
Abstract
Objectives:
A tribomechanically activated clinoptilolite (natural aluminosilicate mineral) has been used to increase growth in meat-producing animals, as an adjuvant in cancer therapy, and a heavy metal remover in humans. Because of its unique cation exchanging and chelating properties, we hypothesized that clinoptilolite may be beneficial for the treatment of dyslipidemia in the manner similar to bile acid sequestrants. Thus, specific aims of this pilot study were to orally administer clinoptilolite in different doses and granule size combinations to determine magnitude and time profile of changes in blood lipids.
Design:
A phase I/IIa prospective, open-label, uncontrolled, dose/granule size-ranging study (treatment phase 8 weeks, follow-up 6 weeks). Blood lipids were examined every 2 weeks.
Settings:
Outpatient clinic of a university-affiliated hospital.
Subjects:
Forty-one subjects (all white, mean age 57.6 ± 6.8 years, 17 women) with blood lipids above the normative limits divided into three groups.
Intervention:
A tribomechanically activated clinoptilolite was administered in three dose/grind combinations: 6 g/day of fine grind (6gF), 6 g/day of coarse grind (6gC), and 9 g/day of coarse grind (9gC).
Outcome measures:
Blood concentrations of total cholesterol (TC), low-density lipoprotein cholesterol (LDLc), high-density lipoprotein cholesterol (HDLc), and triglycerides (TG).
Results:
For the 3 groups combined, all lipid fractions significantly improved after 8 weeks of treatment (20–25%, p < 0.001), which reversed to baseline after 6 weeks of clinoptilolite withdrawal. Early (week 2) and the most pronounced decrease in TC and LDLc was observed in the 6gF group (19% and 23% in week 8, respectively), with no difference in HDLc and TG between the three dose/grind groups. No side effects were reported.
Conclusions:
These pilot results suggest that oral administration of clinoptilolite may improve lipid profile in individuals with dyslipidemia, which warrants further investigations.
Introduction
C
The two critical steps in cholesterol metabolism are the absorption of dietary and biliary cholesterol in the gut and the production of cholesterol in the liver, intestine, muscle, and skin. Statins act by reducing cholesterol synthesis in the liver, which leads to upregulation of hepatic LDLc receptors and increased uptake of LDLc from the blood. Statins have been proven to be efficacious in primary 3 and secondary 4 prevention of cardiovascular disease, but may have some side effects, ranging from mild (muscle aches, 5 increased liver transaminases 6 ) to serious (myopathy, 7 rhabdomyolysis 8 ).
Nonstatin drugs can also lower LDLc and reduce coronary heart disease. 9 Fibrates (peroxisome proliferator-activated receptor agonists) have proved successful when used alone, 10 but provide no incremental benefit if LDLc is already controlled by statins. 11 Bile acid sequestrants (e.g., colesevelam) and inhibitors of cholesterol resorptions (ezetimibe) interfere with the gut absorption and can be beneficial alone or in combination with statins. 12,13
Complementary therapy has also been explored for treatment of dyslipidemia. Plant sterols and stanols can reduce TC, LDLc, and TG, 14 particularly if TG levels are high. 15 Omega-3 fatty acids can also lower TG alone or when combined with statins, 16 but may elevate LDLc. 17 Daily intake of almonds (60 g for 4 weeks) have been shown to reduce LDL and TC in individuals with mild hypercholesterolemia. 18 In persons with type II diabetes, sour tea Hibiscus sabdariffa was found to decrease TC, LDLc, and TG, and increase HDLc. 19 The same has been reported for leaf tea Melothria maderaspatana in mild-to-moderate hypertension. 20
Red yeast rice, a Chinese food supplement produced by fermenting white rice, contains monacolin K, which is chemically identical to lovastatin. Two reviews concluded that red yeast rice significantly lowers TC and LDLc (1 mmol/L or 20%), has mixed effects on HDLc and TG, but may lead to anaphylaxis, toxic hepatitis, or rhabdomyolysis. 21,22 Berberine, another Chinese herbal compound, may also decrease LDLc (25%), TC (30%), and TG (35%) after 3 months of intake. 23 A probiotic yeast, Saccharomyces boulardi, has been found to reduce remnant lipoprotein particles by about 15%. 24
