
Abstract
Background:
Acute radiation proctitis (ARP) is a common side-effect that affects up to 50% of patients receiving radiotherapy. The aim of this study was to evaluate the role of a topical preparation of Aloe vera in the treatment of ARP induced by radiotherapy of pelvic area.
Subjects and Interventions:
In this double-blind placebo-controlled trial, 20 consecutive patients with ARP after external-beam radiation therapy (46–72 Gy) of pelvic malignancies were randomized to receive either Aloe vera 3% or placebo ointment, 1 g twice daily for 4 weeks. These patients presented with at least two of the following symptoms: rectal bleeding, abdominal/rectal pain, diarrhea, or fecal urgency. These symptoms were rated by the patients in terms of their severity (grade 0–4) for each of the symptoms mentioned earlier at baseline and then weekly for 4 weeks. A symptom index was calculated by the addition of the scores (16 most symptomatic). Radiation Therapy Oncology Group (RTOG) acute toxicity criteria and psychosocial status of the patients were also recorded weekly. The lifestyle impact of the symptoms was assessed by questionnaire grading from 0 (no effect on daily activity) to 4 (afraid to leave home).
Results:
There was a significant (p < 0.05) improvement in the symptom index (before treatment vs. after treatment with Aloe vera) for diarrhea (median score: 0.67 vs. 0.11), fecal urgency (median score: 0.89 vs. 0.11), clinical presentation total (median score: 4.33 vs. 1.22), RTOG total (median score: 2.89 vs. 0.89), and lifestyle (median score: 1.1 vs. 0.33). Hemorrhage and abdominal/rectal pain did not improve significantly. The odds ratios for advantage of Aloe vera over placebo for “clinical presentation total” and “RTOG total” were 3.97 (1.3–11.9) and 5.9 (1.6–21.6), respectively.
Conclusion:
A substantial number of patients with radiation proctitis seem to benefit from therapy with Aloe vera 3% ointment.
Introduction
R
A variety of treatment agents have been investigated for treatment of radiation-induced proctitis, such as anti-inflammatory agents, 3 topical steroid solutions, 4 bipolar electrocoagulation, 5 hyperbaric oxygen, 6 laser application, 7 formalin-soaked gauze, 8,9 and short-chain fatty acid enema 10 ; however, unfortunately, there is no widely accepted prophylactic or effective treatment for radiation proctitis.
The molecular mechanism of ARP involves reactive oxygen metabolites and is believed to be a result of oxidative stress, 11 though the exact mechanism is unknown. Aloe vera has been known as a traditional folklore medicine for the treatment of a range of diseases, including accelerating the wound healing and treatment of burn injuries in both experimental and clinical studies, and also mucositis induced by radiation or chemotherapy. 12 –16 Some suggest that its effectiveness in treating wounds and burns and in reducing inflammation is mediated through inhibition of cyclooxygenase, 17 but the exact mechanism of action is not fully recognized. So, because of mentioned pathophysiology of radiation-induced proctitis and also antioxidant and anti-inflammatory properties of Aloe vera, we hypothesized that it may be beneficial in the treatment of radiation proctitis too.
The aim of the present study was to determine whether Aloe vera ointment is beneficial in the treatment of ARP. This is the first randomized study of Aloe vera for treatment of proctitis in patients undergoing pelvis radiotherapy. In addition to elimination of proctitis symptoms as our primary endpoint, we evaluated secondary endpoints, including quality of life (QOL) and psychosocial status, by using Hospital Anxiety-Depression (HAD) Scale.
Methods
Ethics considerations, setting, and patients
This study was a randomized, double-blind, prospective, placebo-controlled trial comparing Aloe vera with placebo ointment. After obtaining approval from the Ethical Committee of Mazandaran University of Medical Sciences (Ethics Code: IR.MAZUMS.REC.94–1196), the study proposal was submitted, approved, and registered by the Iranian Registry of Clinical Trials (IRCT) with a registry code of RCT201606042027N6. This clinical trial was carried out in the radiotherapy department of Imam Hospital, a referral center affiliated to Mazandaran University of Medical Sciences (Sari, Iran). All patients who were enrolled in the study were 18 years or more and underwent irradiation for pelvic cancers.
