
Abstract
Objectives:
This study's aims are to examine the effects of aromatherapy massage on women's stress and immune function during pregnancy.
Methods:
This longitudinal, prospective, randomized controlled trial recruited 52 healthy pregnant women from a prenatal clinic in Taipei using convenience sampling. The participants were randomly assigned to the intervention (n = 24) or control (n = 28) group using Clinstat block randomization. The intervention group received 70 min of aromatherapy massage with 2% lavender essential oil every other week (10 times in total) for 20 weeks; the control group received only routine prenatal care. In both groups, participants' salivary cortisol and immunoglobulin A (IgA) levels were collected before and after the intervention group received aromatherapy massage (every month from 16 to 36 weeks gestation) and were analyzed using enzyme-linked immunosorbent assay.
Results:
The pregnant women in the intervention group had lower salivary cortisol (p < 0.001) and higher IgA (p < 0.001) levels immediately after aromatherapy massage than those in the control group, which did not receive massage treatment. Comparing the long-term effects of aromatherapy massage on salivary IgA levels between groups at different times, the study found that the pretest salivary IgA levels at 32 (p = 0.002) and 36 (p < 0.001) weeks gestational age (GA) were significantly higher than the pretest IgA at 16 weeks GA (baseline).
Conclusions:
This study presented evidence that aromatherapy massage could significantly decrease stress and enhance immune function in pregnant women. The findings can guide clinicians or midwives in providing aromatherapy massage to women throughout the pregnancy.
Introduction
P
The gradually increasing stress during pregnancy can threaten women's health and lead to adverse perinatal outcomes, 10 such as perinatal depression, 2,22,23 pregnancy-induced hypertension, preeclampsia, 24 and an increased risk of preterm delivery and low infant birth weight. 25,26 To improve maternal, fetal, infant, and child health, complementary medicine has received particular attention as a modern method of caring for women during the prenatal, perinatal, and postnatal periods. 27 The comfort interventions that are commonly used and acceptable for the public include the use of aromatherapy and massage to release stress and alleviate physical and psychological discomfort. 28 –31 There are various strategies for the use of essential oil, and stress relief and comfort effects can be generated by massaging natural essential oils into the skin, adding them to bath water, or inhaling the aromas of oils added to a steam infusion or burner. 31 –33
Massage therapy has been shown to have beneficial effects on prenatal depression. 34 The mechanism of the massage therapy involves the stimulation of pressure receptors, which leads to enhanced vagal activity and reduced cortisol levels. 35 –37 Aromatherapy massage is becoming increasingly popular and has been validated as beneficial to the immune function 38 for the general population and for cancer patients. 39,40 Some researchers have also reported that aromatherapy massage using essential oils can reduce body tension and emotional stress. 36 Because of the significant effects of aromatherapy massage on the general populations, clinicians incorporated complementary medicine interventions into perinatal care for women during labor or postpartum. 41,42 Imura et al. used aromatherapy massage to improve postpartum women's physical and mental status and to facilitate mother–infant interactions. 42 A previous study reports that aromatherapy massage significantly reduced pain perception during labor in primiparous women. 41 However, no studies have examined the use of aromatherapy massage to relieve stress and enhance immune functions in pregnant women. To fill this knowledge gap, this study designed a longitudinal study to examine the effects of modified aromatherapy massage on women's stress and immune function throughout pregnancy. Specifically, this study measured levels of salivary cortisol and IgA from 16 to 36 weeks of pregnancy. Based on the mechanisms of aromatherapy and massage, and the above-mentioned research evidence, this study hypothesized that pregnant women receiving aromatherapy massage using lavender essential oil would have lower salivary cortisol and higher salivary IgA levels than those who received only routine prenatal care.
