
Abstract
Objective:
To explore the impact of the Mindfulness-Based Stress Reduction (MBSR) program on pain severity and endocrine, physical, and psychologic functioning in patients with chronic low-back pain (CLBP).
Methods:
A total of 28 participants were enrolled in the study between January and June 2014; 17 participants were sequentially sampled for an 8-week MBSR program, and 11 were placed on a waitlist control group. Pain severity, quality of life (QOL), global psychologic functioning, and depression were assessed at baseline, at the end of treatment, and 4–5 months post-treatment for both groups. Morning and evening salivary cortisol was assessed at multiple time points in participants in the MBSR group.
Results:
In comparison with baseline, evening cortisol release showed a significant increase post-treatment. Significant differences between groups were found in pain severity. Medium-to-large effect sizes were found for between-group differences in both pain severity and QOL.
Conclusions:
The cortisol increase in the MBSR group is a promising finding, in the context of CLBP hypocortisolism. Data show that the effects of the MBSR treatment may take time to surface. However, due to small sample size, decisive interpretation of findings is limited. Nevertheless, the MBSR program may show promise for CLBP and should be an avenue for further investigation through larger clinical trials within healthcare systems.
Introduction
B
Pain is often the only symptom of the vast majority of spinal disorders. 3,4 As suggested, 5,6 there is no correlation between pathologic findings and back pain symptoms. For this reason, if CLBP is ascribed only to organic causes, 7,8 it has a poor prognosis because of a low rate of resolution even with treatment. 9 Psychologic factors such as anxiety and depression seem to be more predictive of pain and disability with CLBP. 10 These factors can be viewed as expressions of dysfunctional emotional processing in general, and suppression of emotions in particular. 11
Mindfulness-Based Stress Reduction (MBSR) was originally developed in a behavioral medicine setting for patients with chronic pain and stress-related complaints, and pain has been a key topic of research on MBSR from the beginning. 12 –15 Several trials have assessed the effect of MBSR on patients with heterogeneous chronic pain conditions, generally reporting positive results, with significant reductions in pain intensity maintained regardless of the length of assessment period. 16 –19 Despite this encouraging trend, recent reviews specific to CLBP found only inconclusive evidence of the short-term improvements in pain intensity and disability, even if limited evidence that MBSR can improve pain acceptance was acknowledged. 20,21
When studying pain reduction with the use of MBSR, it is important to rely on biomarkers as well as patient-reported outcomes. Cortisol is an accepted stress-related biomarker because anomalous levels of the hormone are found in pathologies associated with stress-related symptoms (anxiety, depression, negative affect), and it is known for long-term damaging effects as a result of chronic stress. 22
It is hypothesized that the hypothalamic–pituitary–adrenal axis (HPAA) may play a predominant role in the association between psychologic variables and chronic pain, including CLBP. 23 In fact, stressful experiences can alter pain thresholds by producing either stress-induced analgesia or hyperalgesia. 24,25 HPAA activity has been found to be attenuated in chronic pain, but elevated in depression and hypercortisolism. Consequently, some authors have argued that hypocortisolism in patients with chronic pain may be due to prolonged periods of stress and excessive glucocorticoid release, which may lead to hyporeactivity of HPAA. 26 –28 However, literature on the relationship between chronic pain and cortisol has yielded conflicting results. 29 The relationship of HPAA with pain is complex, especially, since it has been found to exert a paradoxical effect on pain. The same substances are able to promote analgesia as well as hyperalgesia, depending on the site and mode of application.
Based on these findings, the aim of our study was to explore the impact of the MBSR program on CLBP, as well as on endocrine (cortisol hormone), physical, and psychologic functioning. Our expectation is that the MBSR program may produce an amelioration of the clinical condition of people suffering from CLBP.
Materials and Methods
This study was conducted at the Department of Pain Management of the Hospital Santa Croce & Carle, Cuneo, Italy. The study was approved by the Hospital Ethics Committee and was conducted in accordance with the Declaration of Helsinki and its later amendments. All participants gave their written informed consent before their inclusion in the study.
Participants
Participants were recruited between January and June 2014. Inclusion criteria were as follows: (1) CLBP for at least 3 months; (2) aetiology of the pain had to be: (i) lumbago; (ii) sciatica due to displacement of intervertebral disc, neuralgia, neuritis, radiculitis due to displacement or rupture of the lumbar intervertebral disc; (iii) lumbosacral spondylosis without myelopathy; or (iv) fibromyalgia; (3) age between 20 and 65; and (4) willingness to participate in the study. Exclusion criteria were as follows: (1) non-Italian speaking; (2) currently receiving psychiatric treatment; and (3) the presence of cancer, infections, vertebral collapse due to trauma or osteoporosis, visceral related pain, and rheumatisms.