Exclusion criteria were evidence of active infection, evidence of other sources of hematochezia including colon cancer, inflammatory bowel disease, hemorrhoids, anal incontinence, anorectal fistula, anorectal stenosis, previous rectal surgery, pregnancy or breast feeding, females of child-bearing age not taking adequate contraception, known allergy to any ingredients of the ointments, and concomitant use of antibiotics or steroids.
Preparation and formulation of Aloe vera ointment
We applied pure spray-dried Aloe vera powder (Giah salamat nasim faraz, Shiraz, Iran). This product consists of the inner gel from the plant.
First, the powder product was analyzed for microbial contaminants. Since the culture results were positive and because of the lyophilized nature of the Aloe product, it was sterilized with gamma waves by Atomic Energy Organization of Iran.
To formulate the ointment, first, 9 g of Aloe vera powder was ground with a mortar to a very fine powder. Next, the yielded powder was levigated with 7 g of liquid white paraffin. Then, the mixture was intimately blended with 284 g of vaseline by the geometric method.
Afterward, the whole mass was passed through a triple-roller ointment mill ointment grinding machine (D-63150; Erweka, Heusenstamm, Germany) to get smooth and super fine blending ointment. Finally, the Aloe vera ointment was filled in similar lacquered aluminum collapsible tubes under laminar flow hood to provide an aseptic environment and to ensure a sterile condition. Each tube weighed 50 g. The ointment contained Aloe vera gel powder 3%. A six-digit random code was labeled on each tube. Our experimental research and formulations were carried out under sterile conditions.
Patients and study procedure