Materials and Methods
Study design
For this prospective, randomized controlled trial with a longitudinal, repeated-measure design, pregnant female participants were randomly assigned by a blinded statistician using Clinstat block randomization
43
into either the control group or the aromatherapy massage intervention group. The pregnant women in the control group received only routine prenatal care, while the pregnant women in the intervention group received routine prenatal care plus the aromatherapy massage intervention from 16 to 36 weeks gestational age (GA). This study was conducted according to the CONSORT guidelines (Supplementary Fig. S1; Supplementary Data are available online at
Participants and setting
Pregnant women at ∼16 weeks GA were recruited by convenience sampling from February 2014 through January 2015 from the prenatal clinic of a medical center in Taipei, Taiwan. Women were included if they met the following criteria: (1) normal pregnancy, (2) age 20–45 years, (3) agreed to follow-up collections of saliva samples, and (4) could read and write Chinese. Women were excluded based on the following criteria: (1) oral steroid use, (2) history of severe illness (e.g., heart disease, systemic lupus erythematosus, and metabolic disorders) or depression, (3) drug use (prescribed or illicit), and (4) high-risk pregnancy (i.e., first-trimester vaginal bleeding, artificial insemination, multiple gestations, fetal growth restriction, or other abnormalities). Of the 93 pregnant women who were screened, 62 met the study criteria (Fig. 1). A total of 52 pregnant women aged 24–43 years were included in this study and randomly assigned to either the aromatherapy massage intervention group (n = 24) or control group (n = 28). The study's power was estimated using G* POWER version 3.1.2. 45 Based on the between-group and within-group variances, the effect size was 0.498, and the total sample size (52) and a significance level of 0.05 led to a study power = 0.95.
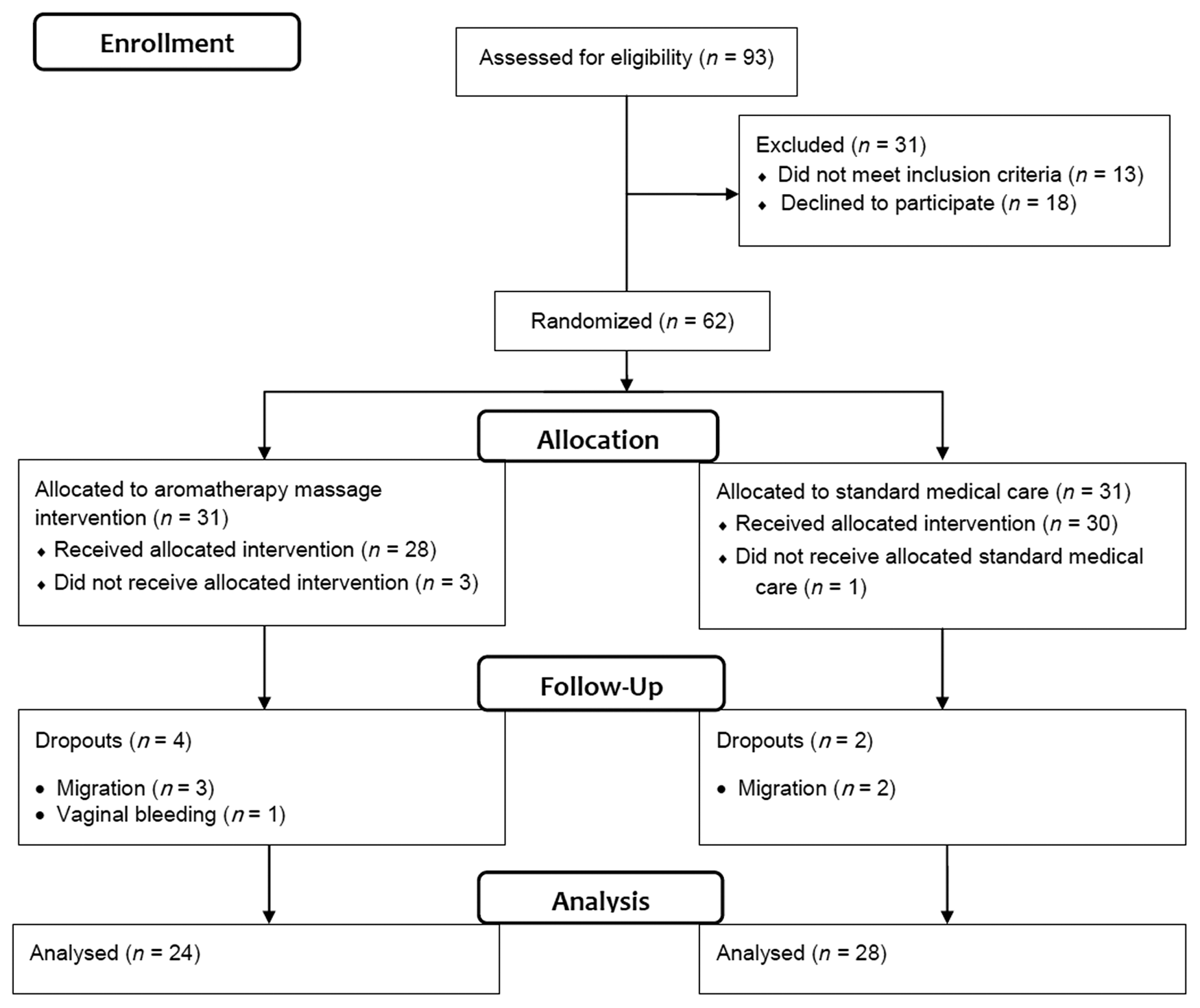
Study design and participant flowchart.
Aromatherapy massage intervention
