the treatment of VMSs have been published, but there are no SRs that included recently published RCTs of acupuncture in the English-language, peer-reviewed literature.
In this article, the authors summarize and update the evidence from prior SRs on the use of acupuncture compared with active and inactive controls for the treatment of menopause-associated VMSs, health-related quality of life (HRQOL), and adverse effects of treatment among perimenopausal and postmenopausal women.
Materials and Methods
Study design
This review is part of a larger effort to assess the effects of nonpharmacologic, nonhormonal treatments for menopause-associated VMSs. The research question was developed after a topic refinement process that included a preliminary review of the literature, discussion with internal partners and investigators, and consultation with content experts and key stakeholders. The full technical report with results for all interventions evaluated is available at (
A standard, published protocol 10 was followed for all steps of this review using a method commonly known as an umbrella review, or a review of reviews. 11 This approach was supplemented by evaluating RCTs published from January 2012 to February 2016 for additional, recent RCTs not included in the SRs.
For this study, acupuncture from any tradition was considered, including auricular acupuncture, electroacupuncture, and laser acupuncture. Studies were excluded if acupuncture was administered in conjunction with Chinese herbal therapies. Cupping therapy was excluded unless it was a component of an acupuncture intervention.
Data sources and searches
In consultation with an expert librarian, searches were conducted on MEDLINE and the Cochrane Database of Systematic Reviews for recent SRs published from January 2010 to November 2015. Searches were also conducted on PubMed, EMBASE, CINAHL, and the Allied and Complementary Medicine Database from January 2012 to February 2016 to identify additional, pertinent RCTs not included in the eligible SRs. MeSH was used and free-text terms were selected for the interventions and health conditions of interest as well as terms for SRs and RCTs. All eligible SRs along with relevant umbrella and narrative reviews identified during citation screening were examined for relevant RCTs not yet identified. The search strategies are reported in Goldstein et al. 10
Study selection
Using prespecified inclusion/exclusion criteria (Table 1), two reviewers appraised titles and abstracts of identified SRs and RCTs for potential relevance to the key question. To be eligible, articles had to (1) evaluate the effectiveness of acupuncture in perimenopausal or postmenopausal women experiencing bothersome VMSs; (2) report effects on VMSs, QOL outcomes, psychological symptoms, or adverse effects; and (3) use a SR or RCT design. Articles included by either reviewer underwent full-text review for potential abstraction. For all phases of this process, including quality assessment, disagreements on articles were resolved by discussion or by a third reviewer.
HRQOL, health-related quality of life; RCT, randomized controlled trial; SR, systematic review; VMSs, vasomotor symptoms.
Data abstraction
Data were abstracted into a customized DistillerSR (Manotick, ON, Canada) database by one reviewer and overread by a second reviewer. Data elements included descriptors to characterize the type of study, study population, intervention, comparator, outcomes reported, study quality, and author conclusions.
Quality assessment
Two reviewers assessed the quality of SRs and newly identified RCTs. For SRs, the following key quality criteria were used, adapted from ROBIS 12 : search methods adequate for replication, selection bias avoided, data abstracted reliably, characteristics of primary literature reported and quality assessed appropriately, results synthesized using appropriate methods, publication bias assessed, conflict of interest reported, and conclusions supported by results. Based on these criteria, SRs were categorized as good, fair, or poor quality, with good- and fair-quality SRs providing sufficient information to assess the strength of the body of evidence using the GRADE criteria. 13 Poor-quality SRs were excluded from this review. For newly identified RCTs, the Cochrane Collaboration's risk of bias (ROB) tool was used, 14 which categorizes biases by six domains (selection bias, performance bias, detection bias, attrition bias, reporting bias, and other bias) and makes a summary assessment. The quality of individual RCTs included in the eligible SRs was not assessed.
Statistical analyses
When an updated or new meta-analysis was indicated and feasible based on the number of new studies with comparable outcomes and comparators, summary estimates of effect for each intervention were computed using end-of-treatment outcomes. When means and variance were not reported in the text, they were approximated from figures with the use of Engauge Digitizer. 15 To update meta-analyses, data used in prior SRs were confirmed and data from newly identified RCTs were incorporated.
