
Abstract
Objectives:
This study focused on patients with bipolar disorder (BD), several years after their participation in mindfulness-based cognitive therapy (MBCT). It aimed at documenting sustained mindfulness practice, perceived long-term benefit from the program, and changes regarded as direct consequences of the intervention.
Design:
This cross-sectional survey took place at least 2 years after MBCT for 70.4% of participants.
Location:
It was conducted in two specialized outpatient units for BDs that are part of the Geneva University Hospitals (Switzerland) and the Sainte-Anne Hospital in Paris (France).
Subjects:
Eligibility criteria were a diagnosis of BD according to DSM-IV and participation in at least four MBCT sessions. Response rate was 66.4%. The final sample included 71 outpatients (71.8% bipolar I, 28.2% bipolar II).
Outcome measures:
A questionnaire retrospectively assessed patient-perceived change, benefit from MBCT, and current mindfulness practice.
Results:
Proportions of respondents who practiced mindfulness at least once a week were 54.9% for formal practice (body scan, sitting meditation, mindful walking, or movements) and 57.7% for informal practice (mindful daily activities). Perceived benefit for the prevention of relapse was moderate, but patients acknowledged long-lasting effects and persistent changes in their way of life. Formal mindfulness practice at least once a week tended to be associated with increased long-lasting effects (p = 0.052), whereas regular informal practice and mindful breathing were significantly associated with persistent changes in daily life (p = 0.038) and better prevention of depressive relapse (p = 0.035), respectively. The most frequently reported positive change was increased awareness of being able to improve one's health.
Conclusions:
Despite methodological limitations, this survey allowed documenting mindfulness practice and perceived sustained benefit from MBCT in patients with BD. Participants particularly valued increased awareness that they can influence their own health. Both informal and formal practices, when sustained in the long term, might promote long-lasting changes.
Introduction
T
Mindfulness-based cognitive therapy (MBCT) is an 8-week group program, which integrates mindfulness practice and cognitive therapy, initially developed with the objective to prevent depressive relapse in unipolar depression. 10 According to the U.K. National Institute for Health and Care Excellence (NICE) guidelines, it is currently a recommended intervention for relapse prevention in patients who have experienced more than two prior depressive episodes. 11 Because long-term morbidity data in BD indicate that the time spent in depression is about 35%, compared to 9% in hypomanic or manic episodes, 12 a few studies tested the feasibility and usefulness of MBCT in BD, mainly as adjunctive therapy. 13 –15 The first randomized controlled trial of MBCT efficacy in a small sample of patients in remission from BD showed decreased residual depression and anxiety symptoms after the intervention. 16 A later trial compared the efficacy of MBCT and treatment as usual over a 12-month follow-up period in a large sample of subjects with BD (n = 95). MBCT was associated with a reduction of anxiety, but no difference between groups was observed for depressive and manic symptoms, and time to recurrence or number of recurrences. 17 Recently, a 3-week online mindfulness-based intervention was introduced to address the specific needs of patients in the late stages of BD. 18 Preliminary data supported its feasibility and effectiveness in terms of improved quality of life immediately after the intervention, but the program warrants further development and testing.
A few studies examined MBCT effects on cognitive functioning and brain activity in BD. Following MBCT, participants in an open trial reported improvement of cognitive functioning (executive functioning, memory, and ability to initiate and complete tasks) that correlated with increased mindful and nonjudgmental observance. However, only executive functioning remained significantly improved after 3 months. 19 Another open study reported improved performance in neuropsychological tasks, such as working memory, spatial memory, and verbal fluency, together with increased activation in the medial prefrontal cortex. 20 MBCT also led to improved emotional processing in BD, as assessed by electroencephalogram parameters. 21
Regular home practice is postulated as a key element to MBCT effectiveness. A survey of 98 mindfulness interventions, which included nonclinical as well as clinical samples presenting with a wide range of physical and mental health conditions, identified 24 studies that tested the hypothesis of a positive association between mindfulness practice and clinical outcome. 22 To our knowledge, a single study examined this issue in BD. It concluded that more regular mindfulness meditation practice during the program was associated with an improvement in depression symptoms at 12-month follow-up. 23 Only 50% of participants continued to meditate at least once a week at that time.