All participants in the intervention group underwent 70 min of one aromatherapy massage every other week between 16 and 36 weeks GA (10 times in total). The interventions were conducted by a certified aromatherapy therapist for pregnant women according to the following protocol: the aromatic massage oils were composed of 2 c.c. lavender (Lavandula angustifolia) blended with 98 c.c. almond oil. This concentration of the mixed essential oil was kept at room temperature for massage use. The aroma of the lavender oil was either inhaled by the women or absorbed into their skin. 41,46 All participants in the intervention group consistently received the aromatherapy massage by applying effleurage, friction, petrissage, and vibration to the body parts. The therapist consistently massaged the body parts, including the head, neck, shoulder, arms, waist, back, legs, and feet with 2% lavender essential oil, using moderate pressure that the pregnant women could tolerate.
The aromatherapy massage took place in a quiet room with the temperature maintained at 25°C–26°C and the humidity at 50%–60%. The participants wore a comfortable gown and lay down on a massage bed for 10 min, after which their saliva was collected using cotton swabs for preintervention outcome data measurement. Then, the aromatherapy massage was performed according to the protocol. The aromatic essential oils were used to massage the back, posterior legs, anterior legs, arms, and shoulders. The total amount of essential oils needed for the massage was ∼30 mL, and the duration of the massage was ∼1 h. Ten minutes after the aromatherapy massage, another saliva sample was collected for postintervention outcome data measurement. Finally, this study provided 200 mL warm water to the participants to drink. To consider circadian variations in salivary cortisol and IgA, 47,48 the aromatherapy massage sessions were scheduled between 15:00 and 17:00 in the afternoon.
Saliva collection
Saliva samples were collected from the participants from 16 to 36 weeks GA under the guidance of the first author between 14:50 and 17:10 on the day the aromatherapy massage took place. The participants were advised verbally and in writing (1) to avoid alcohol for 24 h, (2) to avoid eating and drinking caffeinated products within 2 h before saliva collection, 49 (3) to refrain from brushing their teeth before saliva collection, and (4) to avoid saliva collection if their gums were bleeding. To collect a sufficient quantity of saliva, this study used cotton swabs (Salimetrics, State College, PA), which were stored in double-layer plastic tubes with a lid. When participants chew a swab for ∼2 to 3 min, a sufficient amount of saliva is stimulated for collection (1 mL). After the tube was centrifuged at 1000 g for 2 min, the saliva was stored at −80°C until it was assayed.