R version 3.1.2 (R Foundation for Statistical Computing, Vienna, Austria) with the metafor package was used 16 to calculate random-effects model summary estimates of effect with Knapp and Hartung adjustment of standard errors of the estimated coefficients. 17,18 Because outcomes were measured across the trials using different instruments, outcome measures were combined using standardized mean differences (SMDs) in a random-effects model. The SMD was calculated by dividing the difference in mean values by the pooled standard deviations of the two groups. SMDs of 0.2 can be considered small treatment effects; 0.5, moderate effects; and ≥0.8, large effects. 19 Consistency of findings across individual studies was assessed by standard chi-square tests and the I 2 statistic.
Results
Study characteristics and risk of bias
Three eligible SRs were identified that evaluated the effectiveness of acupuncture for menopause-related VMSs. One was a good-quality Cochrane Collaboration SR by Dodin et al. 20 published in 2013, and two were fair-quality SRs 21,22 that provided qualitative summaries of RCTs published in 2013 and 2015. For the purposes of this analysis, the SR by Dodin et al.was focused 20 because it did not limit inclusion to trials of women with a history of cancer (as did the other two SRs), it included all but three RCTs also included in the other two SRs, it conducted pertinent meta-analyses, and it was judged to be of higher quality than the other two SRs.
Dodin et al. included 16 RCTs. 23 –38 Of these, one is not pertinent to this review because the study intervention was moxibustion alone. 24 The 15 relevant RCTs included 1127 women, and the minimum number of daily VMSs for inclusion in the trials was 2–7 in the eight RCTs that reported this inclusion criterion. All RCTs included perimenopausal or postmenopausal women. Five exclusively enrolled women who had recently completed treatment for breast cancer, and one included only women who had undergone bilateral oophorectomy. Duration of acupuncture treatments ranged from 4 to 12 weeks across the RCTs. Twelve RCTs employed standardized or semistandardized acupuncture treatment protocols, utilizing between 4 and 13 acupuncture points per treatment session. Three RCTs employed individualized treatment plans. Although the SR did not address durability of treatment effect, 6 of the 15 relevant trials reported durability of effect at 3–12 months.
Four new, relevant RCTs (696 participants) published after 2012 were identified that assessed the impact of acupuncture on VMSs or QOL outcomes among perimenopausal or postmenopausal women. 39 –42 All were judged to have low ROB. Two of the four RCTs were two-arm trials comparing acupuncture with no acupuncture 41 and comparing acupuncture with sham. 39 One RCT was a four-arm trial involving 120 breast cancer survivors experiencing bothersome hot flashes that compared gabapentin, placebo gabapentin, 10 treatments (8 weeks) of acupuncture, and sham acupuncture. 40 The fourth RCT randomized postmenopausal women to 12 weeks of acupuncture, sham acupuncture, Chinese herbal medicine, or placebo herbal medicine. 42 Table 2 summarizes the study characteristics of the RCTs.
QOL, quality of life.
Frequency and severity of VMSs
Acupuncture versus no acupuncture or usual care
The SR by Dodin et al. 20 included a meta-analysis of three trials that compared acupuncture with no acupuncture, the results of which demonstrated a statistically significant effect associated with acupuncture for both VMS frequency (SMD −0.50, 95% confidence interval [CI] −0.69 to −0.31, I 2 = 0.0%) and severity (SMD −0.54, 95% CI −0.73 to −0.35, I 2 = 0.0%) compared with no acupuncture. A meta-analysis reported in the review also suggests that QOL outcomes, as assessed by the Women's Health Questionnaire, Menopausal Rating Scale, or the Menopause Specific Quality of Life Questionnaire, are improved with acupuncture (SMD −0.93, 95% CI −1.20 to −0.67, I 2 = 32%, 3 trials) compared with no acupuncture. Subgroup and sensitivity analyses were not performed.