During the period of October 2015 to November 2016, 89 patients completed a cycle of external-beam radiation therapy to the pelvis (46–72 Gy) for pelvis malignancies. Enrolled in the study were 20 patients (13 male and 7 female, with a median age of 57.55 years old) who were presenting ARP syndrome during their radiation therapy. Patients were randomly allocated by random number table, and a similar lacquered aluminum collapsible tube containing Aloe vera or placebo was delivered to each patient. For ethical reasons, all patients with ARP received sulfasalazine 500 mg four times a day (QID) to ameliorate ARP symptoms, though this is not a very well accepted treatment for ARP 1 (Fig. 1). The diagnosis of radiation proctitis was defined as the occurrence of loose stools and tenesmus lasting more than 7 days, associated with at least two of the following symptoms: greater than four bowel movements per day, rectal bleeding, fecal urgency, and abdominal/rectal pain. 18
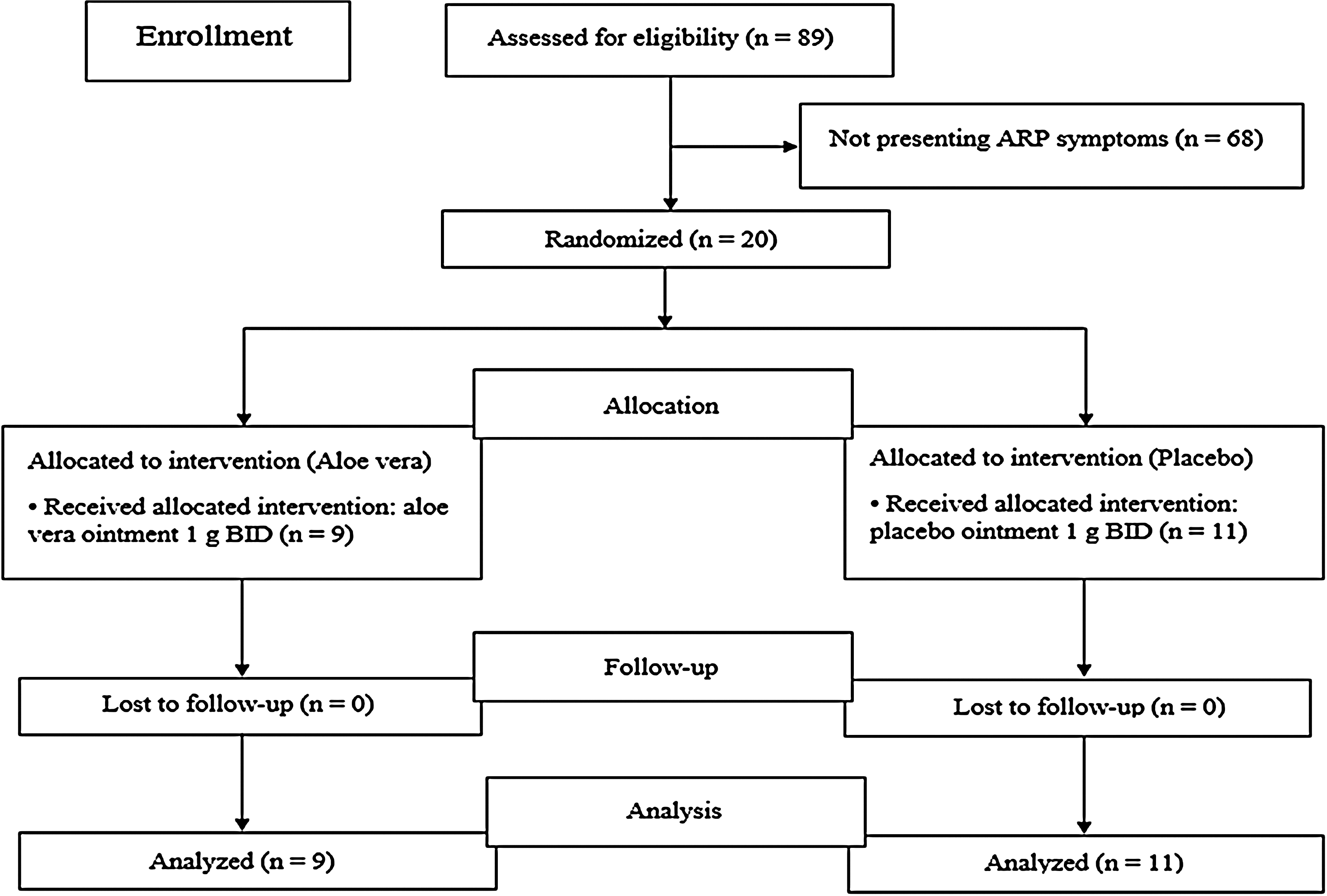
Flow diagram of the study.
The symptoms of ARP were observed in 20 patients: 11 belonging to the placebo arm and 9 to the Aloe group, respectively. Patient age ranged from 24 to 84 years. Every week, patients received five daily fractions of 1.8–2 Gy, a total dose of 50–72 Gy, with a four-field box centered on the pelvis. Patients were instructed to use ointment rectally (Aloe or placebo) for 4 weeks, 1 g twice daily.
The ointment lacquered aluminum collapsible tubes looked identical. The patients, the radiotherapist, healthcare providers, and the investigator of clinical responses were all blinded to the arms of the study. Also, all data were gathered by a single investigator. Patients were assessed a day before and then weekly during radiotherapy for 4 weeks. Compliance was assessed by asking the patients to bring the remainder ointment tubes for weekly visits.