Outcome measures
Stress measures
This study used salivary cortisol as the indicator of stress. To assess stress in this study, the concentrations of cortisol (μg/dL) in saliva samples were analyzed by the first author, who had 2 years of training in medical scientific laboratories. Cortisol was measured using a competitive enzyme-linked immunosorbent assay (ELISA) kit (Cayman Chemical, Ann Arbor, MI).
Immune function measures
This study used salivary IgA as the indicator of immune function. To assess immune function in this study, the concentrations of IgA (μg/mL) in saliva samples were analyzed and measured using the double-antibody sandwich ELISA method according to the manufacturer's instructions (ICL, Inc.).
Procedures
This study was approved by the institutional review board (IRB) of the Tri-Service General Hospital (IRB No. 2-102-05-148) and it was registered at ClinicalTrials.gov (NCT03002337). Written consent was obtained from the women who agreed to participate in the study. The pregnant women who met the study criteria received a pamphlet introducing the study when they first came to the prenatal clinic. Interested women returned the response sheet to a research assistant whose name was printed on the sheet; the assistant then explained the study's objectives and methods and obtained the women's consent. The first author and a research assistant who had worked in obstetric units for ∼2 years were trained by the principal investigator to provide routine prenatal care to all the participants. For the participants in the intervention group, saliva samples were collected by the research nurse 10 min before and immediately after the aromatherapy massage. The participants in the intervention group completed 10 aromatherapy massage sessions from the same aromatherapist over 20 weeks of pregnancy. Each participant lay in supine position on a comfortable soft bed in a quiet room during the massage.
For the participants in the control group, saliva samples were collected by the research nurse at the same times they were collected from the participants in the intervention group. The research nurse stayed in a room next to the prenatal clinic where she provided the routine prenatal care to the participants. A total of 12 saliva samples from each group were collected from 16 to 36 weeks GA. Data from the first saliva samples were used as baseline data. Salivary cortisol and IgA were consistently collected and measured by the first author as outlined above.
Statistical analysis
The data were analyzed using SPSS Version 20.0. All the participants' demographic and clinical characteristics were compared using Mann–Whitney U test for continuous values and Fisher's exact test for categorical values. To evaluate the immediate and long-term effects of aromatherapy massage, this study used the generalized estimating equation method's generalized linear models with three-way interaction (group × weeks × post) to compare salivary cortisol and IgA levels between the intervention and control groups (group). 50 Statistical significance was defined as p < 0.05.
Results
Participant characteristics
Fifty-two pregnant women (24 in the intervention group and 28 in the control group) did not differ significantly in terms of gravida, para, education level, employment status, annual household income, or mean chronological age, which was 33.31 ± 4.01 years (range = 24–43; Table 1). The participants who completed and dropped out of the study did not differ significantly in any of the demographic characteristics measured. All the participants had singleton pregnancies.
p, Statistical significance was defined as p < 0.05.
Fisher's exact test.
Mann–Whitney U test.
NTD, New Taiwan dollars (33 NTD = U.S. $1); SD, standard deviation.
Effects of aromatherapy massage on stress
At pretest (GA = 16 weeks), the salivary cortisol levels for the intervention and control groups were not significantly different (p = 0.295). In the control group, the pretest–post-test difference (immediate effect) in salivary cortisol levels at 16 weeks GA was not significant. Comparing the time effects of the pretest salivary cortisol levels for the control group, this study found that the pretest salivary cortisol level at 36 weeks GA was significantly higher than at 16 weeks GA (p < 0.001) (Table 2 and Fig. 2).