Facing the dearth of data about post-intervention mindfulness practice and MBCT effectiveness in the long term, this survey focused on the perception of patients with BD, several years after their participation in MBCT. We sought to address the following questions: (a) document the frequency and type of mindfulness practice, (b) evaluate the perceived benefit from the program, (c) explore whether practice and perceived benefit were associated with each other and with time since participation, and (d) identify long-term changes perceived as direct consequences of the intervention.
Methods
Study design
This study was conducted in two specialized outpatient units for BD, part of the Geneva University Hospitals (Switzerland) and the Sainte-Anne Hospital in Paris (France). Both structures provide expertise in diagnostic evaluation, as well as treatment recommendations and provision. MBCT is included as a standard treatment option for patients with BD, especially in the late stages of the disorder. In keeping with naturalistic clinical conditions, patient inclusion in the MBCT program does not depend on strict criteria, except for the absence of current abuse or dependence to alcohol or other substances. Most patients have experienced several prior mood episodes and are in remission or only moderately symptomatic at admission in the MBCT program. They generally enter the program upon recommendation of their healthcare providers.
All patients who had participated in MBCT, as part of their standard treatment program, from 2006 to 2011 in Geneva and from 2008 to 2012 in Paris were eligible for this survey if they met diagnostic criteria for bipolar I or II disorder according to DSM-IV (as assessed by experienced psychiatrists) and participated in at least four MBCT sessions. They were contacted from January to February 2012 (Geneva) and January to February 2013 (Paris), either in person or by mail. They received brief information about the study and were invited to fill a questionnaire and return it, together with their written informed consent. A reminder was mailed to participants who did not respond to the first invitation. Response rate was 66.4% (71 of 107 patients). The study protocol was approved by the ethics committee of both hospitals and all participants provided written informed consent.
Mindfulness-based cognitive therapy
MBCT is based on mindfulness-based stress reduction (MBSR), which integrates a secular approach of Buddhist mindfulness, education about stress, and training in coping strategies and assertiveness. 24,25 MBCT combines the principles of mindfulness with those of cognitive therapy. 10,26 It is a group-based program that consists of weekly meetings (about 2–2.5 h duration) delivered over an 8-week period, with guided mindfulness exercises and compact disc for self-practice. Body scan, sitting meditation, as well as mindful walking or movement, are considered formal meditation practices and their duration is long compared to other practices. Informal practices aim at facilitating the generalization of mindfulness skills into everyday life, by bringing mindful attention to internal and external experiences during daily routine activities. Finally, brief centering exercises called the “three-minute breathing space” are used either at neutral times during the day or as “coping strategies” when facing difficulties (emotional challenges and stress). Group sessions were conducted by well-trained and experienced instructors. Both during and after MBCT participation, patients' medical treatment (e.g., medication and medical visits) was provided as usual.
Questionnaire
The questionnaire, used in both centers, was elaborated in Geneva by a group of experienced clinicians involved in MBCT instruction and research. It retrospectively assessed patient-perceived change (10 questions coded from 1 = major negative change to 5 = major positive change) and global benefit from the program (four questions on a visual analog scale from 1 = not at all to 10 = enormously). Mindfulness practice was also addressed as follows: frequency of different types of practice (four questions coded from 1 = never or very rarely to 6 = daily), average duration of practice (from 1 = less than 10 min to 5 = more than 45 min), most frequent practice setting (individual or group practice), and readings related to mindfulness (yes or no). The questionnaire is available upon request (original French version and provisional English version).
Data analysis
Descriptive statistics included frequencies and percentages for categorical variables, and median and range for ordinal variables. A missing value was interpreted as no change or no practice for the corresponding variables. Independent samples were compared with the Fisher exact test for categorical variables and the Mann–Whitney U test for ordinal variables. The Mantel– Haenszel test for trend and the Jonckheere–Terpstra test for trend were used to test associations with time elapsed since participation in the program. Statistics were computed using SPSS version 20 (IBM Corporation, Armonk, NY). All tests were two tailed, with significance level at 0.05.
Results
Characteristics of survey respondents are provided in Table 1. The majority of participants were females (74.6%), 50 years and older (65.6%), and without professional activity (57.4%). Diagnoses included bipolar I (71.8%) and bipolar II disorders (28.2%). All, but one, were prescribed psychotropic medication (mood stabilizers 87.1%, antidepressants 58.6%, and antipsychotics 48.6%).