If a patient met all inclusion criteria for the study, the doctor introduced the study at the end of the physician's office visit as a complementary treatment, and the patient was then referred to the psychologists for further screening.
Of 37 initially identified potential participants, one was a non-Italian speaker, two had scheduling conflicts with the time and date of the course sessions, and six were no longer interested after initial identification, leaving a final sample of 28 (15 women, average age = 48.14, SD = 11.09, median = 47). Of these, 17 were recruited before the beginning of the course and so were selected for the intervention group; the remaining 11 were put onto the control waitlist. Age (p = 0.47), sex (p = 0.48), and education (p = 0.28) of the intervention and control groups were not significantly different (Table 1).
NSAIDs, non-steroidal anti-inflammatory drugs.
At the beginning of the study all patients were undertaking “treatment as usual,” that means a complex array of different analgesic drugs, which were different for each participant (see Table 1 for details). The chronic condition of these people rendered them largely resistant to these treatments. This is the main reason for introducing the MBSR program at the Department of Pain Management. All participants were taking part to a MBSR program for the first time. Furthermore, none had had any previous experience with any kind of meditation and/or yoga practices.
Procedures
After obtaining consent, eligible participants were administered baseline study measures and trained for saliva sampling. The sequential sampling process began in January 2014, and all participants who were referred after March 2014 were put into the control waitlist. The course was organized into 8 weekly sessions of 2 h, included homework assignments, and, during the second-to-last weekend, a 7-h session. All the techniques provided by the program were taught during the course, mainly: the body-scan meditation, sitting and walking meditation, yoga exercises, and relational mindfulness.
In brief, in body-scan meditation, patients were instructed to concentrate their attention on specific parts of their body, to find whatever feelings could be felt from that body part. Once a part was examined this way, attention was moved to another adjacent part, and so on, until the whole body was examined. In sitting meditation, patients were instructed to sit and concentrate their attention on the sensations present in their nostrils as they breathed in and out. This practice was then enriched by increasing the scope of attention to the body, seen as a whole, to the sounds and, finally, to the thoughts that came and left the patient's mind at that time. In walking meditation, patients were asked to pay attention to what their body did as they walked along. In yoga exercises, the patients were directed to extend both their arms and legs and intentionally direct these movements as they exercised gradually. In relational mindfulness practices, the patients were asked to have a brief conversation with one another and direct their heightened awareness to what was happening in the relation space that had just been created.
At the end of each session, the instructor gave reading materials for further study and homework assignments, which usually required the patients to meditate for around 40 min a day with the aid of guided meditation that was recorded and made available on CDs or through web links. After the course was completed, both the intervention and the control group were administered postintervention measurements, with follow-up by telephone at 4–5 months.
For the entire duration of treatment, and during follow-up, both the intervention and control groups underwent “treatment as usual,” including pharmacologic, surgical, and psychologic (cognitive-behavioral) interventions.
Measures
Participants were administered the following measurements at baseline, at completion of the course, and 4–5 months after the end of the course: (1) Cortisol hormone levels were measured in the intervention group only using saliva samples collected using the Salivette® Cortisol test tube (Sarstedt, Numbrecht, Germany, REF 51.1534.500) at 08:00 h and at 23:00 h and analyzed through the electrochemiluminescence immunoassay “ECLIA” Cobas e 411 analyzer (Hitachi-Roche Diagnostics Division USA). (2) Pain severity was measured in both groups through the Numeric Rating Scale (NRS) for pain, a continuous scale from 0 (“no pain at all”) to 100 (“my pain is as bad as it could possibly be”). NRS can be administered verbally, is psychometrically valid and reliable, and preferable to other scales when evaluating pain for research purposes.
30
(3) Quality of life (QOL) was measured in both groups with the SF-36 Health Status Inventory, validated for the Italian population.
31
It reports two summary scores (physical and mental health) and eight individual scores. The physical health summary scale describes the general physical functioning, physical pain, and overall health of a patient; the mental health summary scale describes his or her social and emotional functioning, vitality, and the frequency of experiences related to negative effect, such as anxiety and depression, as well as sensations of psychologic wellbeing. Good internal consistency and reliability of the SF-36 Health Status Inventory for the Italian population have been reported.
31
(4) Depression was measured in both groups through the Beck Depression Inventory (BDI-II), a widely used 21-item multiple-choice self-report inventory of depression symptoms.