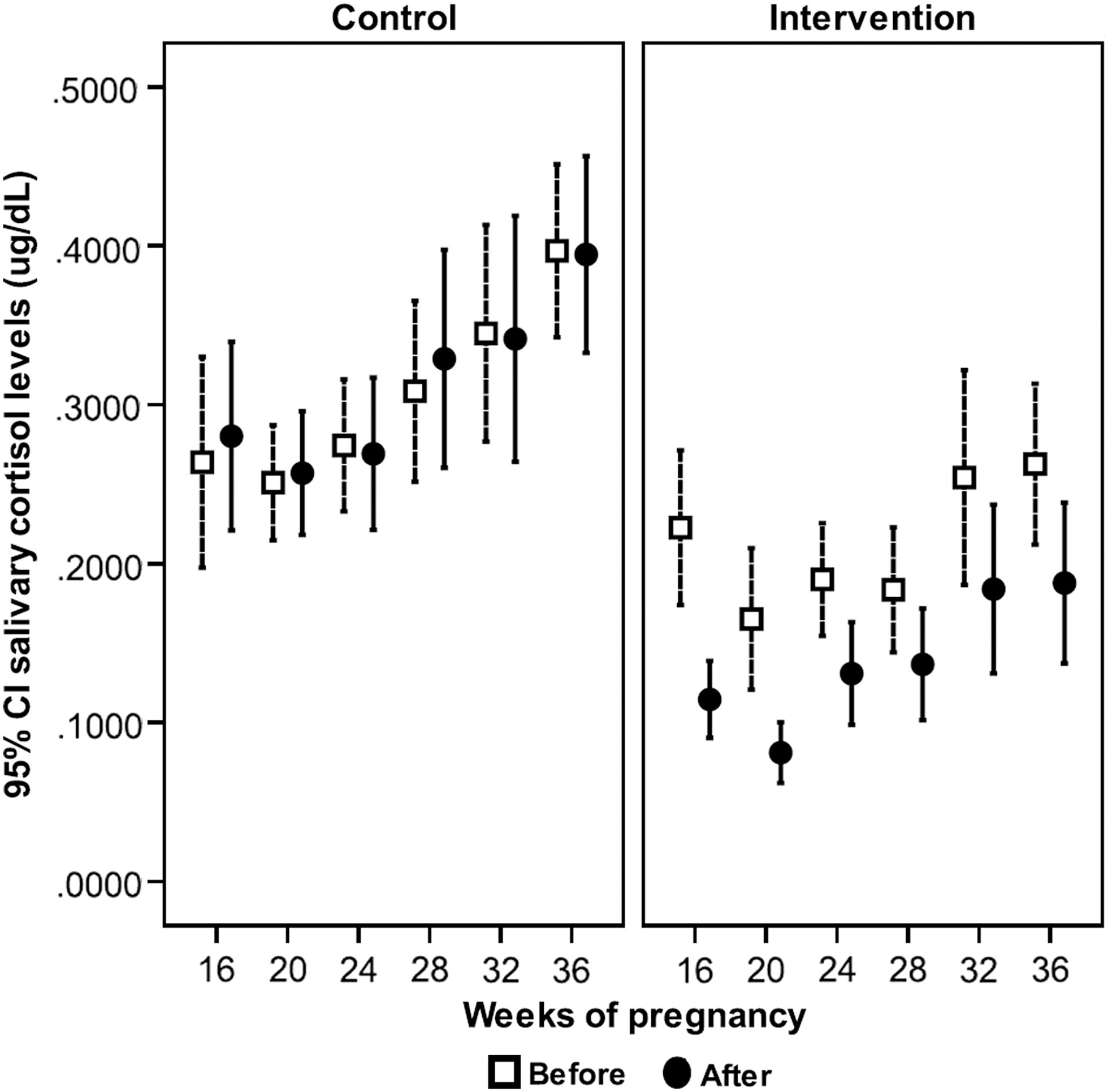
Overall differences between the intervention and control groups in salivary cortisol (μg/dL) levels. Changes in salivary cortisol levels at six time points (16, 20, 24, 28, 32, and 36 weeks GA) during pregnancy for women receiving aromatherapy massage (intervention group) or routine prenatal care (control group). 95% CI, 95% confidence interval; GA, gestational age.
p, Statistical significance was defined as p < 0.05.
Group: 1, intervention group; 0, control group.