Clinoptilolite is a naturally occurring aluminosilicate mineral with unique structure and biochemical properties. 25,26 It is composed of a honeycomb framework of micropores (2–50 nm) that are negatively charged. This negative charge is balanced by exchangeable sodium, potassium, or calcium cations, which can be displaced easily by other cations. The internal surface area of micropores available for cation exchange is 10–300 m2/g, making canals and free spaces capable of trapping molecules (“molecular sieving” 25 ). Because of exceptional chelating properties, clinoptilolite has been used for treating soil and water contaminated with heavy metals and radioactive materials. 26 –28 It has also been supplied to food to increase growth and health of meat-producing animals. 25 In humans, clinoptilolite has been used as adjuvant in cancer therapy; heavy metal remover; hemostatic, antimicrobial, antioxidant, and antidiarrheal agent; and skin regeneration and immune system stimulant. 29 No side effects have been reported in humans after up to 8 weeks of oral intake, perhaps owing to minimal resorption from the gut, minimal solubility within the physiological pH range, and no changes in mineral and vitamin content. 30,31 In persons with immunodeficiency, however, Megamin supplement (3.6 g) significantly increased CD4+, CD19+, and HLA-DR+ lymphocyte counts and decreased CD56+ count, whereas Lycopenomin (1.2 g) significantly increased CD3+ and decreased CD56+ cells.
Considering its ion exchange properties, we hypothesize that clinoptilolite may change ionic content, pH, and buffering capacity of the gastrointestinal secretions, creating a less favorable environment for cholesterol absorption. Due to chelating properties, clinoptilolite may also act as bile acid sequestrants and interfere with micellar adaptation of intestinal cholesterol, effectively reducing its absorption into enterocytes. This would presumably reduce the amount of cholesterol delivered to the liver, upregulate hepatic LDLc receptors, increase LDLc uptake into hepatocytes, and decrease LDLc concentration in the blood.
The purpose of this pilot study was to determine the preliminary efficacy of clinoptilolite in persons with dyslipidemia. The specific aims were to orally administer clinoptilolite in different doses and granule size compositions to examine magnitude and time profile of changes in blood lipids during 8 weeks of treatment and for 6 weeks after treatment withdrawal.
Materials and Methods
Subjects
Subjects were recruited among patients receiving care at the authors’ institution. The inclusion criteria were age ≥18 years, TC >6.5 mmol/L or LDLc >4.1 mmol/L, and no plans to change diet, lifestyle, or physical activity over the next 3 months. The exclusion criteria were use of medication for dyslipidemia, history of congestive heart disease or arrhythmia, chronic renal failure or renal transplant, malignancy, cognitive dysfunction (The Mini-Mental State Exam score <19), depression (The Patient Health Questionnaire score >4), and, for women, pregnancy or plans to become pregnant over the next 3 months. The criteria for terminating the study were serious side effects, newly diagnosed disease, or physician order to change already prescribed medication (e.g., diabetes, hypertension). The study was approved by the Ethics Committee of our institution and all subjects signed the informed consent.
Study design
This was a phase I/IIa prospective, open-label, uncontrolled, dose/granule size-ranging study, with the treatment phase lasting 8 weeks and the follow-up phase lasting 6 weeks after the treatment withdrawal. Such treatment and withdrawal periods were selected because of no a priori knowledge about the time profile of postulated changes. Based on the recruitment order, the subjects were prospectively assigned to one of the three treatment groups in blocks of five, provided with the appropriate clinoptilolite formulation, and instructed about dosing. The subjects were instructed to contact the study investigators if any change in health was noted. Follow-up visits were scheduled for every 2 weeks.
Intervention
A tribomechanically activated clinoptilolite was prepared by the company which distributes clinoptilolite locally for human and animal consumption. The process of tribomechanical activation (heating, grinding, sifting, classifying) results in finely ground powder with particles ≤50 μm in size.