MBCT, mindfulness-based cognitive therapy.
The survey took place at least 2 years after termination of the MBCT program for most patients (70.4%). Daily mindfulness practice at that time was infrequent: 4.2% for body scan or sitting meditation, 7.0% for mindful walking or movements, 11.3% for 3-min breathing space, and 14.1% for mindful daily activities. Mindfulness practice at least once a week is documented in Table 1. Formal mindfulness practice was endorsed by 54.9% of respondents. A nonsignificant decrease was observed with increasing time since MBCT participation (<2 years, 71.4%; 2–4 years, 53.3%; >4 years, 40.0%; Mantel–Haenszel test for trend, p = 0.060). Informal practice at least once a week was endorsed by 57.7% of respondents, with no effect of time since participation (p = 0.72). No significant difference was observed between patients with bipolar I and bipolar II disorders for either formal or informal practice (Fisher exact tests, p = 0.12 and p = 0.59, respectively). Practice was mostly individual, with only 25.4% of participants still involved in group practice. Duration of practice was 10–30 min for the majority of participants who practiced mindfulness (52.5%).
Perceived benefit from the MBCT program (rated on 1–10 scales) was moderate for the prevention of depressive relapse (median 5, range 1–10, n = 52) and hypomanic/manic relapse (median 6, range 1–10, n = 44). Nevertheless, long-lasting effects were acknowledged (median 7, range 1–10, n = 67): the most frequently cited effects (open question) were “being in the moment” (n = 10), “increased self- and body-awareness” (n = 7), and “relaxation and well-being” (n = 5). The program was perceived as a determinant of persistent change in participants' way of life or philosophy of life (median 6, range 1–10, n = 64). Perceived benefits tended to decrease with the time elapsed since MBCT participation (prevention of depressive relapse, p = 0.081; prevention of hypomanic/manic relapse, p = 0.063; long-lasting effects, p = 0.010; and modified way of life, p = 0.043; Jonckheere–Terpstra trend tests). No significant difference was observed between bipolar I and bipolar II diagnostic groups. Most former participants would recommend MBCT to relatives and friends (93.0%).
The relationship between perceived benefits in the long term and sustained practice was examined by comparing participants who practiced at least once a week and the ones who did not (Table 2). A tendency was observed for formal practice being associated with increased long-lasting effects (Mann–Whitney U test, p = 0.052). Respondents who practiced mindful breathing regularly reported better prevention of depressive relapse (p = 0.035), whereas the ones who were compliant with regular informal practice perceived higher levels of change in their daily life (p = 0.038). Perceived benefits in the long term did not significantly differ according to whether patients were still involved in group practice or not.
Mann–Whitney U-test.
Either body scan, sitting meditation, or mindful walking or movements.
Mindful daily activities.
Positive long-term changes perceived as direct consequences of MBCT participation are further documented in Figure 1. Frequencies of positive changes were highest for “being aware that I can help improving my own health,” “being able to care for myself,” and “being aware of what disturbs my life at the moment it occurs” (≥80% of all respondents).