Post: post-test minus pretest; 1, post-test; 0, pretest.
The reference category was baseline or 16 weeks of gestation.
B, coefficient; CI, confidence interval; SEM, standard error of the mean.
In comparison, the pretest–post-test difference at 16 weeks GA shows an immediate and significant effect of aromatherapy massage on salivary cortisol levels between the two groups (p < 0.001). In the control group, the post-test salivary cortisol levels were similar to the pretest salivary cortisol levels at each time point. The immediate effects were not significantly different from the immediate effect at 16 weeks GA except at 24 (p = 0.035) and 36 (p = 0.049) weeks GA because the post-test salivary cortisol levels were lower than the pretest levels at 24 and 36 weeks GA. In the intervention group, the post-test salivary cortisol levels markedly decreased after aromatherapy massage and persisted at 20, 24, 28, 32, and 36 weeks GA in the same manner as the immediate effect at 16 weeks GA (Fig. 2). Therefore, the immediate effects of the salivary cortisol levels at 20, 24, 28, 32, and 36 weeks GA were not significantly different from the immediate effects at 16 weeks GA in the intervention group (Table 2 and Fig. 2).
Effects of aromatherapy massage on immune function
At baseline (GA = 16 weeks), salivary IgA levels did not differ significantly between the intervention and control groups. In the control group, the pretest–post-test difference in salivary IgA levels at 16 weeks GA was not significant. Comparing the time effects of the pretest salivary IgA levels in the control groups, this study found that the pretest salivary IgA level at 24 weeks GA was significantly higher than at 16 weeks GA (p = 0.005). Comparing the time (or long term) effects of aromatherapy massage on salivary IgA levels between the intervention and control groups at different times, the study found that the pretest salivary IgA levels at 32 (p = 0.002) and 36 (p < 0.001) weeks GA were significantly higher than the pretest IgA at 16 weeks GA (baseline) (Table 3 and Fig. 3).

Overall differences between the intervention and control groups in salivary IgA (μg/mL) levels. Changes in salivary IgA levels at six time points (16, 20, 24, 28, 32, and 36 weeks GA) during pregnancy for women receiving aromatherapy massage (intervention group) or routine prenatal care (control group). IgA, immunoglobulin A.
p, Statistical significance was defined as p < 0.05.
Group: 1, intervention group; 0, control group.
Post, post-test minus pretest: 1, post-test; 0, pretest.
The reference category was baseline or 16 weeks of gestation.
In comparison, in the intervention group, the pretest–post-test difference at 16 weeks GA showed an immediate effect of aromatherapy massage on salivary IgA levels (p < 0.001). In the control group, the post-test salivary IgA levels were similar to the pretest salivary IgA levels at each time point. The immediate effects were not significantly different from the immediate effect at 16 weeks GA; the exception was at 32 (p = 0.026) weeks GA, when the post-test salivary IgA levels were lower than the pretest levels. In the intervention group, the post-test salivary IgA levels markedly increased after aromatherapy massage and persisted at 20, 24, 28, 32, and 36 weeks GA in the same manner as the immediate effect at 16 weeks GA (Fig. 3). Therefore, the immediate effects on salivary IgA levels at 20, 24, 28, 32, and 36 weeks GA did not significantly differ from the immediate effects at 16 weeks GA (Table 3 and Fig. 3).
