
Abstract
Aims and Objective:
The aim of this study was to evaluate and compare the effect of chlorhexidine (CHX) chip and turmeric chip as a local drug delivery (LDD) agent in the treatment of patients with chronic periodontitis.
Materials and Methods:
A total of 120 sites with pocket depths 5–8 mm were chosen as a split mouth design at 3 sites in the same patient. Selected sites were randomly divided into three groups to receive CHX chip in addition to scaling and root planing (SRP) in group A, turmeric chip in addition to SRP in group B, and SRP only in group C. Clinical parameters, that is, plaque index (PI), gingival index (GI), probing pocket depth (PPD), and relative attachment level (RAL) were recorded at baseline, 1 month, and 3 months interval.
Result:
On applying statistical analysis, results revealed that there was a significant reduction in all the clinical parameters, that is, PI, GI, PPD, and gain in RAL from baseline to 1 month and 3 months in all the three groups. These results were found to be significantly high in the CHX group and turmeric group than in the SRP group. Also, the results in both the test groups were maintained till the end of the study periods, but SRP group showed a significant deterioration after 1 month as was seen by increase in PPD and decrease in RAL scores after 3 months in the SRP group.
Conclusion:
Both the treatment modalities with the application of LDD as an adjunct to SRP proved to be equally beneficial in the treatment of chronic periodontitis.
Introduction
P
Surgical procedures have inherent disadvantages such as greater patient morbidity, marginal bone resorption, and compromised postsurgical aesthetics in the form of gingival recession and interproximal soft tissue cratering. 4 Further there are certain individuals in whom surgery is contraindicated such as medically compromised patients, uncooperative individuals, elderly patients, and persons with physical or mental handicaps. 5
Earlier, a greater emphasis was laid on the microbiologic etiology of periodontal disease. The microbial ecology of human periodontitis suggests therapies with antimicrobial agents in addition to mechanical therapy. Goodson in 1979 first proposed the concept of controlled delivery in the treatment of periodontitis. It has been observed that the local route of drug delivery can attain 100-fold higher concentrations of an antimicrobial agent in subgingival sites than a systemic drug regimen. 6
Various antimicrobial agents such as tetracycline, 10% doxycycline, 2% minocycline, metronidazole, and chlorhexidine (CHX) gluconate have been used and investigated as local drug delivery (LDD) in the treatment of periodontal disease. 7
Although local agents are beneficial as adjunct in the treatment of periodontal diseases, some side-effects with their usage have been mentioned in the literature such as placement of tetracycline-containing fibers around 12 or more teeth resulting in oral candidiasis in few patients. 7 Also because of its high cost factor, usage of these LDD agents in routine clinical practice may be restricted. To overcome these disadvantages, research is being conducted on the use of natural products as LDD agents. With the growing interest and increasing knowledge about the medicinal value of natural products, various formulations have been made commercially available. Herbal formulations such as turmeric, aloe vera, neem, tulsi, cocoa husk, and pomegranate are tested widely these days. 8 These products not only have long era of use and better patient tolerance but also act as a renewable source and are cost-effective.
Turmeric (haldi) is a rhizome of Curcuma longa. It has proven properties such as anti-inflammatory, antioxidant, antimicrobial, hepatoprotective, immunostimulant, antiseptic, antimutagenic, and also accelerates wound healing. 9 This natural product is easily available, cost-effective, and can be used as a LDD agent to treat patients with chronic periodontitis effectively. 10 Literature search reveals very few studies performed using turmeric as a LDD agent. Therefore, it adds up to the ongoing research related to herbal products in LDD.
The agent that has shown the most positive antibacterial results to date with pronounced antiseptic properties is CHX, 7 and is considered as “gold standard” in periodontics. Hence the aim of this study was to evaluate the efficacy of turmeric as an LDD agent in the form of chip as compared with only SRP and to compare the efficacy of this herbal chip as an LDD agent with the CHX chip in the treatment of chronic periodontitits.
Materials and Methods
Materials
CHX chip used in this study (PerioCol-CG) is a small, orange-brown rectangular chip manufactured by Eucare Pharmaceuticals, Chennai, India. The size of the chip is 4 × 5 mm with a thickness of 0.25–0.32 mm and weighing 10 mg. Each chip contains 2.5 mg of CHX in a biodegradable matrix of fibrilar collagen.