Questionnaires on demographic and clinical details of each patient, including cancer diagnosis, co-morbidity, previous treatments, and the radiation dose, were filled out by the investigator. The clinical activity of ARP was assessed by recording bowel movements/stool consistency, rectal bleeding, abdominal/rectal pain, fecal urgency, and from a self-rating based on the impact of symptoms on life activities. For each factor, a scale from 0 (not present) to 4 (causing significant discomfort) was used. The maximum overall score was 16, and the minimum score required for enrolment was 4 (a score of at least 2 from two discrete symptoms mentioned earlier, concurrently). All our 20 patients completed the study. Clinical presentation score total was calculated by the sum of four specific symptoms (e.g., bowel movements/stool consistency, rectal bleeding, abdominal/rectal pain, fecal urgency).
Radiation-induced toxicity was evaluated weekly by using the Radiation Therapy Oncology Group (RTOG) criteria (Table 1) 19 and based on the clinical presentation (Table 2). 11
BMI, body mass index; HTN, hypertension; NSAIDs, non-steroidal, anti-inflammatory drugs; SD, standard deviation.
The impact of these symptoms was also graded by using a questionnaire regarding the effect of these symptoms on lifestyle (Table 3). 11
Possible score range: 0–16.
We appraised the psychosocial status of the patients by applying HAD Scale. 20 The patients were requested to weekly fill out the HAD form considering their feelings during the past week.
Calculation of sample size and randomization
According to the pilot study, the minimum expected difference between mean values of the total clinical presentation score before and after Aloe vera consumption was considered as 3 score; and also, a standard deviation (SD) of 2 score was expected for the calculation of sample size. Power was set as 80% for the calculation of sample size. With an allowance of 10% lost to follow-up rate, we allocated 11 people to the control group and 9 people to the treatment group.
The patients who met the eligibility criteria were assigned into one of the intervention groups, by using a permuted block randomization method. Blocks of four were used for this purpose. Each ointment was given a six-digit number by the principal investigator. The patients, the treatment team, and the investigator of clinical responses did not know the types of the interventions. At the end of the study, the principal investigator decoded the consumed ointment numbers and assigned each to the appropriate group correctly.
Statistical analyses
Qualitative variables were reported by frequency and percent, and quantitative variables were reported by Mean ± SD. Chi-square test and Fisher's Exact Test were used to compare the qualitative variables in the two groups of the study. To analyze the quantitative variables, Mann–Whitney Test was used. A generalized linear model with a repeated-measures test was used for time-trend assessment and time-intervention interaction. For estimating the odds ratio between groups, logistic regression was used. All statistical analysis was conducted by using SSPS software version 19, and differences with a value of p < 0.05 were considered significant.
Results
Participants
The flowchart of enrollment of the patients is displayed in Figure 1. Demographic and baseline clinical characteristics of patients are presented in Table 4. As indicated, there was no significant difference between the two groups in demographic and clinical characteristics (age, gender ratio, body–mass index, total dose and dose of radiotherapy in each session, concomitant medication, and comorbidities).
Possible grade range: 0–4.