Discussion
In this study, the effects of aromatherapy massage with 2% lavender essential oil in pregnant women showed significant immediate effects on stress (salivary cortisol levels) and significant immediate and long-term effects on immune function (salivary IgA levels) throughout pregnancy. This study contributes knowledge to the literature by using a longitudinal repeated-measures design to monitor changes in healthy pregnant women's salivary cortisol and IgA levels after aromatherapy massage between 16 and 36 weeks GA. In addition, the aromatherapy massage showed significant long-term effects on salivary IgA levels at 32 and 36 weeks GA compared with the immediate effects on the IgA levels at 16 weeks GA in the intervention group. However, the long-term effects of aromatherapy massage on pregnant women's stress (salivary cortisol levels) did not significantly decrease. The finding can be explained by the fact that pregnant women's stress increases as the pregnancy progresses, and this is the normal physiological response to pregnancy. In the control group, the salivary cortisol levels significantly increased at 36 weeks GA. Although the effects of aromatherapy massage might buffer and alleviate pregnant women's stress, the dosages of the aromatherapy massage that the authors provided to these pregnant women were still not enough to overcome the stress caused by pregnancy especially at 36 weeks GA. These findings also suggest that the dosages of aromatherapy massage provided to the pregnant women needed to increase after 32 weeks GA. This study did not explore the frequency of aromatherapy massage pregnant women need. However, it can infer that the dosages need to be adjusted according to the pregnant woman's stress levels at different points in their pregnancy, and they may need to receive aromatherapy massage once a week or twice a week. These results suggest that aromatherapy massage significantly benefited women by immediately reducing their stress and strengthening their long-term immunity, supporting the hypothesis that regularly receiving aromatherapy massage mitigates pregnant women's stress and enhances their immunity.
The study findings are also consistent with the findings from several previous studies that explored the effects of aromatherapy massage 36,38 or aroma inhalation therapy 51,52 on stress (cortisol levels decreased) in nonpregnant women. Furthermore, Field reported that massage only could significantly reduce stress in adults, infants, and pregnant women by increasing parasympathetic activity and improving the functioning of the HPA system. 35 However, Takeda et al. reported that there were no significant differences in the salivary cortisol and IgA levels of a group that underwent a single session of massage or aromatherapy massage compared with a rest group. 53 The reasons for their contradictory finding might be that their study only provided a single session of massage or aromatherapy massage and their sample included only 13 participants. 53 However, findings regarding the effects of aromatherapy massage are still inconsistent. Further studies are needed to explore the effectiveness of aromatherapy massage and determine how many dosages of the therapy different populations need to effectively relieve their stress.
Regarding the effect on salivary IgA levels, the study findings suggest that aromatherapy massage could significantly enhance pregnant women's immunity, regardless of whether the effects are immediate or long lasting. Takeda et al. conducted a cross-over study and found that salivary IgA levels increased immediately after rest, massage, and aromatherapy massage in healthy adults. All three of these interventions showed increases in salivary IgA levels. 53 However, this study did not discuss the interval between the interventions or consider the carryover effects of each intervention. Another study compared the effects of massage with a carrier oil and massage with essential oils on the salivary IgA levels of healthy adults and reported that there was no significant difference in the salivary IgA levels between the two groups. 38 However, there was no control group in that study, the sample only included 11 adults, and the participants only received one session of massage. The study results could not show the immediate or long-lasting effects of the two interventions. 38
Moreover, some studies have reported that aromatherapy inhalation with essential oils could significantly decrease heart rates and improve anxiety and anger for pregnant women. 46 Field et al. provided massage therapy twice a week to pregnant women from 12 to 32 weeks GA and found that it could significantly reduce their anxiety and depression during pregnancy. 34 While it is clear that there is a growing body of evidence regarding the practice of aromatherapy massage, there is little empirical data to guide clinical practice for maternity care. Although these two studies did not measure the biological outcomes, their findings guided the authors in developing this study and designing the intervention for pregnant women.