The meta-analysis reported in the SR was updated by adding both the results at the end of treatment from Avis et al. 41 and the results of the no acupuncture group at the end of treatment from the three-arm RCT by Avis et al. 35 in the SR by Dodin et al. 20 (which was not included in the meta-analyses of acupuncture vs. no acupuncture in that SR). In the authors' updated meta-analysis, acupuncture was associated with decreased VMS frequency (SMD −0.66, 95% CI −1.06 to −0.26, I 2 = 61.7%, 5 trials; Fig. 1) and decreased VMS severity (SMD −0.49, 95% CI −0.85 to −0.13, I 2 = 18.1%, 4 trials; Fig. 2). Acupuncture resulted in a statistically significant decrease in hot flash frequency at 6 months, and maintained at 12 months after baseline. 41

Forest plot of acupuncture versus no acupuncture on change in hot flash frequency at end of treatment. CI, confidence interval; SD, standard deviation; SMD, standardized mean difference.

Forest plot of acupuncture versus no acupuncture on change in hot flash severity at end of treatment. CI, confidence interval; SD, standard deviation; SMD, standardized mean difference.
Acupuncture versus sham acupuncture
Dodin et al. 20 conducted meta-analyses using data from eight trials that compared acupuncture with a sham control and reported daily VMS frequency or severity. 23,25,26,28 –30,35,38 These meta-analyses revealed no significant difference for daily VMS frequency (SMD −1.13, 95% CI −2.55 to 0.29, I 2 = 70%) but significantly improved severity of hot flashes (SMD −0.45, 95% CI −0.84 to −0.05, I 2 = 62%) compared with sham acupuncture. Subgroup analyses demonstrated that heterogeneity was partially explained by the trials involving women with breast cancer and trials with duration of treatment less than or greater than 12 weeks.
