
Abstract
Objectives:
To determine the efficacy of a high-velocity low-amplitude manipulation of the thoracolumbar junction in different urologic and musculoskeletal parameters in subjects suffering from renal lithiasis.
Design:
Randomized, controlled blinded clinical study.
Settings/Location:
The Nephrology departments of two hospitals and one private consultancy of physiotherapy in Valencia (Spain).
Subjects:
Forty-six patients suffering from renal lithiasis.
Interventions:
The experimental group (EG, n = 23) received a spinal manipulation of the thoracolumbar junction, and the control group (CG, n = 23) received a sham procedure.
Outcome measures:
Pressure pain thresholds (PPTs) of both quadratus lumborum and spinous processes from T10 to L1, lumbar flexion range of motion, stabilometry, and urinary pH were measured before and immediately after the intervention. A comparison between pre- and postintervention phases was performed and an analysis of variance for repeated measures using time (pre- and postintervention) as intrasubject variable and group (CG or EG) as intersubject variable.
Results:
Intragroup comparison showed a significant improvement for the EG in the lumbar flexion range of motion (p < 0.001) and in all the PPT (p < 0.001 in all cases). Between-group comparison showed significant changes in PPT in quadratus lumborum (p < 0.001), as well as in the spinous processes of all of the evaluated levels (p < 0.05). No changes in urinary pH were observed (p = 0.419).
Conclusion:
Spinal manipulation of the thoracolumbar junction seems to be effective in short term to improve pain sensitivity, as well as to increase the lumbar spine flexion.
Introduction
T
The etiologic factors of kidney stone formation are complex and diverse and involve genetic, metabolic, and environmental risk factors, 3 some of which may be adjustable, 4,5 so that the stone formation usually results from an imbalance between factors that promote urinary crystallization and those that inhibit crystal formation and growth. 6 The most important data appear to be related to the links between genetic variability and urine calcium excretion and pH, so these risk factors seem to be at the very center of the problem of kidney stone disease. 6 Therefore, urinary pH is a decisive element to be considered in supersaturation of many stones 6,7 ; thus, it should be taken into account that both highly acidic urine (pH ≤5.5) and highly alkaline urine (pH ≥6.7) predispose patients to calcium kidney stone formation.
All stones share similar presenting symptoms. 8 Most patients present with moderate-to-severe colic where the painful area is determined by the location of stone in the urinary system. It may also be accompanied by other possible symptoms, such as dysuria, urination urgency and frequency, 7 and autonomic manifestations. Less often, patients present with silent ureteral obstruction, unexplained persistent urinary infection, or painless hematuria.
There are scarce studies on the use of physical therapies as a hypoalgesic measure against renal lithiasis (RL) 9,10 and even less on the use of manual therapy or spinal manipulative therapy (SMT). 11,12 As far as the authors are concerned, there are no randomized clinical trials on the application of SMT on patients suffering from RL.
The purpose of this study was to evaluate the immediate effect of thoracolumbar spinal manipulation in pressure pain threshold (PPT) in the thoracolumbar region, in the back range of motion, in postural control and balance, and in urinary pH-metry in subjects suffering from RL.
Materials and Methods
Study design
The study consisted in a controlled randomized double-blind clinical trial (Registration of clinical trials: Australian New Zealand Clinical Trials Registry 13/05/2014: Registration Number ACTRN 12614000506695).
Randomization and blinding procedures
To randomize patients into their respective groups, a randomized number table designed by an Internet website (
Blinding
Subjects remained unaware of the number of study groups and the treatment allocation group, whereas evaluators who collected or analyzed data remained unaware of critical study factors and also the treatment allocation group to ensure participant blinding and outcome assessor blinding, respectively. 13 The clinician in charge of the intervention did not participate in the assessment protocol and was not aware of the purposes of the study.
Study and sampling population
Those subjects meeting the study criteria were selected according to nonprobabilistic consecutive sampling techniques and were recruited for the study from the Nephrology Departments of two hospitals and one private consultancy of physiotherapy in Valencia (Spain).