The test product turmeric chip used in the study measures 4 × 5 mm with a thickness of 0.4 mm and weighing 10 mg in a biodegradable 1000 mg hydroxy propyl cellulose matrix with 5% turmeric by weight.
Method
A total of 120 sites in 40 patients aged 30–50 years (each comprising 3 test sites with probing pocket depth [PPD] 5–8 mm) with mild-to-moderate chronic localized periodontitis (when <30% of the sites assessed in the mouth demonstrate attachment loss and bone loss) were selected from the outpatient department of periodontics, Modern Dental College, Indore. The study protocol was approved by the institutional ethical committee. The patients were duly informed about the study and written consent was obtained for their participation in the study. PPD was measured using a graduated probe (UNC-15) by inserting the probe into the gingival sulcus and readings were taken from the gingival margin till the base of the pocket. Alginate impressions were made to prepare customized acrylic stents that would act as a reference guide for recording PPD and relative attachment levels (RALs) at the experimental sites (as explained in flowchart).
Exclusion criteria included pregnant and lactating females, patients with a history of any kind of periodontal therapy within past 6 months, medically compromised patients, sites neighboring recent extraction sites, teeth showing endoperio lesions, restorations and other plaque retentive factors, smokers and tobacco chewers, and, importantly, subjects not compliant with oral hygiene procedures.
Study design
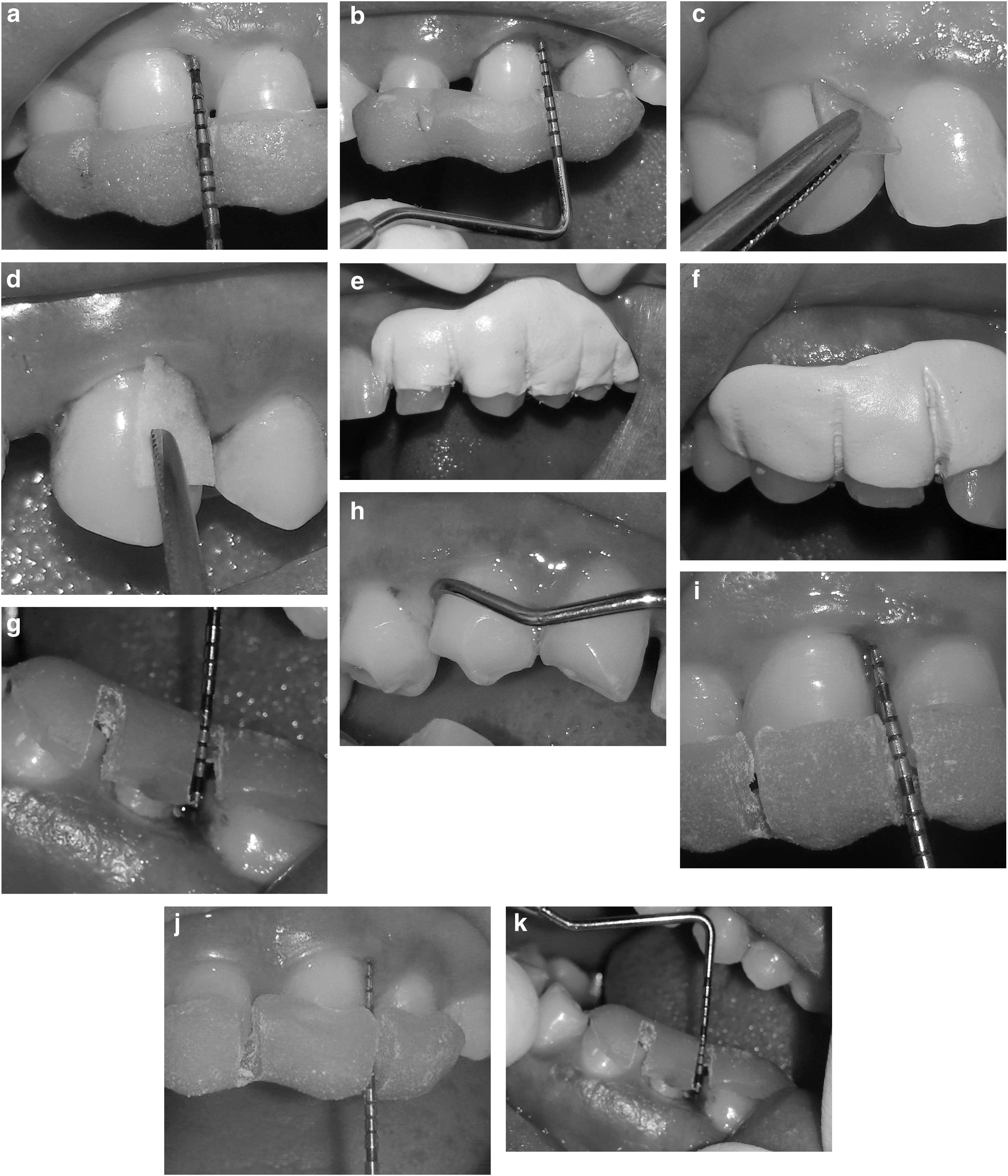
A flowchart indicating chronological order of procedures performed during the study period is shown in Figure 1. For each patient, three contralateral target sites were selected using simple randomization procedure and assigned to one of the three treatment modalities as follows:

Study design.