Effect of Aloe vera rectal ointment on symptoms
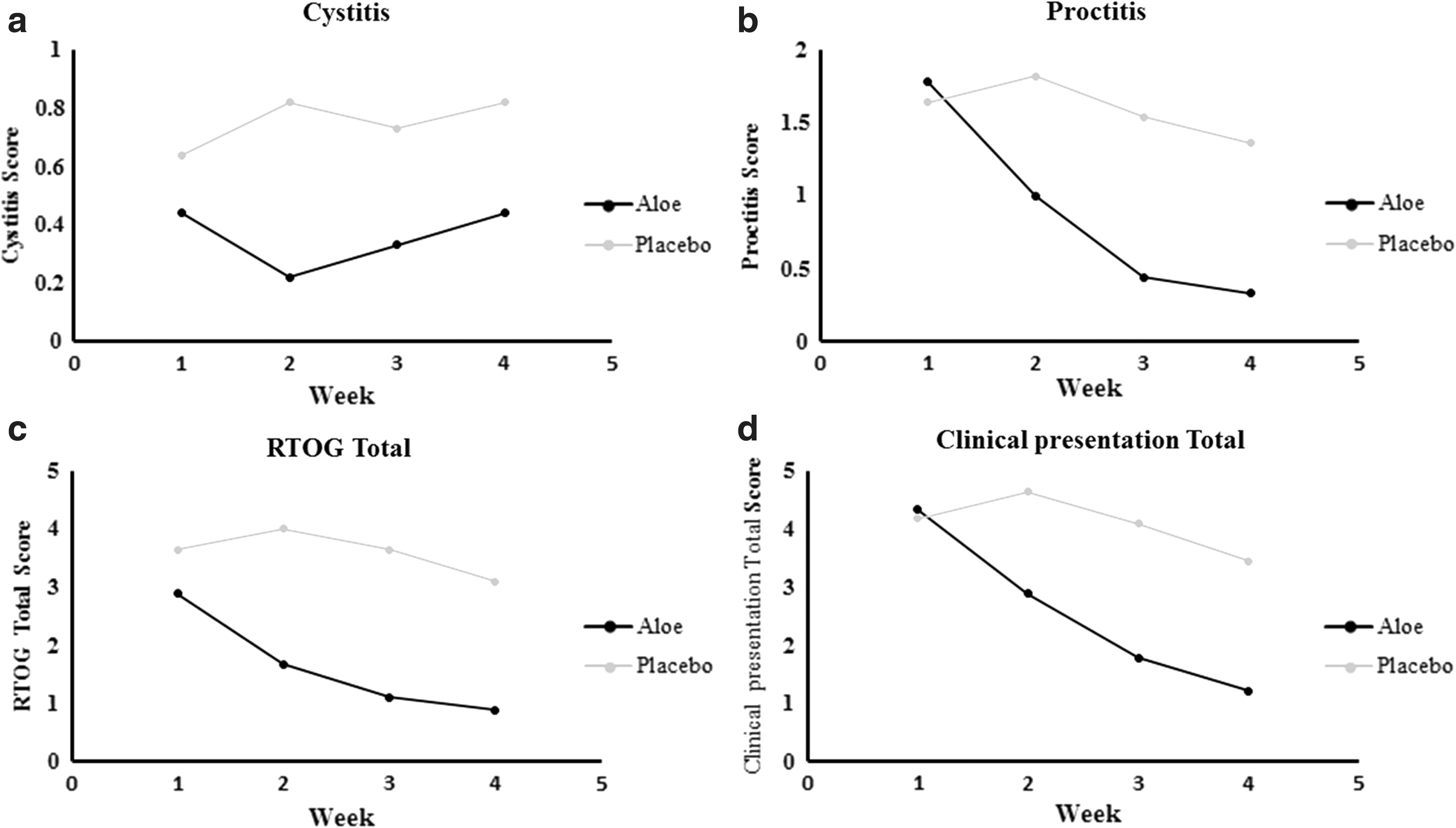
All patients treated with Aloe vera became symptom free or improved greatly as clinical presentation score total decreased from 4.3 (standard error of the mean [SEM]: 2.2) at baseline to 1.2 (SEM: 0.8) at week 4 of treatment. In the placebo group, the overall score value remained almost unchanged (clinical presentation score total changed from 4.2 [SEM: 1.2] at baseline to 3.5 [SEM: 1.1] at week 4). The RTOG score of patients in the Aloe group followed a decline trend (score from 2.89 [SEM: 2.1] to 0.89 [SEM: 1.0]) within the treatment period. None of the symptoms increased during the 4 weeks of follow-up in the Aloe group. The differences between the mean in the two groups were statistically significant for both clinical presentation score total (p = 0.0087) and RTOG total (p = 0.0016).