32
Higher scores indicate more depression-related symptoms, and cutoff scores are available for differentiating different levels of depression severity. (5) Compliance with the MBSR program and feedback on the general experience of CLBP were measured by semistructured interviews created ad hoc. For what concerns compliance, the questions assessed how many sessions the participant attended and how many minutes of meditation were practiced during the program and a month since its conclusion. It also assessed whether participants reported any difficulties associated with the course and the exercises. For what concerns feedback on the general experience of CLBP, questions asked were the same at baseline and after treatment as follows: (i) How do you describe your lower back pain? (ii) When you feel pain in your back, what are your most common emotions, or thoughts, if any? (iii) How do you live with your lower back pain in your relationship with other people, in the workplace, and in everyday life? (iv) What do you think of the Mindfulness treatment? (v) How would you describe yourself as a person? (vi) How do you see your future in 5–10 years' time? (6) Follow-up by telephone at 4–5 months measured pain severity, QOL, and the duration and quality of the meditation practice.
Statistical analyses
Welch's t tests, and paired t tests were used to compare groups before and after treatment. All variables were tested for normality with the Shapiro–Wilk normality test. Cohen's d was used to calculate the effect size difference between the intervention and control groups. Finally, an intention-to-treat analysis was used for this study, using the Last-Observation-Carried-Forward method. All analyses were computed using the R “Spring Dance” version 3.1.0 program. A p-value of <0.05 was considered to be significant.
Results
Retention and engagement
A total of eight participants completed the meditation program and another five participated in at least four lessons. Four participants dropped out after two or three sessions. All participants—excluding those who dropped after two to three sessions—reported having done a median of 20 min of meditation-related practices per day during the course and a median of 10 min 4–5 months post-treatment. Of the control group, two patients dropped out 4–5 months after the end of treatment.
Dropout rates can be ascribed to the following main factors: (1) all participants in the intervention group were undergoing a period of worsening chronic pain, since they were visiting the Department of Pain Management for pain relief, and the management of such a group was particularly difficult where feelings of anger and sadness were intense; (2) little flexibility was available with the offered course, timewise, and as such scheduling conflicts made participation hard for employed participants, even if notes of attendance were available to present at the workplace; (3) most participants were willing to “try anything” to get rid of their pain, but some could not understand how meditation, a “mental thing,” could produce benefits for pain perceived as a “physical thing.” At some level, therefore, there was prejudice about the practice, which is still new in Italy.
Cortisol levels
Cortisol measurements (Fig. 1) show baseline (T0) and post-treatment (T1) intervention group participant cortisol levels, in μg/dL, at around 08:00 h (morning; M) and 23:00 h (evening; E). One participant was excluded from analysis because of sample timing issues.
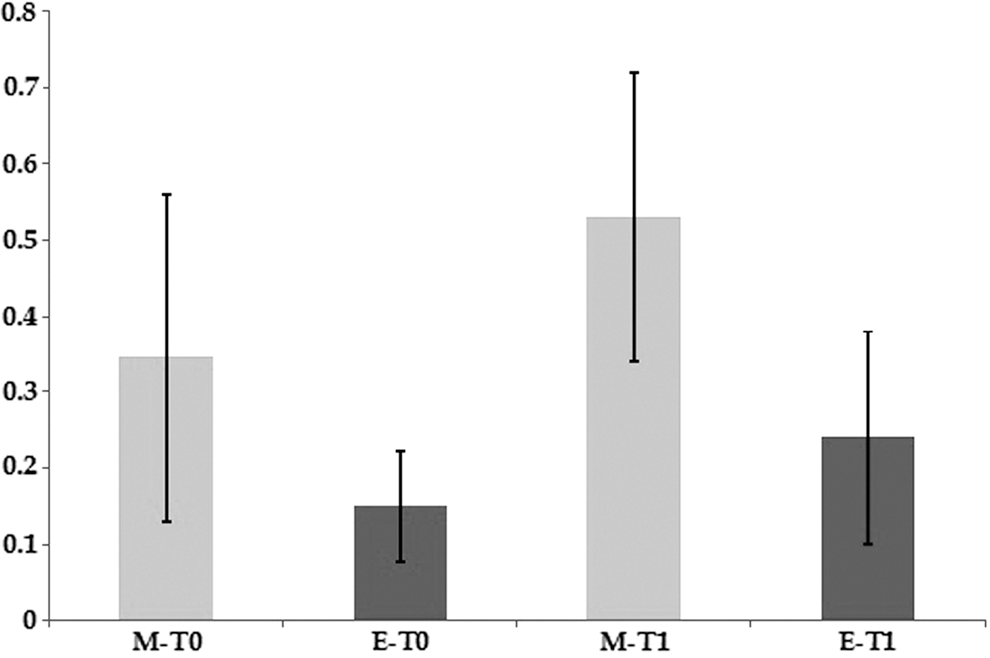
Levels of morning and evening cortisol in μg/dL in the intervention group. Sample size, N = 16. M-T0, baseline morning cortisol; E-T0, baseline evening cortisol; M-T1, after treatment morning cortisol; E-T1, after treatment evening cortisol.