Group A: Sites to be treated with CHX gluconate chip (Periocol-CG) in addition to SRP (Fig. 2a, c, e, i).
Group B: Sites to be treated with turmeric chip in addition to SRP (Fig 2b, d, f, j).
Group C: Sites to be treated with only SRP (Fig 2g, h, k).
Randomization was done using predetermined computer-generated randomization scheme to receive balanced random allocation of patients. Each randomization number was randomly assigned to the three treatments—CHX chip, turmeric chip, and SRP alone. One set of envelope was provided to the investigator containing individual randomization codes. The randomized allocation sequence was generated by a statistician.
Statistical analysis
Mean and standard deviations of plaque index (PI), gingival index (GI), PPD, and RAL were calculated for each group. Mauchly's test of sphericity was applied to check whether there was a violation of assumption of sphericity. All significant values in Mauchly's test were subjected to Greenhouse–Geisser corrections and p-values were calculated. Being a split mouth design, intragroup comparisons were analyzed by repeated measures analysis of variance (ANOVA). Bonferroni test was used for post hoc comparisons after the repeated measures ANOVA. Analysis of covariance (ANCOVA) test was applied for intergroup comparisons at 1 month and 3 months adjusting for the baseline score variations as the covariate (adjusted analysis). Both adjusted and unadjusted values are presented in the results. Probability value of <0.001 was considered as statistically significant for all comparisons.
Results
A total of 40 subjects were recruited for this study. The mean age was found to be 34 years. Of these 40 subjects, 18 (45%) were females and 22 (55%) were males.
Intragroup changes at baseline, 1 month and 3 months for mean PI and GI for group A (CHX group) are shown in Table 1 and Intragroup changes at baseline, 1 and 3 months for mean PPD and RAL for group A (CHX group) are shown in Table 2.
ANOVA and post hoc Bonferroni test.
ANOVA, analysis of variance; GI, gingival index; PI, plaque index; SD, standard deviation.
ANOVA and post hoc Bonferroni test.
PPD, probing pocket depth; RAL, relative attachment level.
Intragroup changes at baseline, 1 month and 3 months for mean PI and GI for group B (Turmeric group) are shown in Table 3 and Intragroup changes at baseline, 1 month and 3 months for mean PPD and RAL for group B (Turmeric group) are shown in Table 4.
ANOVA and post hoc Bonferroni test.
ANOVA and post hoc Bonferroni test.
The mean PI and GI and the mean PPD and RAL displayed a statistically significant reduction in scores at 1 month and 3 months compared to baseline interval for both the groups (p < 0.001).
Intragroup changes at baseline, 1 month, and 3 months for mean PI and GI for group C (SRP group) are shown in Table 5. The mean PI and GI displayed a statistically significant reduction in scores when compared from baseline to 1 month and 3 months (p < 0.001).
ANOVA and post hoc Bonferroni test.