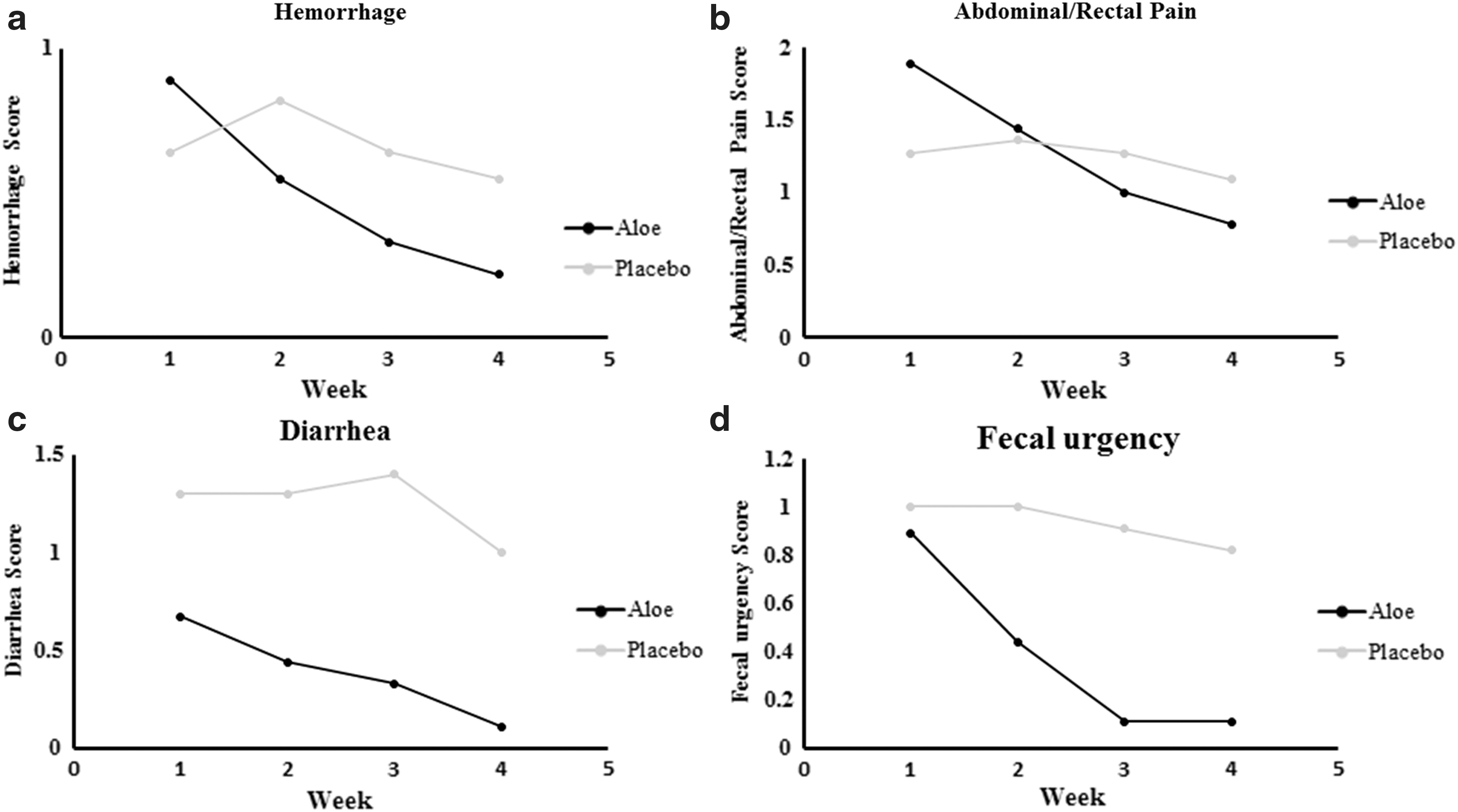
With the exception of hemorrhage and abdominal/rectal pain (which did not achieve statistical significance, but still favored the Aloe group), all measures of clinical presentation toxicity were better by treatment with Aloe. The toxicity prevented most effectively was diarrhea (p = 0.008) (Table 5). Figures 2 and 3 show the outcomes by applying the Aloe or placebo ointments over the 4 weeks of the study.