Considering a bilateral contrast with an alpha risk of 0.05 and a beta risk of 0.20 and assuming a common standard deviation of 0.6, as well as the lack of losses during the monitoring, a sample size of 23 subjects per group was estimated through the Granmo online v7.12 software [
Inclusion and exclusion criteria
The inclusion criteria for participants were: (1) subclinical RL diagnosed by a Nephrology specialist (following the European Association of Urology criteria) 14 ; (2) ages between 25 and 55 years; and (3) signing the informed consent.
Patients with any of the following characteristics were excluded: (1) having suffered from nervous tissues or bone tumors, inflammatory rheumatism, infectious diseases, or other nonlithiasic nephropathies; (2) pregnancy; (3) central or peripheral neurologic pathology or suffering or having suffered pathologies showing impaired balance; (4) breathing disorders capable of changing the urinary pH; (5) contraindications for the intervention technique; and (6) having taken some kind of medication within the last 72 h.
Participants
Fifty-one subjects suffering from subclinical RL were evaluated for their participation in the study; however, only 46 (n = 46) subjects met the selection criteria. Participants were randomized in two groups: the control group (CG) and the experimental group (EG). The final sample included 27 men (59%) and 19 women (41%) with an average age of 38.5 (standard deviation [SD] = 6.80) and a body–mass index (BMI) of 25.07 (SD = 3.12). No loss to follow-up was recorded during the data collection or analysis phases. The study protocol followed the CONSORT guidelines 15 (Fig. 1).
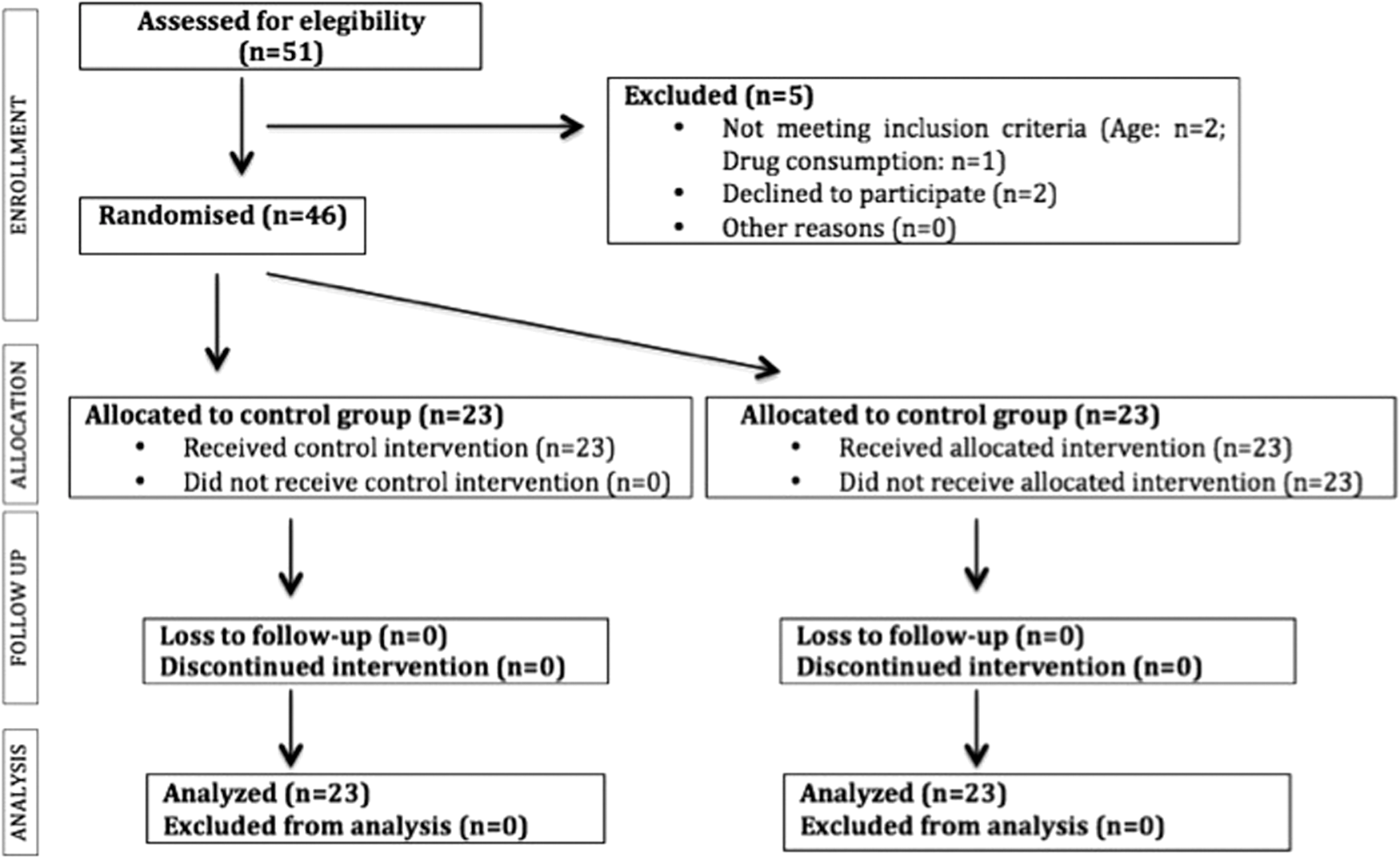
Flowchart according to the CONSORT statement for randomized trial reports.