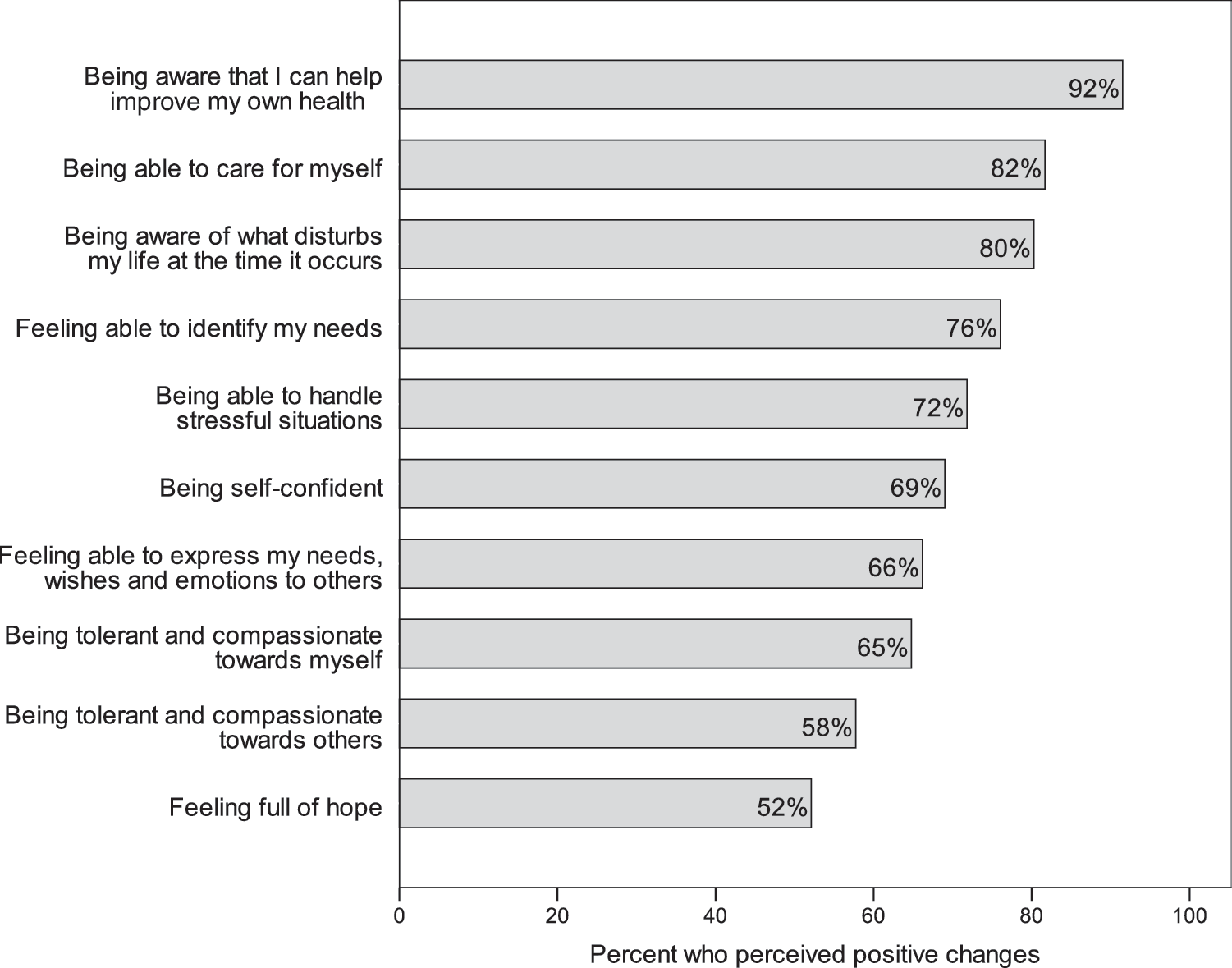
Percent of participants who perceived some or major positive changes as direct consequences of MBCT participation (N = 71). MBCT, mindfulness-based cognitive therapy.
Discussion
To the best of our knowledge, this is the first survey in patients with BD that examined mindfulness practice and perceived benefits from MBCT in the long term, more than 2 years after the program for most respondents. In contrast, efficacy studies of mindfulness-based therapy for anxiety and depression symptoms had a median follow-up period of 12 weeks, 27 whereas relapse prevention studies most often considered 14–18-month observation periods. 28
Although regular practice of mindfulness meditation is postulated to play a central role in sustained therapeutic effects, few studies have examined the amount and type of practice after termination of the MBCT program. However, a small study in BD showed that 50% of participants continued to meditate at least once a week after 12 months. 23 More than 50% of respondents to the present survey were compliant with such meditation frequency (formal and informal) more than 2 years after MBCT. Results, although encouraging, are also in agreement with an earlier study in unipolar patients that documented a significant decrease over time for formal meditation practice, but not informal practice. 29 This raises the issue of whether the original MBCT protocol 10 might need some adaptation to promote long-term adherence of patients with BD. Among a series of adjustments, Deckersbach et al. 30 proposed to introduce a stepwise approach to meditation and a gradual increase of the duration of practices, to overcome possible attention difficulties of patients with BD.