Hemorrhage trend of changes during 4 weeks of follow-up
Cystitis trend of changes during 4 weeks of follow-up
RTOG, Radiation Therapy Oncology Group.
The advantages of Aloe over placebo were statistically marked, especially for clinical presentation total and RTOG total with the odds ratios of 3.97 and 5.9, respectively (Table 6).
Data refer to the first 4 weeks of treatment.
CI, confidence interval; OR, odds ratio.
Compliance was good as assessed by comparing the actual and estimated volumes of residual ointment. The Aloe vera ointment was generally well tolerated, and no adverse effects were experienced by any patient in either group.
Hemorrhage and abdominal/rectal pain trend
As shown in Table 5, there was a statistically significant time effect (within-subject differences), indicating that when the two groups were combined, the average hemorrhage and abdominal/rectal pain at baseline was higher than the average after starting the treatment (p = 0.007 and 0.0001, respectively). Furthermore, the trend of changes between groups (between-subject differences or group effects) was also significant (p = 0.044 and 0.005, respectively). But, there was no significant group-by-time interaction effect (p = 0.56 and 0.93, respectively) (Fig. 2).
Diarrhea and fecal urgency trend
Table 5 displays that there were no statistically significant between-subject differences, or group effects (p = 0.56 and 0.147, respectively) for diarrhea and fecal urgency. However, both time effects (p = 0.04 and 0.014, respectively) and group-by-time interaction effects were statistically significant (p = 0.008 and 0.027, respectively).
The average scores of diarrhea in the Aloe group significantly decreased from 0.67 ± 0.9 to 0.11 ± 0.3 over the 4 weeks of the study, and an almost complete cessation of rectal bleeding was observed at the end of week 4. In the placebo group, it remained unchanged, from 1.3 ± 0.8 at week 1 to 1 ± 0.8 at the end of week 4.
The average scores of fecal urgency followed a downward trend during the study, decreasing from 0.89 ± 0.8 in week 1 to 0.11 ± 0.3 at the end of week 4. However, that of the placebo group was again almost unchanged (Fig. 2).
Proctitis and cystitis trend
As illustrated in Table 5, there was a statistically significant time effect (p = 0.00009), indicating that when the two groups were combined, the average proctitis at baseline was higher than the average after the treatment. The trends of changes between groups were also statistically significant (p = 0.0058). Nevertheless, group-by-time interaction effects were not significant (p = 0.094) (Fig. 3).
In terms of cystitis, there were no statistically significant time effects (p = 0.704), group effects (p = 0.308), or group-by-time interaction effects (p = 0.15) (Table 5 and Fig. 3).
Clinical presentation total and RTOG total trend
As demonstrated in Table 5, the average clinical presentation total and RTOG total in the Aloe group were lower than the placebo group after initiating therapy with rectal ointment. The average scores of total clinical manifestations and RTOG total over time significantly decreased by 3.11 ± 1.42 and 2.0 ± 1, respectively, over the 4 weeks of treatment. Again, the trend of changes almost remained unchanged for the placebo group (Fig. 3).
Secondary endpoints
Lifestyle was affected in 14 out of 20 (70%) patients at baseline, and they had multiple symptoms that interfered with their daily lives. The median lifestyle score improved significantly after the treatment with Aloe vera, ranging from 1.1 (SEM: 1.1) to 0.33 (SEM: 0.5). In the placebo group, the overall score value remained almost unchanged (1.8 [SEM: 0.8] to 1.4 [SEM: 0.8]; p = 0.004).
However, treatment with Aloe vera did not influence the psychosocial status of the patients, as there was no statistically significant difference between HAD Scale during the treatment period (p = 0.14 for depression and p = 0.52 for anxiety).