Study protocol
Participants received the evaluation and intervention protocol together in one session. The therapist and the evaluator were both experienced senior physical therapists and osteopaths.
The assessor carried out the preintervention measurements; subsequently, the therapist performed the assigned intervention; and 10 min later, the evaluator repeated the said postintervention measurements. All measurements were performed in the morning. 16 The patients were asked to attend the consultancy about 2 h after having had breakfast and not having practiced any exercise throughout the morning in which the study was conducted. 17,18 The sequence of all measurements was performed in the same way for both the EG and for the CG.
PPT on the spinous processes and the quadratus lumborum muscle
The digital compression dynamometer PCE FM-200 (PCE, Meschede, Germany) was used. The PPT was measured on T10 to L1 spinous processes with the subject placed in prone position 19 and in the trigger point of the quadratus lumborum (QL) just below the 12th rib with the subject placed in lateral decubitus and the homolateral upper limb placed above the head. 20 The algometer pointer was placed perpendicular to the point of evaluation, increasing the pressure force with a constant rate of 1 kg/cm2/s evenly and continuously until the perception of a tender point. 21 Patients were asked to inform when they felt a change in the feeling of pressure pain and then the evaluator stopped applying pressure, taking the appropriate register. 22 The algometer remained with the display in a position where the evaluator could not see it until the signal of the patient. Three measurements were made, taking the mean as the reference value. Ten seconds were waited between each one of the three measurements and 20 sec when changing the point. 23
Evaluation of back range of motion
Trunk flexion was measured using a digital inclinometer, BASELINE model (New York), recommended by the AMA Guide (American Medical Association). 24 Patients were in their underwear, standing barefoot, arms hanging, knees extended, separated feet to the width of their hips, and without hip rotation. They were asked a maximum trunk flexion with knees extended and arms hanging down. 25 The inclinometer was placed on the spinous process of T12, and trunk flexion was requested following the above instructions. Three proper measurements were made, leaving 30 sec between each 26 and taking the mean as the reference value. 27
Urinary pH analysis
The measurement was performed with the pH-meter Oakton Waterproof pHTestr 30 Pocket pH Tester (Oakton, Barcelona, Spain). The pH study was performed within the first 2 h after the sample was taken. Following the European guidelines the mean portion of urine was collected, after washing the external genitalia. The tip of the pH-meter was immersed about 2 cm in the container with urine, it was stirred, and the authors waited for the reading to stabilize. 28
A urinary pH measurement was performed before the intervention, and this measurement was repeated for the first urine after the intervention.