Three new trials that compared acupuncture or electroacupuncture with sham acupuncture were identified. In an RCT by Mao et al., 40 electroacupuncture (which involves administering low-dose electrical current through some of the acupuncture needles) reduced the hot flash composite score at 24 weeks by 7.4 units compared with 5.9 with sham electroacupuncture, 5.2 with gabapentin, and 3.4 with the placebo medication (p < 0.001). In an RCT by Ee et al., 39 hot flash scores decreased in both groups by ∼40% from baseline to the end of acupuncture treatment and were sustained for 6 months. There was no evidence of an advantage of acupuncture over sham acupuncture on QOL outcomes. In the new RCT by Nedeljkovic et al., 42 acupuncture was more effective than sham acupuncture in reducing hot flash frequency and severity, and in improving menopause-related QOL outcomes.
The meta-analysis reported in the SR was updated by adding findings from these three new RCTs. 39,40,42 The authors' updated meta-analysis generated an estimate of the SMD of −0.21 (95% CI −0.49 to 0.07, I 2 = 53.5%, 10 trials) for reduction in VMS frequency (Fig. 3) and −0.35 (95% CI −0.70 to 0.01, I 2 = 66.5%, 8 trials) for reduction in VMS severity (Fig. 4).
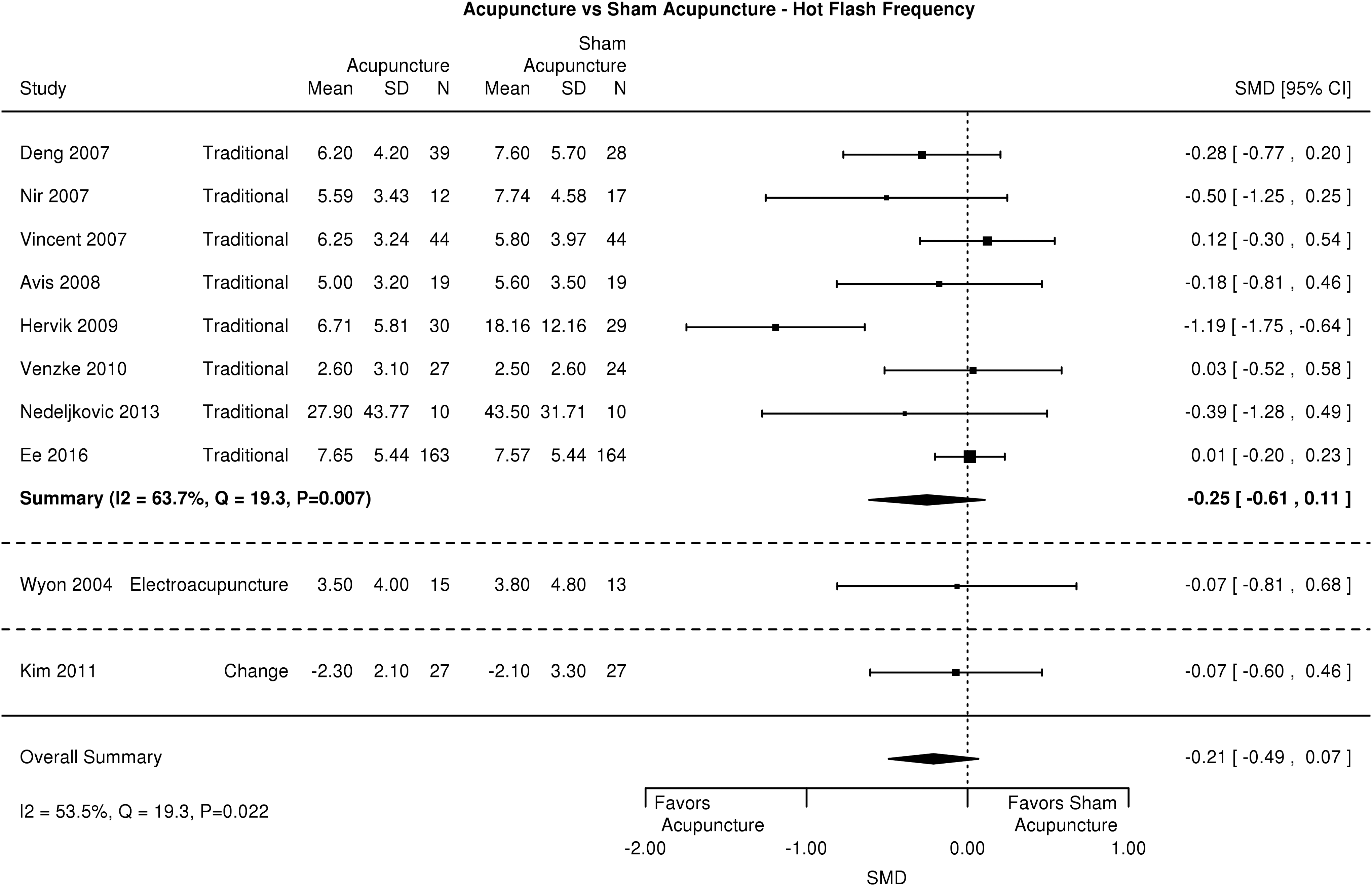
Forest plot of acupuncture versus sham acupuncture on change in hot flash frequency at end of treatment. CI, confidence interval; SD, standard deviation; SMD, standardized mean difference.