Discussion
This preliminary double-blind placebo-controlled, clinical trial shows very encouraging early results, indicating that topical Aloe vera 3% at a dose of 1 g/day is effective in ARP. Overall subjective clinical scores improved as determined by the clinical presentation and RTOG scores, with subscore analysis showing most improvement in the severity and frequency of fecal urgency and diarrhea, which were significantly reduced in the Aloe group compared with the placebo. Fewer incidences of adverse effects of radiotherapy obviously enhance the QOL of the patients during therapy, as the patients in Aloe group experienced an improved QOL.
In this study, treatment with the safe and widely available medical plant, Aloe vera, appeared to ameliorate the symptoms of diarrhea, fecal urgency and also to significantly improve the patients' lifestyle. This traditional folklore medicine implements its effectiveness in treating wounds and burns and in reducing inflammation through inhibition of cyclooxygenase and scavenging reactive oxygen metabolites. 17,21,22
No proven effective pharmacotherapy is, at present, available for ARP. However, the traditional approach to the treatment of ARP has been directed toward decreasing the inflammation observed in irradiated rectal tissue with the use of anti-inflammatory agents such as amino salicylic acid derivatives, 23,24 and corticosteroids. 4,24,25 Some other agents, including mesalamine, pentoxifylline, 26 metronidazole, 27 butyrate, 18 and sucralfate, 28 have been applied as well. Also, a variety of approaches such as short-chain fatty acid enemas, 10 rectal instillations of formalin, 8,9 endoscopic (laser) therapy, 7 hyperbaric oxygen, 6 and Argon plasma coagulation 29 have been tried in a limited number of patients. But the responses to such treatment have been disappointing in some cases or have been complicated with ulcerations created in ischemic tissue that may take months to heal. Therefore, the optimal method of safe and effective therapy remains unclear.
Our findings demonstrate a step toward the treatment of radiation-induced proctitis targeting the possible pathophysiology of injury. Although the exact mechanism of action is not clearly recognized, reactive oxygen species may be formed as the direct effect of the radiation itself or the subsequent ischemia induced by the radiation. 11 Previous studies suggested a beneficial role for antioxidants in radiation proctitis. 30 Therefore, Aloe vera, with antioxidant and anti-inflammatory properties, enhances healing of mucosal lesions and reduces related symptoms. So, it is beneficial in the underlying mechanism of action of the damage to irradiated rectal tissue.
Study limitations
The major limitation of the study is the small number of patients. Although the results of this preliminary study are very promising, and it was performed in a randomized controlled prospective manner with predefined endpoints, these findings need to be confirmed in a larger group of patients with ARP. It should be noted that Aloe vera has not been applied in the treatment of radiation proctitis earlier and we aimed at having a primary evaluation of the tolerability and response of ARP to Aloe vera for the first time. Furthermore, the optimal period of treatment with Aloe vera ointment for a successful treatment outcome of ARP remains unknown as this is the first preliminary clinical trial of treatment with Aloe vera and seeks further studies. Finally, when considering the mechanisms of action by which Aloe yields its efficacy, rectosigmoidoscopic assessment would be advantageous. However, any mechanical intervention during the acute phase should be avoided as it could worsen the condition, due to the risk of irreversible damage to the internal sphincter and the resultant incontinence and infection. 31 Therefore, we did not find it ethical for the first clinical trial of this herbal medicine.
Conclusion
In summary, the data of this study support that Aloe vera ointment is a safe and effective therapy for ARP. Aloe vera improves the symptoms of proctitis, including diarrhea and fecal urgency scores, and also enhances the QOL of patients without any significant adverse event.
Footnotes
Acknowledgments
The authors gratefully acknowledge the vice chancellor of Research and Technology Affairs of Mazandaran University of Medical Sciences for financial support. The results of this trial are a part of a postgraduate thesis (A.S.).
Author Disclosure Statement
No competing financial interests exist.