Since biological activity of clinoptilolite is believed to be inversely related to a particle size, two fineness of clinoptilolite grind were used in this study (hereto termed fine and coarse). The grind composition was verified by an independent laboratory certified in geological analysis according to the ISO11277:2009 standards. The examined samples of fine grind contained 85.7% of particles ≤10 μm in size (28.0% <2 μm, 37.0% 2–5 μm, 20.7% 5–10 μm) and 14.3% of >10 (14.1% 10–20 μm, 0.2% >20 μm). The coarse grind contained 61.5% of particles ≤10 μm in size (16.4% <2 μm, 22.5% 2–5 μm, 22.6% 5–10 μm) and 38.5% >10 μm (28.0% 10–20 μm, 10.5% >20 μm). The fine grind was administered at a morning dose of 6 g/day and the coarse grind at doses of 6 and 9 g/day (hereto referred to as 6gF, 6gC, and 9gC). Similar doses have been used in humans before. 32 The sample examined by the government-accredited agency using X-ray diffraction method showed that clinoptilolite accounts for 92% of the mineral content.
Assessment
At each visit, the subjects were asked about changes in diet, lifestyle, or physical activity over the prior 2 weeks. Potential side effects were assessed by asking subjects an open-ended question about changes in their health since the last visit and the responses were noted. The subjects were also questioned about the adherence to prescription. Overnight fasting blood was taken and sent for laboratory analysis.
Outcomes and hypotheses
The outcomes included blood concentrations of TC, LDLc, HDLc, and TG. The first hypothesis was that TC, LDLc, and TG will significantly decrease and HDLc will significantly increase after 8 weeks of treatment, with the values at 6 weeks after treatment withdrawal no longer significantly different from baseline. It was further hypothesized that the magnitude (hypothesis 2) and time profile (hypothesis 3) of changes in blood lipids will be different between 3 dose/grind combinations. In secondary analyses, time to response, peak response, and maintenance of response upon treatment withdrawal were examined for each dose/grind combination. The side effects were counted.
Statistical analyses
Demographic data were summarized for descriptive purposes. All analyses were run for each lipid fraction separately. The first hypothesis was tested on all subjects combined using a one-way repeated measure ANOVA across the three main time points (before treatment, end of treatment, end of follow-up). If ANOVA was significant, two planned pairwise comparisons with Bonferroni's correction were made under the hypothesis of significant differences between the pretreatment and posttreatment, but not between the pretreatment and follow-up.
Before between-group comparisons, baseline differences were evaluated using ANOVA with Bonferroni's correction for multiple comparisons. To determine whether the magnitude of changes differed between 3 dose/grind combinations (hypothesis 2), a mixed 3 × 3 ANOVA was used with group (6gF, 6gC, 9gC) as the between-factor and time as the within-factor (pre, post, follow-up), examining the significance of group-by-time interaction. If significant, planned pairwise comparisons with Bonferroni's correction were run to determine if the percent change from baseline was different between three dose/grind groups. For hypothesis 3 (time-profile difference), data were converted to a percent baseline. Another mixed ANOVA was run with group (6gF, 6gC, 9gC) as the between-factor and time as the within-factor (all 8 time points included), examining the significance of group-by-time interaction. If significant, planned pairwise comparisons with Bonferroni's correction followed.
Secondary analyses were conducted for each group separately using Dunnett's pairwise comparisons to determine the onset of effect (first time point significantly different from baseline), peak effect (time point showing the largest significant difference from baseline), and maintenance of effect (last time point after treatment withdrawal still significantly different from baseline). The results are presented as mean ± standard deviations and the illustrations show mean ± standard errors. p < 0.05 was considered significant.
Results
The sample included 41 subjects (all white, age 57.6 ± 6.8 years, 17 women; see Table 1 for demographics of each group). Due to slow recruitment, 11 instead of 15 subjects were included in the 9gC group. Antihypertensive medication was taken by five subjects in the 6gF group and four subjects in the 6gC group. One subject in the 6gC group was treated for type II diabetes.
Compliance and side effects
All subjects returned for all study visits. They reported taking the prescribed treatment regularly and no changes in diet, lifestyle, or physical activity throughout the study. No side effects were reported.
Comparison between pretreatment, posttreatment, and follow-up for all subjects combined (hypothesis 1)
One-way ANOVA revealed significant changes in each lipid fraction over the main study time points when all data were analyzed together (p < 0.001). The Bonferroni comparisons between the pre- and posttreatment indicated significant decrease in TC, LDLc, and TGL (p < 0.001), and significant increase in HDLc (p < 0.001) after 8 weeks of clinoptilolite intake (Table 2). At the end of follow-up, the results were no longer significantly different from baseline.
p < 0.001.