Intragroup changes at baseline, 1 month, and 3 months for mean PPD and RAL for group C (SRP group) are shown in Table 6. The mean PPD and RAL displayed a reduction in scores at 1 month and 3 months interval. The values were statistically significant (p < 0.001) when compared from baseline to 1 month for both PPD and RAL. There was statistically significant increase in PPD scores and RAL scores from 1 month to 3 months in the SRP group.
ANOVA and post hoc Bonferroni test.
Intergroup changes at baseline, 1 month, and 3 months for mean PI and GI between group A (CHX), group B (turmeric), and group C (SRP) are shown in Figure 3.
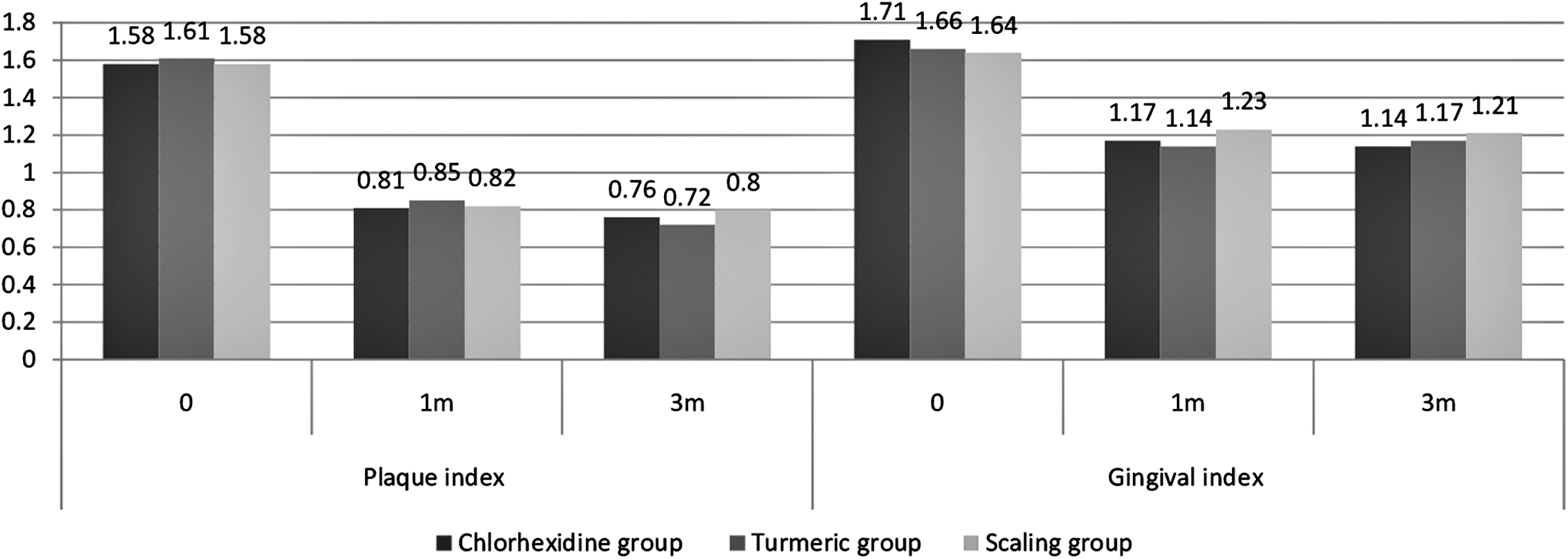
Graph showing intragroup comparison of plaque index and gingival index from baseline to 3 months.
Intergroup changes at baseline, 1 month, and 3 months for mean PPD and RAL between group A (CHX), group B (turmeric), and group C (SRP) are shown in Figure 4.