Postural control and balance
The stabilometry and baropodometry platform PODOPRINT of Namrol (Barcelona, Spain) were used. This instrument allows to collect the following variables related to postural control and balance: X and Y mean oscillation, average speed and stroke length, anterior and lateral mean variation, and L/S parameter (the ratio of stroke length and the surface of the ellipse). Before the measurement, the patient was explained what the whole process involved 29 and the correct way to stand on the platform. 30 Three measures of 30 sec each were performed, taking the third measure. 31 After each reading, patients were asked to take a step back and leave the platform, after which the measurement process started again until all three measurements were completed. 32
Intervention in the EG
Based on the sympathetic innervation of the kidneys 33 and the fact that spinal manipulations modulate some organ functions in some cohorts, 34 the therapist applied a thrust manipulation of the thoracolumbar junction that can be described as Ref. 35 (Fig. 2).

Indirect manipulation technique of the thoracolumbar junction.
The patient was placed first on her/his side, with the contralateral lower limb flexed and his/her foot resting on the popliteal fossa of the other lower limb, which remained in extension. Thus a flexion parameter is also placed on the upper lever with a rotation in the region of 5–10° up to T12-L1 and then in the lower lever, for which the upper lower limb is flexed and where the rotation will be about 20° until reaching the level to manipulate (T12-L1). The therapist, who is in front of the patient, has his rear leg flexed and resting on the lower limb of the patient. The caudal hand presses on the inferior articular apophyses of T12, contralateral to the side that the patient is lying on, while the cranial hand rests on the chest of the patient. From that premanipulative position, the therapist performs a force of high speed at the end of the available range of motion, rotating the patient toward the side he is lying on. This rotational movement of low amplitude is executed through a traction of the pelvis forward, while the therapist's leg resting on the lower limb of the patient makes a sharp knee extension to further rotate the pelvis forward. Since autonomic effects can be unilateral, 36,37 this technique was made bilateral at the level T12-L1 only once. After the intervention, the patient was at rest for 10 min.
Intervention in the CG
The CG received a placebo maneuver. 38 The subject was lying in supine position. The therapist placed one hand on the sacrum and the other hand on the middle thoracic region, without performing any action for 90 sec. A rest time of 10 min was also taken before taking the postintervention measurements.
Data analysis
Data were analyzed and processed using the statistical package R, version 3.0.1 (
At baseline, the mean and standard deviation were described (for quantitative variables with normal distribution), or medians and percentiles [P25–P75] (for those without a normal distribution). To assess the normality of distributions, the Shapiro–Wilk test was performed for each of the variables analyzed.
The existence of baseline differences was analyzed between both groups using both parametric tests (Student's t test for independent samples) or using nonparametric tests (Wilcoxon–Mann–Whitney) based on the results of the normality test.
For comparison between the pre- and postintervention phase (intrasubject differences), the differences between variables were calculated, and the Shapiro–Wilk normality tests were applied to the changes to determine the adequacy of parametric tests (Student's t test for intrasubject measurements) and nonparametric tests (Wilcoxon test). Due to the small sample size, all contrasts were repeated in the nonparametric version in the variables with a normal distribution.
An analysis of variance for repeated measures was performed using time (pre- and postintervention) as intrasubject variable and group (CG or EG) as intersubject variable. In those variables in which statistically significant between-group differences were found at baseline measurements, the preintervention value was included as a potential covariable (analysis of covariance) to adjust the effect. The statistical analysis was conducted considering statistically significant p value <0.05.
Ethical considerations and data protection
The study was conducted according to the Code of Ethics of the World Medical Association (Declaration of Helsinki), 39 and the data privacy was respected. 40 Before randomization, all participants were informed of the general aspects of the trial, including, among others, the aims, methods, institutional affiliations of the researchers, possible benefits, risks, side-effects of assessments and interventions, and the right to withdraw consent to participate at any time without reprisal. The subject filled in and signed an informed consent form, as established by the Declaration of Helsinki. The study received approval of the Institutional Ethics Committee of the Scientific European Federation of Osteopaths.
Results
The CG was composed of 23 subjects, 57% were men, with a mean age of 38.65 ± 6.20 years and a mean BMI of 25.12 ± 2.87 kg/m2. The EG was composed of 23 subjects, 61% were men, with a mean age of 38.34 ± 7.48 years and a mean BMI of 25.03 ± 3.41 kg/m2. No differences between groups were found at baseline in any of the control variables collected.