While no significant difference between baseline and after treatment was found in the morning, paired t(15) = 1.84, p = 0.08, a significant difference was observed in the evening cortisol between baseline and post-treatment, paired t(15) = 3.18, p = 0.006. However, no significant correlation was found between cortisol levels and the difference in pain intensity at baseline and after treatment. Cortisol levels obtained in a healthy subject population in Cuneo hospital at 08:00 and 23:00 h, average <0.9 μg/dL and <0.3 μg/dL, respectively (per the Cuneo Hospital Endocrine Department records). These data seem to suggest that no abnormalities, such as hypercortisolism, can be observed in the patients studied.
In the MBSR group, post-treatment evening cortisol demonstrated an increase from baseline, although levels remained within the range of normal levels reported in the Cuneo population. However, all other cortisol measurements (at both baseline and during treatment) were lower in the MBSR group than that in the Cuneo general population, M-T0: t(15) = 8.86, p < 0.0001; E-T0: t(15) = 6.09, p < 0.0001; M-T1: t(15) = 7.7, p < 0.0001.
Pain severity
Figure 2 shows NRS medians at baseline (T0), after treatment (T1), and at 4–5 months after treatment (T2) for both the intervention and control groups. A significant difference was observed between the intervention and control distributions, Welch two-sample t(22) = 2.69, p = 0.01. The observed effect size was large (Cohen's d = 1.03) at T2.
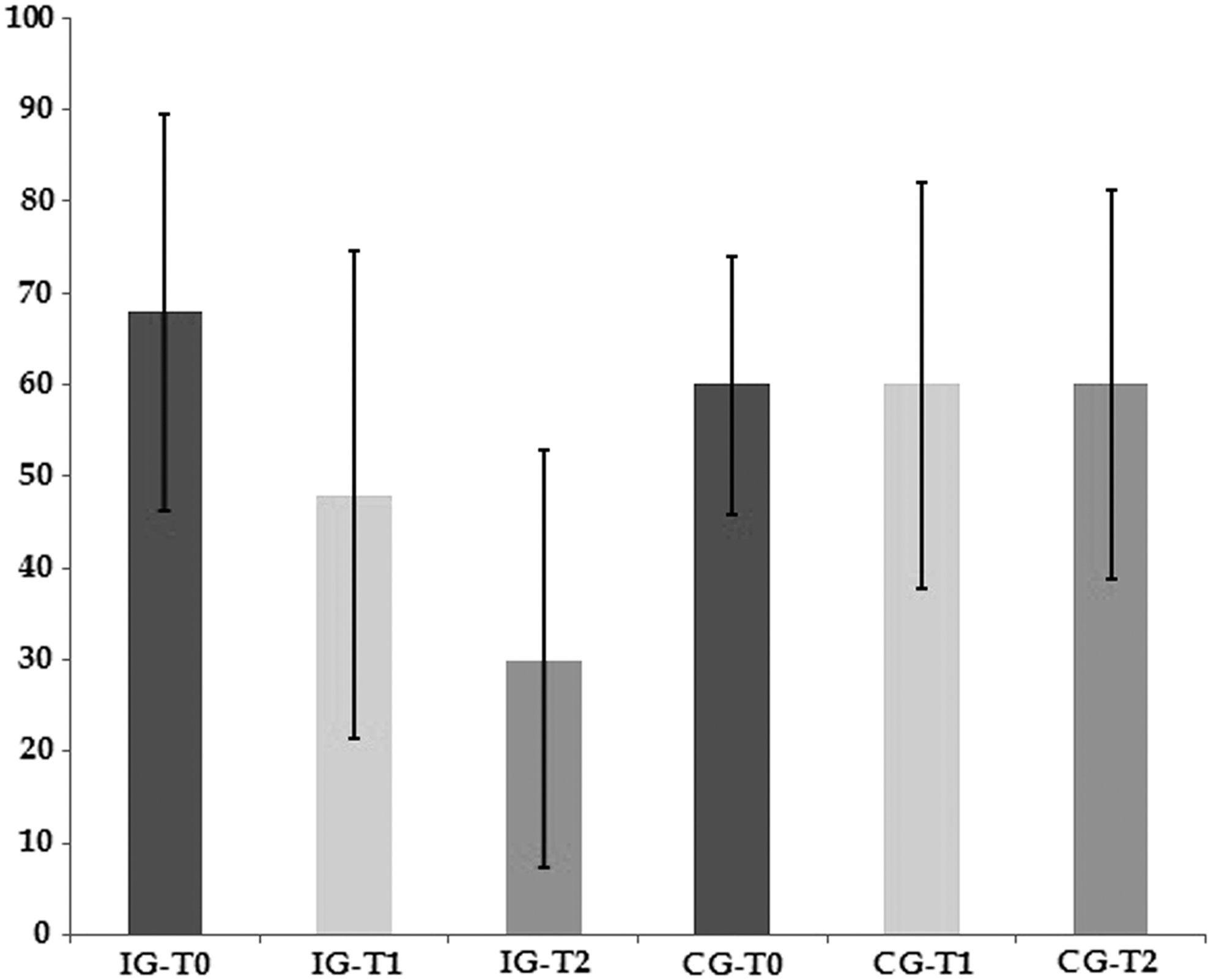
Pain measured by the NRS for pain. Lower scores indicate lesser pain severity. Sample size, n = 11 for the control group and n = 17 for the intervention group. IG-T0, intervention group baseline pain; IG-T1, intervention group after treatment pain; IG-T2, intervention group 4–5 months after treatment pain; CG-T0, control group baseline pain; CG-T1, control group after treatment pain; CG-T2, control group 4–5 months after treatment pain; NRS, Numeric Rating Scale.
Quality of life