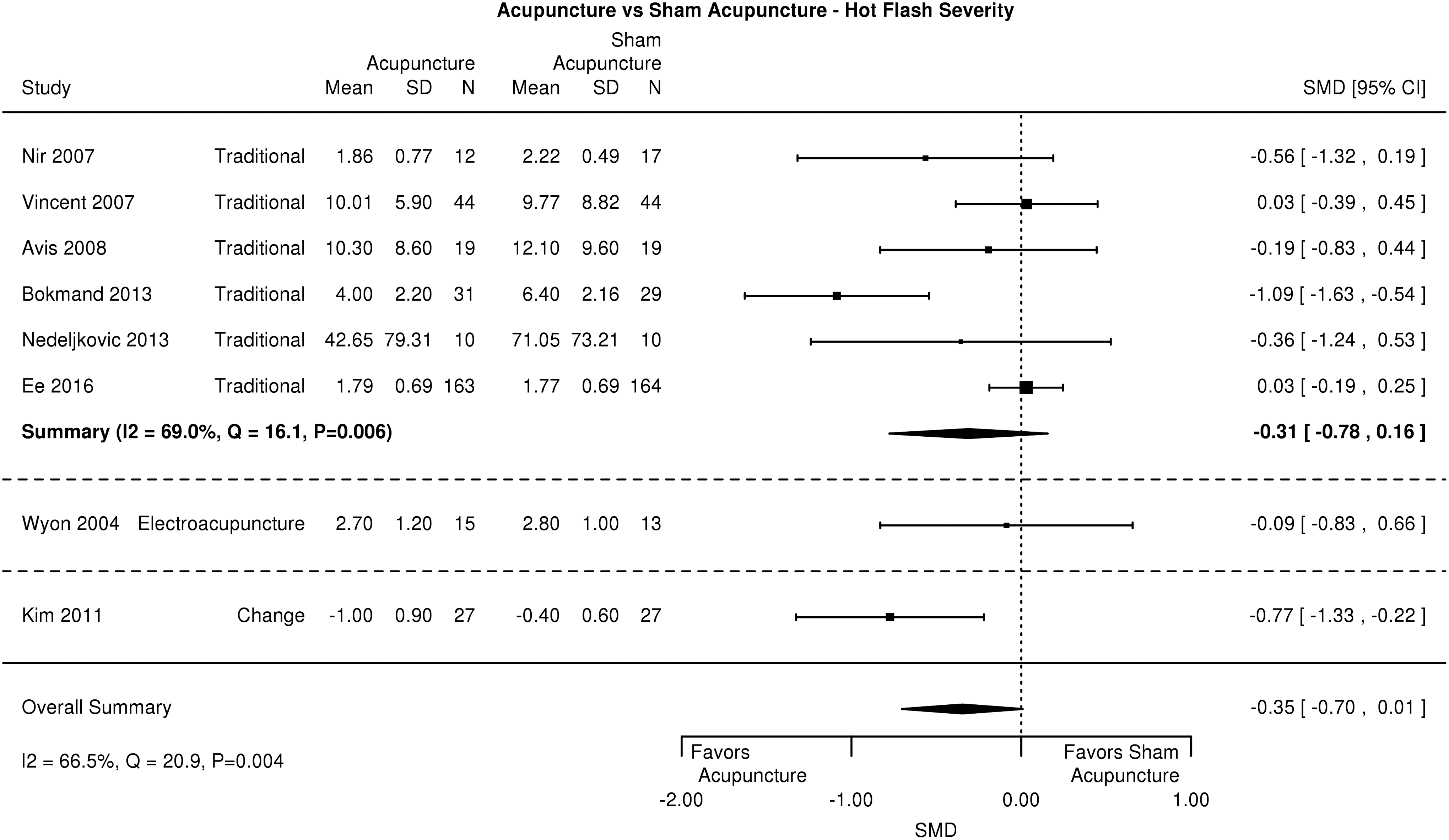
Forest plot of acupuncture versus sham acupuncture on change in hot flash severity at end of treatment. CI, confidence interval; SD, standard deviation; SMD, standardized mean difference.
Acupuncture versus hormone therapy
The SR by Dodin et al. included three RCTs that compared acupuncture with hormone therapy. 36 –38 Among these, acupuncture was associated with significantly higher daily VMS frequency compared with hormone therapy (SMD 3.18, 95% CI 2.06 to 4.29, I 2 = 0%, 3 trials). There was no statistically significant differences in VMS severity between acupuncture and hormone therapy (SMD 0.53, 95% CI −0.14 to 1.20, 2 trials).
Acupuncture versus relaxation
A single RCT 31 included in the SR compared electroacupuncture with relaxation, finding no significant differences between both groups on either daily VMS frequency (MD −0.40, 95% CI −2.18 to 1.38) or severity (MD 0.20, 95% CI −0.85 to 1.25). Any new RCTs that compared acupuncture with relaxation were not identified.
Health-related quality of life outcomes
Two of the RCTs 23,25 included in the SR by Dodin et al. 20 found no significant difference in HRQOL (as assessed by the Menopausal Specific Quality of Life questionnaire or the Greene Climacteric Scale) between acupuncture and sham acupuncture (SMD 0.11, 95% CI −0.33 to 0.55). The authors' updated meta-analysis that included results of changes in the Menopause Specific Quality of Life questionnaire in two of the new RCTs 41,43 generated an SMD of −0.23 (95% CI −1.40 to 0.95, I 2 = 77.0%, 5 trials) for change in HRQOL (Fig. 5).