Table 1 shows the baseline physical and clinical characteristics of the study sample and compares the existence of differences between groups. Despite randomization, significant baseline differences were found between groups in almost all algometry values and those of the inclinometry and in values of average lateral variation in the stabilometry. Moreover, it is appreciated that the values of PPT in the QL muscle and all variables related with stabilometry (except for the mean X and mean Y) did not follow a normal distribution.
Data are reported as mean (SD) or as median [P25–P75].
L/S, length/surface; SD, standard deviation.
In regard to the score differences after intervention, Table 2 indicates the intragroup comparison results. There was a very significant increase in the range of trunk flexion in the EG (p < 0.001). The EG also observed a very significant increase in the PPT in both muscles (right and left QL; p < 0.001 in both cases) and at the level of the thoracic and lumbar spinous process (p < 0.001 in all cases). There were no differences between treatments in the other variables analyzed. In the CG there was also a significant decrease in the PPT of the spinous process of T12 and L1.
Data are reported as mean (SD) or as median [P25–P75]. p-Value: intragroup comparison between pre- and postintervention results.
Table 3 lists the intergroup comparison of differences from postintervention to preintervention values. There were significant differences, with better values for the EG, for PPT in the right QL [p < 0.001; F(1.39) = 49.623; R2 = 0.636] and in the left one [p < 0.001; F(1.39) = 35.586; R2 = 0.527]; and also in the spinous process of all levels valued: T10 [p < 0.001; F(1.39) = 26.507; R2 = 0.461]; T11 [p < 0.001; F(1.39) = 80.481; R2 = 0.716]; T12 [p < 0.001; F(1.39) = 103.173; R2 = 0.763]; L1 [p < 0.001; F(1.39) = 40.820; R2 = 0.731]; and in the range of motion in the level T12-L1 [p < 0.001; F(1.39) = 48.686; R2 = 0.603].
Data are reported as mean ± SD and (95% confidence level). p-Value: intergroup comparison between pre- and postintervention values (ANOVA).
ANOVA, analysis of variance.
Discussion
The average age of people in the study coincided with most of the studies reviewed, where the highest incidence of RL occurs around age 40. 41 Not surprisingly, the mean scores of BMI were above 25 and, therefore, can be classified as overweight or obese grade I. 4,42
Spinal manipulation increased trunk flexion at T12-L1 levels in the EG. The mechanical force introduced into the spine during SMT may alter the segmental biomechanics through the release of adhesions, the trapped meniscus, or reducing the distortion of the annulus fibrosus. 43 This might explain the increase in the articular mobility. The authors believe that the increased mobility reflected in the study patients must be motivated by the presence of a restriction affecting the thoracolumbar region. 44,45 It should be considered that it is known that the effects of a spinal manipulation on stiffness are restricted to the manipulated level. Therefore this result can be due to the detailed and specific maneuver which was applied. 46 One of the clinical manifestations of visceral dysfunction in the large intestine is the presence of taut bands in the paravertebral lumbar muscles. 47 Thus, the significant increase recorded in inclinometry as a result of the applied treatment may also be explained by a decrease in the paravertebral lumbar and QL muscle tone. It could be a consequence of a sensitization process due to the presence of the kidney suffering, which might produce a spasm of the neuromeric musculature, that is, which are included in the same metamere than the kidney, as it has been shown in previous studies. 44,48
It also produced a significant improvement in the average lateral variation in the EG postintervention, which the authors think may be due to an improvement in the patient's proprioceptive system as a result of the manipulation. 40 SMT can improve postural control, forcing the nervous system to a greater proprioceptive response, so that it detects and reacts more quickly to changes in its center of gravity. Perhaps, if the sample had been larger, other stabilometric parameters could also have changed significantly.
Similarly, the manipulation increased PPT at the level of the spinous processes of the vertebrae related to the autonomic innervation of the kidney. 49 QL muscles, which are related anatomically and through neurologic innervation, 50,51 also showed increased PPT.
This improvement was obtained despite the fact that the experimental PPT was significantly lower in baseline measures, which probably puts more emphasis on the importance of the result.