Summary scale results of the SF-36 Health Status Inventory are presented in Figures 3 and 4. The bar charts present the medians of the summary scales provided in the SF-36 Health Status Inventory for both physical and mental well-being.
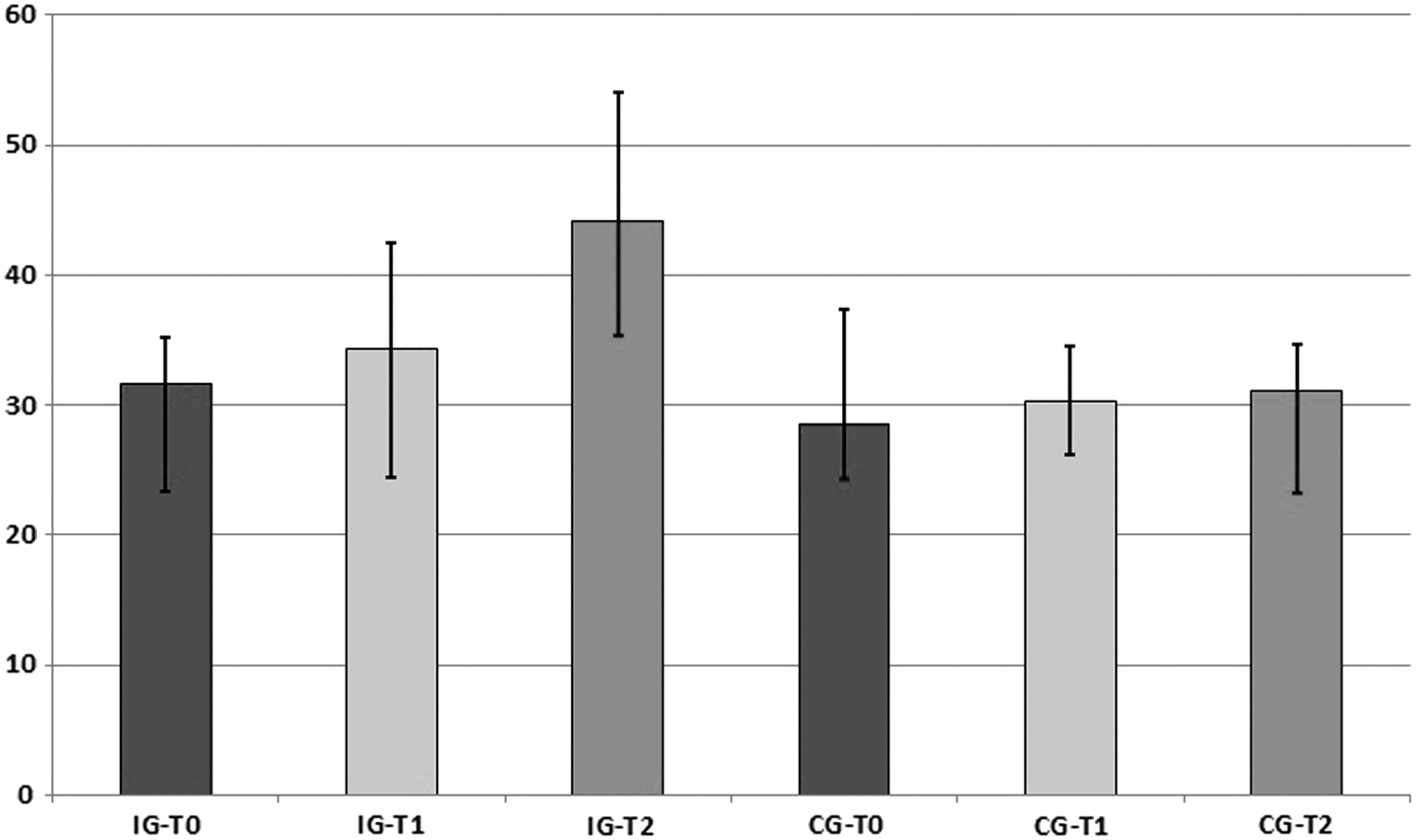
Physical Health Summary Scale bar chart. Sample size, n = 11 for the control group and n = 17 for the intervention group. IG-T0, intervention group baseline; IG-T1, intervention group after treatment; IG-T2, intervention group 4–5 months after treatment; CG-T0, control group baseline; CG-T1, control group after treatment; CG-T2, control group 4–5 months after treatment.
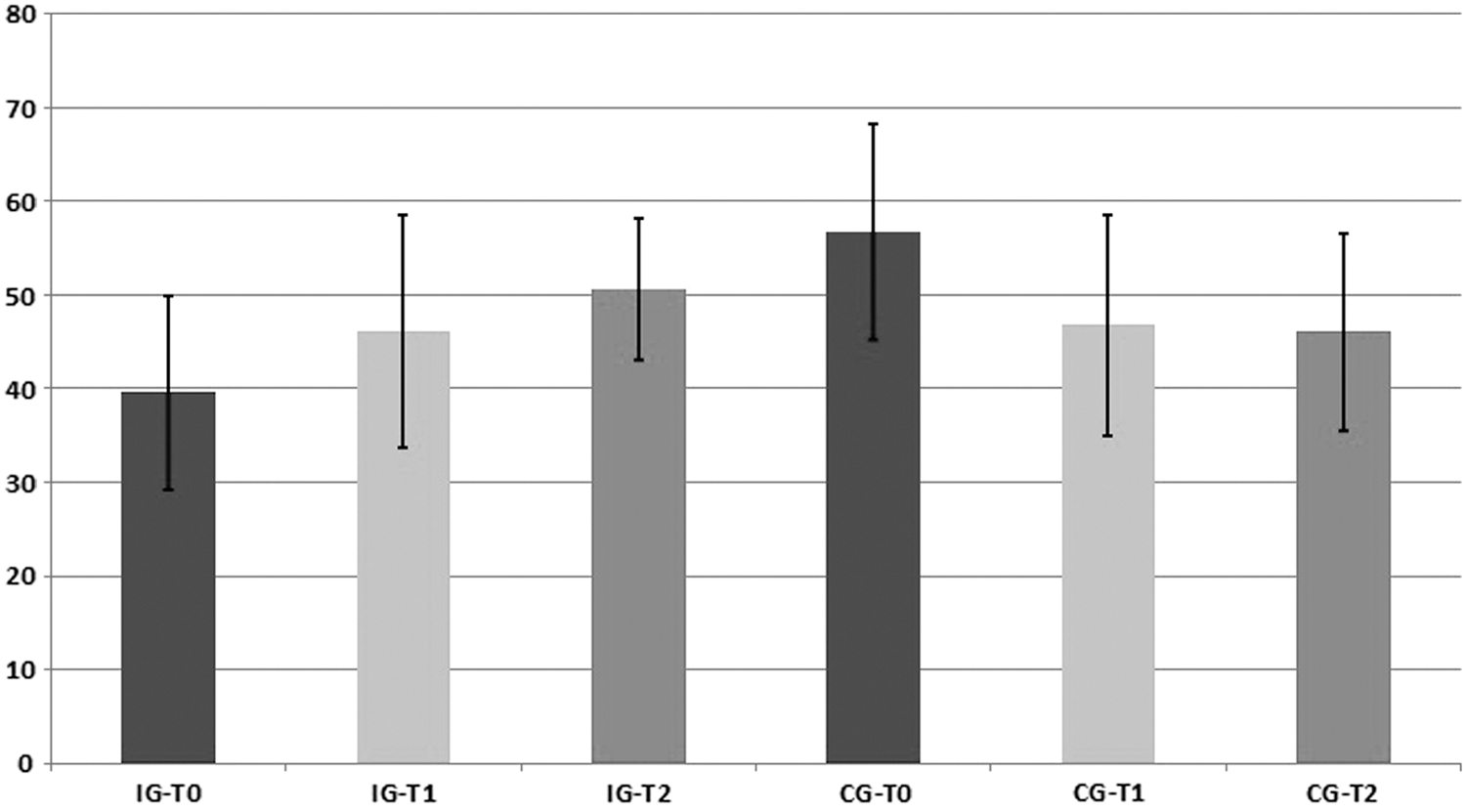
Mental Health Summary Scale bar chart. Sample size, n = 11 for the control group and n = 17 for the intervention group. IG-T0, intervention group baseline; IG-T1, intervention group after treatment; IG-T2, intervention group 4–5 months after treatment; CG-T0, control group baseline; CG-T1, control group after treatment; CG-T2, control group 4–5 months after treatment.