LDL, low-density lipoprotein; HDL, high-density lipoprotein.
Comparison of pretreatment to posttreatment and follow-up between groups (hypothesis 2)
At baseline, only LDLc was significantly higher in the 6gF group than the other two groups (p < 0.05). Regarding hypothesis 2, ANOVA revealed a significant group-by-time interaction for TC and LDLc (p < 0.001), but not for HDLc (p = 0.150) or TG (p = 0.579) (Fig. 1).

Blood concentrations of total cholesterol, LDL cholesterol, HDL cholesterol, and triglycerides before treatment (Pre), after 8 weeks of treatment (Post), and 6 weeks after treatment withdrawal (follow-up) for 6gF, 6gC, and 9gC groups (mean ± SE values shown). LDL, low-density lipoprotein; HDL, high-density lipoprotein.
The significant interaction for TC was associated with a greater decrease in the 6gF group (19% on average) compared with the 9gC group (16%, p < 0.01) and 6gC group (12%, p < 0.001) at the end of treatment. The significant interaction for LDL was also due to a greater decrease in the 6gF group (23%) than in the 6gC and 9gC groups (17% and 16%, respectively, p < 0.01). At the end of follow-up, TC, LDLc, HDLc, and TGL were not different from baseline in any group.
Comparison of time profile of changes between groups (hypothesis 3)
To determine if the pattern of change over the course of study was different between the 3 groups, the significance of group-by-time interaction was examined. This interaction was significant for TC (p < 0.001), LDLc (p = 0.046), and HDLc (p = 0.017), but not TG (p = 0.809) (Fig. 2).
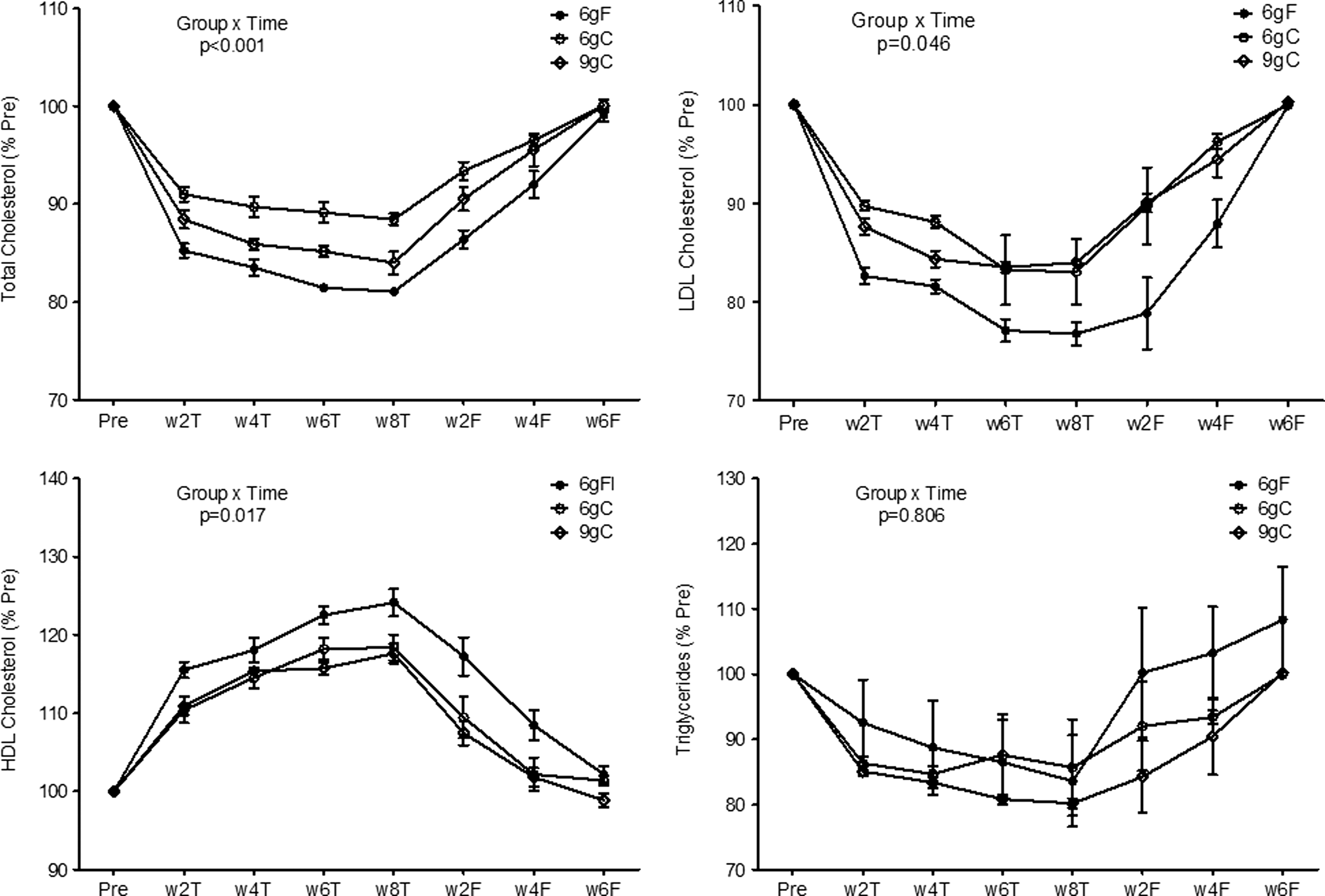
Time profile of changes in blood lipids during 8 weeks of treatment and 6 weeks of follow-up expressed as a percentage of pretreatment values (mean ± SE values shown).