Several studies have shown the existence of referred visceral hyperalgesia to somatic tissues based on different mechanisms in the case of recurrent and/or prolonged visceral stimuli. 52 These referred visceral hyperalgesia findings have been reproduced in animal models such as those generated by the formation of artificial stone in one ureter in rats. 53,54 This has also been studied in patients with kidney stones. It has been proved that lumbar muscle hyperalgesia, in addition to the rest of parietal tissues valued corresponding to the somatic areas of the body wall located in the same neuromeric field as the organ in question, appears soon after the first or second colic. This lumbar muscle hyperalgesia increases with the repetition of the colic, is detectable between the painful episodes (pain-free interval), and even in 90% of the cases persists in some degree, mostly at muscular level, after elimination of the urinary stone for months–years (even up to 10 years). It happens even without current instrumental evidence of a new calculosis or other pathology of the urinary tract. 55 That is to say, this phenomenon often outlasts not only spontaneous pain but also the presence of the primary pain trigger in the internal organ, to the extent that the somatic manifestation could be the only manifested symptom in subjects with visceral suffering. 56
As for the approach of RL using SMT, case reports of unusual presentation have been described where mild reduction in pain and transient remission of symptoms were obtained, respectively. 11,12 However, the neurophysiologic mechanisms underlying the effectiveness of spinal manipulation to reduce pain are not fully known. Various pathways have been proposed, such as the activation of the endogenous opioid system and/or presynaptic inhibition of nociceptive pathways, 43 as well as the inhibition of the production of pro-inflammatory cytokines, 43,57 or the stimulation of mechanoreceptors that would participate in the pain gating, resulting in somatosomatic and somatovisceral reflexes. 58
The literature confirms that mechanical stimulation of the spine modulates some organ functions in some cohorts. 34 However, no significant differences were seen in urinary pH in their study, so in the short term, the spinal manipulation did not change the visceral status. Maybe in studies with a longer follow-up period and subsequent interventions, a change in the renal function and, consequently, the urinary pH could be achieved.
Limitations of the study
It should be taken into account that a nonrandomized sampling was performed, and the potential self-selection bias, due to the voluntary nature of the participation of the subjects. It should also be considered the baseline between-group differences in some of the studied variables. The effects of these differences have been minimized by using the preintervention values as covariables. Furthermore, it was the EG the one that showed worse preintervention values.
The study has a very significant effect in the short term, but it would be interesting to assess how long the changes are maintained in the medium/long term. It would also be noticeable to evaluate possible changes in the medium/long term in those variables which in the short term have not showed to be significant, such as the urinary pH. It would have been interesting to include the assessment of catecholamine levels to help explain the increase in PPT, such as studies with similar rationale have done. 59
There is an absence of guidelines to design the most reliable placebo for manual randomized controlled trials. 60 The authors have used a sham maneuver based on light touch, such as other recent studies have done. 61 However, there are no studies confirming that this is an adequate control. Future studies should consider assessing the success of subject blinding and ensuring inertness of their place a priori as a minimum standard for quality. 62
To finish with, the authors consider suitable to perform further studies where several techniques are combined 63 to evaluate whether the effect of the interaction is greater than the effect of an isolated technique.
Conclusions
The bilateral vertebral manipulation of the thoracolumbar junction seems effective in patients with RL to improve algesic sensitivity in the thoracolumbar region at the level of the QL muscle, to increase spinal range of motion in flexion and also to improve the average lateral variation as a stabilometric manifestation of the proprioceptive system. Regarding the urinary pH and other stabilometric parameters, no significant differences have been found.
Footnotes
Acknowledgments
This study was approved by the Ethical Committee of the Scientific European Federation of Osteopaths.
Authors' Contributions
A.O.P.-V. and C.R.-B. designed the study. A.O.P.-V., R.P.-R., F.R., and M.A.F.-S. conducted the literature research. R.P.-R. and P.E.-A. were responsible for data acquisition. A.O.P.-V., J.C.F.-D., and C.R.-B. were involved in data analysis. A.O.P.-V., J.C.F.-D., and M.A.F.-S. were involved in writing the article. All authors were responsible for drafting the article and have read and approved the final version.
Author Disclosure Statement
No competing financial interests exist.