A significant difference was observed between intervention group T0 and T2 scores on both scales, Physical Health Summary scale paired t(16) = 3.71, p < 0.001, and Mental Health Summary scale paired t(16) = 3.75, p < 0.001. Comparisons between the intervention and control groups' scores indicated that these patients, despite an observed increase from baseline, report a level of QOL well below the average for the Italian population of 53.3 for the Physical scale, t(16) = 5.36, p < 0.001, while no significant difference was found for the Mental scale between the general population average of 49.3 and participant scores, t(16) = 0.9, p = 0.37. No baseline difference was found between the intervention and control groups on the Physical scale, t(25.1) = 1.4, p = 0.15, nor on the Mental scale, t(19.5) = 1.8, p = 0.7.
Depression
No significant difference was observed in depression between the intervention (average = 8.41, median = 9, SD = 5.91) and control (average = 6.82, median = 4, SD = 6.16) groups, Welch's two-sample t(20.8) = 0.67, p = 0.5. The effect size was negligible (d = 0.26).
Semistructured interviews
Semistructured interview recording sessions lasted an average of 13.87 min (SD = 4.92) per participant at baseline and post-treatment, for a total of 720 min of interviews across all participants.
Approximately 72% of participants judged the program positively, with a minority (23%) reporting that they would attend the course again, given the chance. Nearly 17% had mixed feelings or had no opinion to offer, while the remainder (11%) was critical and found it a negative experience. Approximately 71% reported continuing to practice 4–5 months following the end of the program; of these, 33% said that they used the body scan most often, another 33% the formal sitting meditation, 25% the walking meditation, and the last 9% used a mix of mindful eating and simple present moment concentration in a variety of situations. Regarding the meditation practice, 41% said that they found it relaxing, 23% reported less pain, and 17% said that it increased their wellbeing.
Discussion
In the present study of MBSR in patients with CLBP, both an evening cortisol increase and a reported amelioration of chronic pain were observed post-treatment.
Lower cortisol levels have been found in chronic pain patients as well as in some stress-related disorders, such as fatigue syndrome, chronic pelvic pain, and fibromyalgia. 23,33 –38 Hypocortisolism in patients with chronic pain may be due to prolonged periods of stress and excessive glucocorticoid release, leading to hyporeactivity of the HPAA; therefore, this process is believed to be causally involved in pain chronicity. 26 –28 Although this finding was expected, the literature on chronic pain and basal stress hormones has yielded conflicting results, 29,39,40 and complex confounding factors in salivary cortisol sampling may diminish explanatory power. 41 Moreover, steroid drugs taken during the sampling period may account for some of the results obtained. 23
Other confounding factors, such as depression, may explain the increase in basal cortisol levels 29 ; however, no significant differences in depression were observed at either baseline or post-treatment. In addition, it is important to note that due to small sample size, these results cannot be generalized. Consequently, the authors conclude that, barring the above-mentioned cautions, these data suggest convergence of the intervention group toward more normative levels of glucocorticoid release. Since comparison with the control group is not possible, the authors cannot determine to what degree the MBSR treatment impacted the results observed. This is a limit of the study and in the future it should be clarified.