According to the staging model, treatment recommendations during the late stages of BD are to focus on approaches aimed at preventing relapse, reducing functional decline and improving patients' quality of life. Participants in this survey estimated that MBCT was moderately effective for relapse prevention. Indeed, a 12-month trial in BD did not support a protective effect of MBCT with respect to time to depressive or hypomanic/manic relapse, or number of recurrences. 17 However, patients in this study valued long-lasting benefits from MBCT, such as increased focus in the moment and greater self-awareness, as well as sustained changes in their daily life. Deckersbach et al. similarly observed improvement for a variety of outcome measures that included attention, emotion regulation abilities, psychological well-being, and psychosocial functioning. 13
Perceived positive changes in this study were congruent with an enhanced sense of self-efficacy, as reported in a relapse prevention study in depression. 31 Self-efficacy has been proposed as a potential mediator of the relationship between greater use of mindfulness skills and improved emotion regulation difficulties. 32 Underlying mechanisms might include perceptual redistancing leading to increased acceptance, reduced anxiety response, and greater self-awareness and self-motivation. 33 A review of 14 qualitative MBCT and MBSR studies in different diagnostic groups led to describe the patients' process of transforming their relationship to the illness experience with four components, which were labeled sense of control, acceptance, command over the body, and ability to take action. 34 Various “top-down” and “bottom-up” emotion regulation strategies have been examined in relationship with mindfulness practice. 35
The effectiveness of mindfulness is expected to increase with additional practice and integration of skills. In BD, the amount of mindfulness practice during the 8-week program was associated with improved depression symptoms at 12 months, suggesting that a deeper engagement in the practice might better protect against psychiatric symptoms. In contrast, sustained practice throughout the 12-month follow-up period was not associated with symptom reduction. 23 According to a review of articles evaluating the relationship between mindfulness practice and clinical outcome, only about half provided at least partial support to the expected association. 22 The question of which aspect of mindfulness practice is important (i.e., duration, frequency, quality, or a combination of these aspects) has led to emphasize the need to monitor the quality of mindfulness practice using specific instruments. 36 Another issue is to distinguish between different types of practices (e.g., longer formal meditation practices vs. more flexible informal practices during daily life activities) and their effect on different possible outcomes (e.g., state mindfulness scores, psychiatric symptoms, relapse rate, or quality of life measures). Results are controversial in this respect. More intensive formal practice during MBCT was associated with a reduced risk of relapse in depression. 37 Conversely, in generalized anxiety disorder, beneficial effects on worry, clinician-rated anxiety, and quality of life were associated with the amount of post-treatment informal practice, but not formal practice. 38 This survey provides preliminary support to the role of flexible informal practice with respect to long-lasting changes in the daily life of patients with BD.
Interestingly, sustained practice of short breathing exercises was associated with the perception of better efficacy with respect to the prevention of depressive relapse, but not hypomanic/manic relapse. On the one hand, one may hypothesize that patients' tolerance toward prodromes of depression might be lower than toward signs of escalating mood, postponing the introduction of relapse prevention strategies in the latter situation. On the other hand, one may postulate that specific practices might be needed to prevent depressive and hypomanic/manic relapse, respectively. In particular, mindful walking or movements may allow more grounding and focus in times of acceleration, increased energy, and distractibility. 30
Several shortcomings of this study need to be pointed out. First, recruitment in specialized outpatient units for BD and limited sample size preclude generalization to more diverse populations, despite a good response rate. Second, we cannot exclude some social desirability bias or acquiescent response bias in reporting perceived benefit and changes. Third, the cross-sectional study design did not allow taking into account some relevant factors, such as pharmacological or psychological treatment during and after MBCT, actual depressive and hypomanic/manic relapse since program termination, or changes in the amount and quality of practice over time. We also did not adjust for possible confounders, such as the severity of depressive or manic symptoms, when questionnaires were completed. As a consequence, no causal inference can be made with respect to the observed relationship between mindfulness practice and perceived benefit from MBCT.
Conclusions
Despite limitations, this survey speaks in favor of MBCT as an acceptable and beneficial approach in BD. Participants particularly valued increased awareness that they can influence their own health. Both informal and formal practices, when sustained in the long term, might promote long-lasting changes. Future prospective studies should further examine the amount and quality of home practice over time, explore the barriers to practice, and evaluate the impact of means to enhance adherence on different possible target outcomes.
Footnotes
Acknowledgment
We thank Sandra Ter Pelle for her expert technical assistance in article preparation.
Author Disclosure Statement
G.B. is a member of an advisory board for Pfizer, but there is no conflict of interest with this study. For the remaining authors, no conflict of interests is declared.