The Bonferroni-corrected comparisons showed that TC in the 6gF group was significantly lower than in the 6gC group between weeks 2 and 8 of the treatment (p < 0.001), and lower than in the 9gC group at week 2 after treatment withdrawal. The group-by-time interaction was also significant for LDLc due to a slower return to baseline in the 6gF group than the other two groups after treatment withdrawal (significantly lower LDLc in 6gF vs. 6gC group at weeks 2 and 4, and 6gF vs. 9gC group at week 2). Similar pattern, but in the opposite direction, was found for HDL (significantly higher HDLc in 6gF vs. both 6gC and 9gC groups at week 2 of the follow-up). Short of significant group-by-time interaction for TG, pairwise tests were not run.
Onset, peak, and maintenance of effect in different groups (secondary analysis)
The Dunnett's comparisons against baseline showed that in all three groups TC and LDLc significantly decreased already at week 2 and peaked at week 8 after starting the treatment. These effects were maintained following the treatment withdrawal for 4 weeks in the 6gF group, for 2 weeks in the 9gC group, but disappeared immediately in the 6gC group. In terms of the increase in HDLc, the same time profiles as above were observed in the 6gF and 9gC groups during the treatment, but HDLc declined in the 9gC group immediately after stopping the treatment. In the 6gC group, however, HDLc increase was delayed until week 6 and peaked at week 8, but then immediately disappeared after ending the treatment. Regarding TG, only the 9gC group showed significant decrease starting at 2 weeks, peak effect at 8 weeks, and retention for 2 weeks after ending the treatment.
Discussion
This study shows that oral administration of clinoptilolite in doses up to 9 g for 8 weeks is efficacious for temporarily improving lipid profile in people with dyslipidemia. Some of the improvements were dependent on the formulation, such that lower dose and finer grind of clinoptilolite (6gF) resulted in greater changes in TC and LDLc, but not HDLc and TG, after 8 weeks of treatment. Also, the effects on TC, LDLc, and HDLc developed sooner and lasted longer with the 6gF treatment.