With regard to the chronic pain levels of the MBSR group, the results of this study seem to indicate an amelioration of the clinical condition, measured both directly through assessment of pain levels and indirectly through the increased bodily functionality reflected by the QOL scales. Observed effect sizes were medium to large for the intervention group compared with the control group, but the low rate of completion of the program and the dropout rate of the control group make these and other results difficult to interpret; therefore, it is not possible to draw definitive conclusions from the data presented herein. Anecdotally, some participants' semistructured interview statements seem particularly revealing of this state of affairs, in particular, regarding pain:
Said a participant, “I had greater expectations about the pain relief the meditation would bring. The pain is acute, it is strong, but now I feel less afraid of it. It is as if it was free no more, as if it was contained into something, like a gelatin container.”
Another participant said, “I can do today less than I used to do before, but now it is a little better; I can coexist with this pain with more awareness, I allow myself to do what I can.”
From these interviews, the decoupling of the emotional and sensory components of pain can be seen at work. Other studies are consistent with these findings. 21,39,42 –46 Meditation, of which MBSR provides an introduction, takes time to produce effects. 21,47,48 In fact, the authors observed that the effect sizes at the end of treatment were small, while there was a larger increase at 4–5 months follow-up.
It is worth noting that, rather than addressing pain as an issue to be confronted and resolved head-on, 49 the approach of Mindfulness is directed toward the acceptance of one's entire present experience, which includes, among other things, unwanted experiences, including pain, unpleasant emotions, and thoughts. In this way, the aim is not to reduce pain, but the patient's response to it. However, it is also interesting to note that most participants stated that meditation was useful just for relaxation, pain reduction, and wellbeing purposes, while it is recognized that meditation's primary objective is to build awareness of one's life in the present, moment by moment, as well as acceptance, while relaxation and other benefits are viewed as collateral effects other than the final goal of the technique. 50
Furthermore, it is worth noting that since yoga has been reported to ameliorate both dysfunction and disability in CLBP patients, it may have a crucial effect on pain reduction within the MBSR program, since the only randomized control trial that has reported favorable effects of MBSR on functional disability also included yoga. 51 Further research, as Cramer et al. 21 noted, should include dismantling studies that separately evaluate the effects of different components of MBSR such as mindful meditation and yoga.
The results observed can be explained in terms of the placebo effect. It is well known that the placebo response can affect mood, endocrine functions, and pain perception among other things. 52 Ethical standards require that patients receive the best treatment available; therefore, it was not possible to withhold treatment in the control group which underwent “treatment as usual,” which, in turn, was difficult to standardize. In addition, patient-reported outcomes, patient's expectations about the benefits of the treatment, and the quality of the relationship with the MBSR instructor, may account for increased placebo responses, with implications for both the endocrine and psychologic outcomes.
On the contrary, a placebo response should also be observed in the control group if this were the case, which was undergoing standard pharmacologic treatment, invasive surgical techniques, and psychoeducational (cognitive-behavioral) support during the same period of the intervention group. Moreover, it should be noted that no significant group differences in pain perception and only small-to-medium effect sizes were observed immediately post-treatment. It could be argued that the placebo effect should have been observed directly after the end of the treatment rather than 4–5 months later. That said, it is hard to discern what effects may be ascribed to effective treatment(s), placebo, or their interaction at this stage. Therefore, the aim of future studies should be to minimize the placebo response or optimize treatment-placebo differences.
Conclusion
The use of the MBSR program for adults with CLBP revealed medium-to-large improvements in the intervention group compared with the control group at 4–5 months post-treatment on measures of pain severity and physical and psychologic functioning. Increases in evening cortisol release after treatment, although within normative levels, may be a positive sign, given that hypocortisolism has been found in many studies with CLBP subjects. Furthermore, data seem to suggest that the treatment exerts greater effects over time. Although this study has some limitations and the results cannot be generalized, the use of the MBSR program for CLBP shows promise and could present an avenue for further investigation with larger clinical trials within the context of healthcare systems.
Footnotes
Acknowledgments
The authors gratefully acknowledge for their assistance and support with this study Federico Boem, PhD Philosopher of Science; Fabrizio Dini, PhD and Lapo Farnesi Engineers, Consultants for Statistical and Data Analysis; Ludovica Mazzei, PhD Psychologist and Practicing Therapist; and all of the other Cuneo Hospital Santa Croce & Carle Pain Management Department. R.B.A. was supported by the University of Turin (Ricerca scientifica finanziata dall'Università “Cognizione sociale e attaccamento in popolazioni cliniche e non cliniche”).
Author Disclosure Statement
No competing financial interests exist.