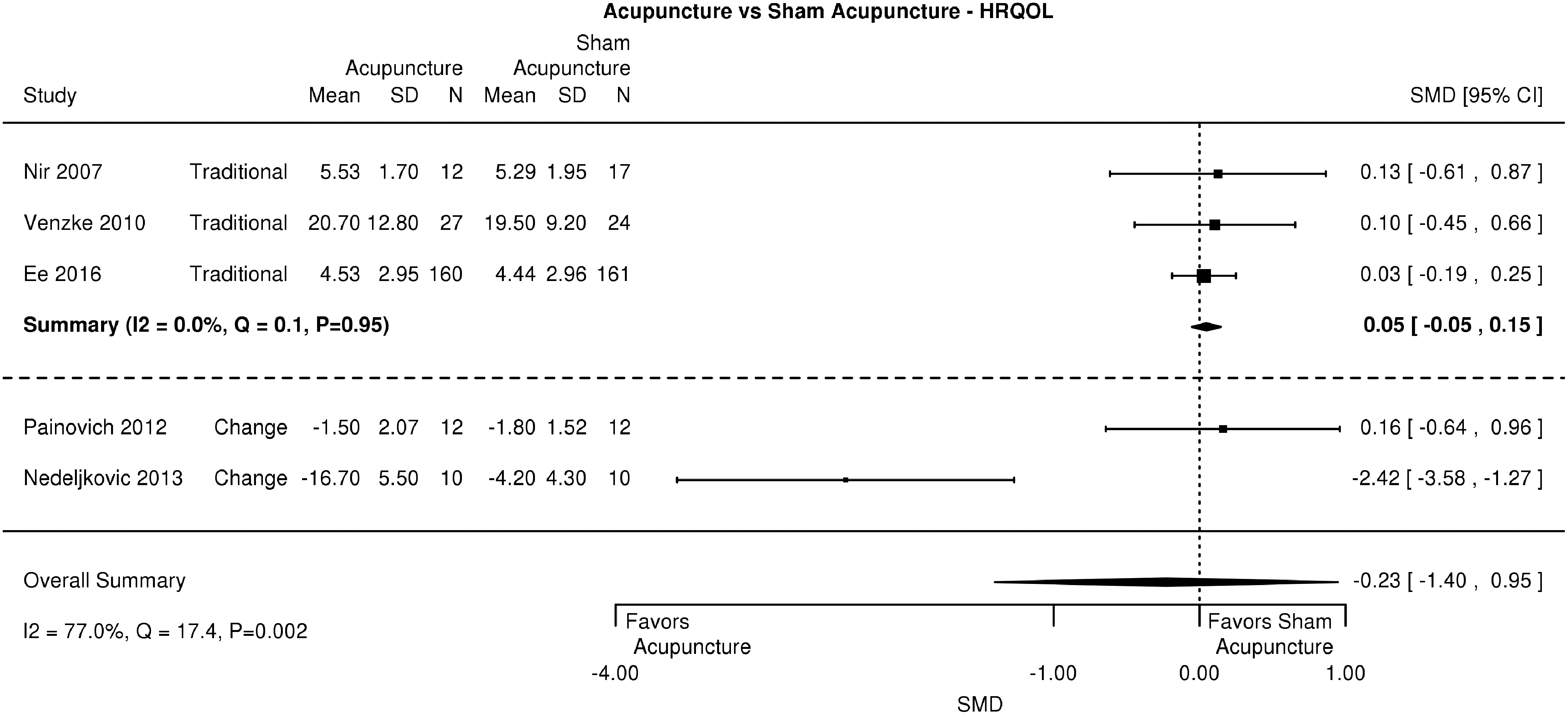
Forest plot of acupuncture versus sham acupuncture on change in quality of life at end of treatment. HRQOL, health-related quality of life; SD, standard deviation; SMD, standardized mean difference.
Acupuncture versus hormone therapy
HRQOL as assessed by the Kupperman Index was significantly greater in the hormone therapy group than in the acupuncture group (SMD 0.11, 95% CI 0.01 to 0.21, 1 trial) in the single study included in the review by Dodin et al. that reported this outcome. 37 New RCTs that compared acupuncture with hormone therapy were not identified.