The unique aspect of this study is that it longitudinally followed women throughout their pregnancy to determine the effects of aromatherapy massage on the women's immune function. The evidence established by this study could guide clinicians in helping women alleviate their stress and enhance their immune function and health during pregnancy. The benefits of this study are particularly important for women during pregnancy. Pregnancy and motherhood are a unique responsibility for women; however, pregnancy and the changes it brings cause stress and discomforts that might impede women's responses to the challenges of being pregnant, especially in the current competitive society. Therefore, it is essential to help pregnant women manage their stress and promote their health. 54 Clinicians play pivotal roles in identifying and relieving women's stress in obstetric practice. The optimal strategies for pregnant women involve natural, harmless, and safe interventions, such as complementary therapies. Aromatherapy is one such complementary therapy. These findings encourage clinicians to incorporate aromatherapy massage into maternity care. Prenatal health care teams should recruit personnel who are certified in aromatherapy massage and work with them to help pregnant women alleviate their stress and enhance maternal and fetal health. Or the authors can provide training on complementary therapies in the educational program for midwifery, and cultivate midwives to be good at using complementary therapies. In the future, the prenatal service will not only include routine prenatal care but will also incorporate stress relief and comfort interventions, for example, aromatherapy massage for women during pregnancy. The study findings also suggest that the dosage and frequency of stress-relief interventions need to be adjusted as the woman's perceived stress increases after 32 weeks GA.
This study found that salivary cortisol levels were lower immediately after aromatherapy massage, but did not show long-term effects on reducing pregnant women's stress. The possible reason might be that the aromatherapy massage provided by this study is only once biweekly, therefore, it is difficult to produce long-term effects. This dosage and frequency of aromatherapy massage may be insufficient to generate long-term effects. However, the study findings also suggest that the women's stress increased as the pregnancy progressed, especially after 32 weeks GA. Other possible reasons for the lack of long-term stress reduction are that cortisol levels are easily affected by other factors, such as circadian rhythms, seasonal changes, salivary flow rate, mood, sleep, and other life stressors. 1,23,48
This study has several strengths. First, its outcome variables were biological markers of both salivary cortisol and IgA, and were sensitive to the immediate and long-term effects of prenatal aromatherapy and massage. Second, saliva samples were collected from the participants every month from 16 to 36 weeks gestation before and after aromatherapy massage. The study closely monitors the change in the outcome variables. Third, the study is a longitudinal randomized control trial, and the results were compared with a control group.
However, there are some limitations to this study. First, it did not measure the effects of aromatherapy massage on long-term clinical outcomes or other physiological markers of immune and adrenal function (i.e., serum IgG, IgA, IgM, and dehydroepiandrosterone sulfate). Second, the sample size and the dose and frequency of aromatherapy massage may not have been adequate to produce long-lasting effects on salivary cortisol levels. Third, the attrition rate was higher in the intervention group than in the control group because of the time required for the aromatherapy massage, and some of the participants did not enjoy using the essential oils. Fourth, the sample size was small, and data were collected from only one hospital at Taipei. The results may not be generalized to pregnant women in other countries. Fifth, this study only used lavender oil for massage and did not try other essential oils that might have had different treatment effects for pregnant women. Sixth, this study only examined the effects of the combined use of aromatherapy and massage on saliva cortisol and IgA. There was no way to separate the effects of massage from the effects of the lavender oil. Future study can design four different intervention groups (massage alone, massages with essential oil, essential oils alone, and routine care) and examine the effects of the four treatments on the saliva cortisol and IgA. In addition, future studies might include other clinical outcomes and physiological markers, recruit more pregnant women, and provide various doses for different stages of pregnancy. Also, future studies might use different essential oils and compare their treatment effects. Furthermore, future research could compare the effects of various methods of aromatherapy, such as bathing, topical application, and foot soaks. In the future, the authors may develop multiple-site studies with a larger sample size.
Conclusions
Complementary therapies are being incorporated into current medical practice. This study presented evidence that aromatherapy massage could significantly reduce stress and enhance immune function in pregnant women. The study evidence can guide clinicians or midwives in providing aromatherapy massage to pregnant women throughout the pregnancy. Maternity health care teams could work with personnel certified in aromatherapy massage and provide individualized stress-relief interventions to pregnant women based on their needs. The educational program for midwifery could include training on complementary therapies and educate more midwives in providing aromatherapy massage or other complementary therapies to help promote health in pregnant women.
Footnotes
Acknowledgment
This study was financially supported by the National Science Council of Taiwan for grant support (NSC 21 99-2314-B-016-039-).
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.