When analyzed for the 3 dose/grind groups together (hypothesis 1), the improvements in lipid profile after 8 weeks of clinoptilolite intake ranged, on average, from 0.37 mmol/L for TG to 1.18 mmol/L for LDLc (Table 2), which corresponded to about 20% to 25% change from baseline (−18% TC, −24% LDLc, +20% HDLc, −22% TG). This brought the average HDLc and TG, but not TC and LDLc, within the normative limits. The comparison between different dose/grind combinations (hypothesis 2, Fig. 1) showed the greatest decrease in TC and LDLc with 6 g of finely ground clinoptilolite (6gF). This result has to be interpreted in the context of significantly greater baseline levels of LDLc (but not TC) in the 6gF group compared with the other two groups. Thus, the effect of clinoptilolite may also depend on the initial severity of dyslipidemia, which needs to be studied further. Conversely, the three studied dose/grind combinations seem comparably efficacious for normalizing HDLc and TG.
The time profiles of relative changes in TC, LDLc, and HDLc (but not TG) proved different between the three dose/grind combinations (hypothesis 3). The decrease in TC occurred sooner after starting treatment (week 2) and was more profound with the 6gF and 9gC than 6gC formulation (Fig. 2). Despite no difference in onset, the decrease in LDLc and increase in HDLc with the 6gF formulation outlasted the effects of both 9gC and 6gC formulations for 2 and 4 weeks, respectively.
The changes in lipid concentrations with clinoptilolite were either similar to or lower than what has been reported previously for statins. About 25% decrease in LDLc reported in this study is similar to the effects of 40 mg of fluvastatin, 10–20 mg of lovastatin, 20–40 mg of pravastatin, and 10 mg of simvastatin (20–30% decrease), 33 but it is lower than the effect of 10 mg of atorvastatin (37%) 34 or rosuvastatin (46%). 35 The decrease in LDLc with clinoptilolite is similar to 10 mg/day of standardized monacolin extracts, 36 but higher compared with phytosterol therapy (11%). 37 The 20% increase in HDLc reported in this study is higher compared with statins (2–10%) and fibrates (5–15%), but lower compared with niacin (up to 30%). 38
No side effects were reported in this sample. We were concerned about possible gastrointestinal side effects if clinoptilolite acted as bile acid sequestrants, which often cause constipation, 39 but this was not the case. However, since the design of this study only permitted evaluation of preliminary efficacy, more rigorous safety studies are needed before concluding that clinoptilolite in doses of up to 9 g may be considered safe for human use. Potential safety concerns include negative effects on the lungs (fibrosis, mesothelioma), central nervous system (neurotoxicity associated with aluminum), and gastrointestinal system (interference with absorption of minerals and fat-soluble vitamins), and specifically in the context of dyslipidemia, whether intake of clinoptilolite may cause weight gain.
The results of this pilot study lend support for a randomized control trial and can be used to estimate a sample size. The effect size estimates, derived from the results across all doses/grind combinations (Table 2), are 2.1 for TC, 1.6 for LDLc, 1.4 for HDLc, and 0.8 for TG. Since uncontrolled studies tend to overestimate the effect size, reducing it for 25% yields an estimate of 1.2 for LDLc, which is most likely to serve as the primary endpoint. Under these assumptions, the two groups would require 12 subjects each to achieve 80% power and 16 subjects for 90% power. For the effect size of 1.0, the respective values are 17 and 23.
This study has several important limitations. First, there was no control group and the baseline level of LDLc ended up being higher in the 6gF group than the other two groups. However, the greatest effect was also observed in the 6gF group, leading to a hypothesis that the effect of clinoptilolite may be dependent on severity of dyslipidemia. Thus, future studies should consider employing a stratified randomization. Second, neither subjects nor investigators were masked, but this bias was minimized by independent laboratory analysis. Physical activity, diet, and safety were not formally monitored; however, the subjects reported no change in lifestyle or health during the study. Finally, the mechanisms by which clinoptilolite may reduce dyslipidemia remain speculative, which warrants further investigations.
Conclusions
Oral administration of clinoptilolite in doses up to 9 g for 8 weeks appears to be efficacious for temporarily improving lipid profile in people with dyslipidemia. These pilot results provide basis for a randomized placebo-controlled trial to examine in more depth the safety profile and, in this study, suggested benefits of clinoptilolite for the treatment of dyslipidemia. Future studies should also address whether adding clinoptilolite to statins is providing an incremental gain over statins alone.
Footnotes
Acknowledgment
The authors thank Dobrivoje S. Stokic, MD, DSc, for assistance and comments on preliminary version of the article.
Author Disclosure Statement
No competing financial interests exist.