Adverse effects
All of the adverse effects reported in the new RCTs were graded as mild. Among the 327 patients allocated to either true or sham acupuncture in the RCT by Ee et al., 39 8 (2%) reported bleeding or bruising, 7 (2%) reported pain, 3 (1%) reported syncope or presyncope, 3 (1%) reported worsening of symptoms, 1 reported tingling near an acupuncture point, 1 reported swelling around an acupuncture point and itching of the whole arm, 1 reported skin sensitivity and feeling hot, 1 reported nervousness, and 1 reported essential tremor. The RCT by Mao et al. 40 reported 5 (17%) adverse effects in the acupuncture arm, 1 (3%) in the sham arm, 8 (27%) in the placebo pill group, and 13 (43%) in the gabapentin arm (p value across the 4 groups was 0.005). A single adverse event in the form of pain sensation at the site of needle insertion was reported in the sham acupuncture group in the RCT by Nedeljkovic et al. 42 Adverse effects were not reported in the RCT by Avis et al. 41 Adverse effects, if any, reported in the RCTs included in eligible SR were not discussed by Dodin et al. 20
Discussion
Strengths and limitations of the umbrella review
The novel approach of supplementing a review of SRs with findings from recently published RCTs allowed us to synthesize both quantitatively and qualitatively the most current information on acupuncture as a nonpharmacologic, nonhormonal intervention for VMSs. A significant limitation to this approach is that the authors of this study relied on the SR authors' judgments on the appropriateness of their search strategies, eligibility criteria, and synthesis of the evidence. This review was limited to English-language publications, which may have excluded potentially informative evidence. The authors also limited reporting of outcomes of interest to VMSs, HRQOL, and adverse events, but other outcomes such as sleep quality, psychological symptoms, and other patient-reported outcomes were evaluated and reported in some included studies.
Limitations of the RCTs
Approximately half of the acupuncture trials used sham acupuncture controls. The purpose of a sham procedure or attention control is to evaluate whether the mechanisms of action for a given intervention's involve physiological processes that are independent of nonspecific effects that can be attributed to healthcare providers' care and attention or individual patients' beliefs and expectations. In the case of acupuncture, there is considerable debate about the appropriate control. 43,44 Some argue that sham procedures may not be physiologically inert, and that a usual care arm may be a more appropriate comparison for trials that aim to inform clinical practice, as opposed to determining the specific effects of an intervention.
Conclusions
Compared with usual care controls, evidence from RCTs supports the use of acupuncture for reducing VMSs and the impact of such symptoms on women's activities and HRQOL. The safety of acupuncture in the treatment of VMSs has not been rigorously examined, but there is no clear signal for a significant potential for harm. The authors conclude that the evidence supports the use of acupuncture as an adjunctive or stand-alone treatment in the treatment of menopause-related VMSs with the understanding that observed clinical benefit associated with acupuncture may be due in part or in whole to nonspecific effects.
Footnotes
Acknowledgments
The authors thank the members of the technical expert panel and organizational stakeholders: Nancy Avis, PhD (Wake Forest); Veronica Ades, MD, MPH (Veterans Affairs or VA); Lori Bastian, MD, MPH (VA); Margery Gass, MD (Executive Director, North American Menopause Society); Tracy Gaudet, MD (VA); Andrea LaCroix, PhD (Chair, Women's Health Center of Excellence, University of California, San Diego); Laurie Zephyrin, MD, MPH, MBA, Director, Reproductive Health Office of Patient Care Services; and Jodie Katon, PhD, MS. They also thank Liz Wing, MA, of the Duke Clinical Research Institute for editorial assistance. This study was funded by VA Evidence-based Synthesis Program (No. 09-010), VA Health Services Research and Development Career Development Award (No. 13-263) (Dr. Goldstein), and VA OAA Health Services Research and Development PhD Fellowship (TPP 21-027) (Dr. Shephard-Banigan).
Disclaimer
The findings and conclusions in this document are those of the author(s) who are responsible for its contents; the findings and conclusions do not necessarily represent the views of the Department of Veterans Affairs or the United States government. Therefore, no statement in this article should be construed as an official position of the Department of Veterans Affairs. This article is part of a larger project undertaken by the Evidence-based Synthesis Program (ESP) Center at the Durham Veterans Affairs (VA) Healthcare System in Durham, NC. The full report will be published on U.S. Department of Veteran Affairs Health Services Research & Development Evidence-based Synthesis Program at: (
Author Disclosure Statement
All authors declare that they have no competing interests or conflicts of interest.