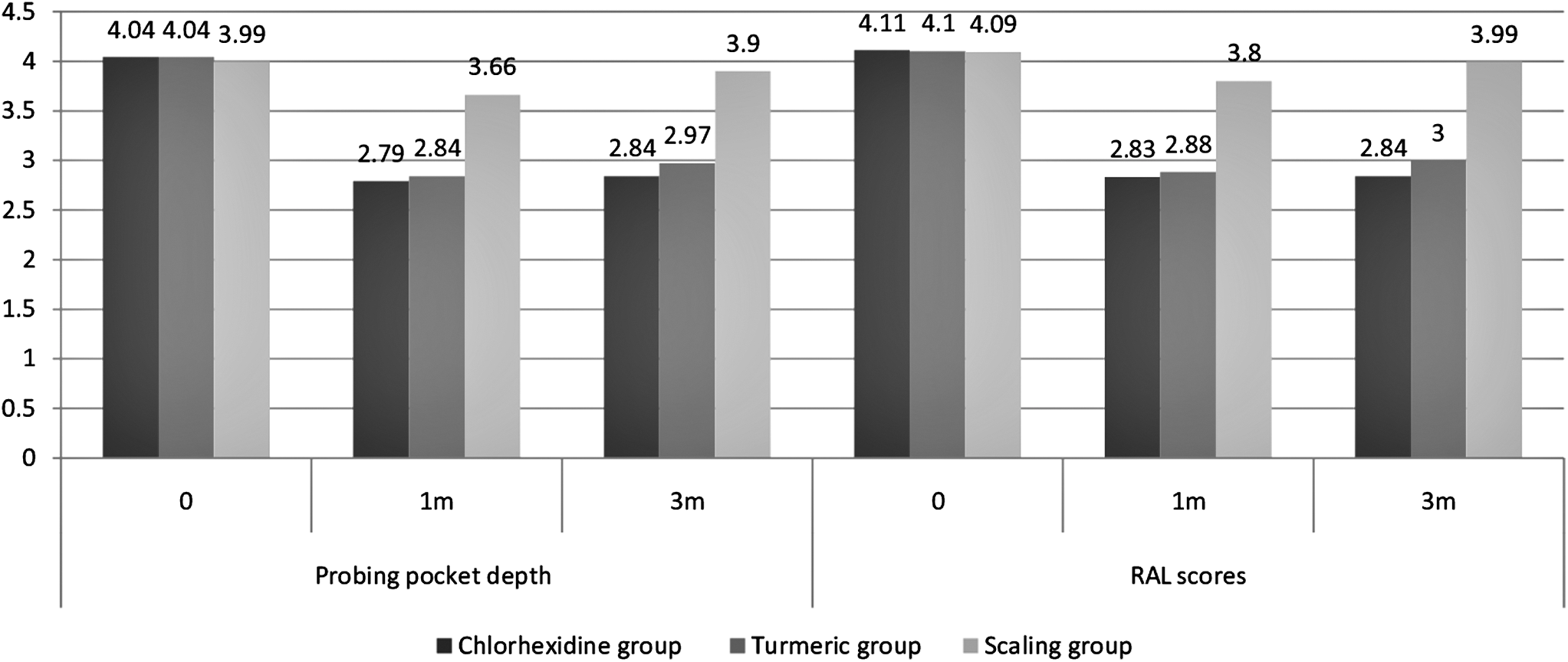
Graph showing intergroup comparison of PPD and relative attachment level from baseline to 3 months.
The PI, GI, PPD, and RAL scores for group A (CHX), group B (turmeric), and group C (SRP) were compared using ANOVA and ANCOVA to elicit any intergroup changes at baseline, 1 month, and 3 months interval. On applying ANOVA for overall comparison of three groups, there was no significant difference between the baseline scores when compared between the three groups.
After 1 month and 3 months interval, the PI and GI scores displayed no significant difference between the three groups. After 1 month interval and 3 months interval, the three groups significantly differed in PPD and RAL scores when adjusted for baseline values by ANCOVA. When further compared by post hoc Bonferroni tests, SRP group showed statistically significant (p < 0.001) higher PPD and RAL scores than the other two groups. There was no significant difference between CHX and turmeric groups.
Discussion
The present split mouth randomized controlled clinical trial evaluated two drug forms, that is, CHX and turmeric, both in the form of chip as a LDD over SRP alone in chronic periodontitis patients for a period up to 3 months. Split mouth design eliminates interpatient systemic differences (e.g., age, systemic health, and gender) that are known to confound the effects of periodontal treatment (independent variable) on clinical parameters and bacterial counts (dependent variables). 11 Also, maintaining the same oral environment for the experimental and control sites provides similar bacterial load, salivary pH, hygiene maintenance, etc. so that the effects of the drugs to be evaluated can be determined. Furthermore, to avoid “carry across” or “spillover” effects while comparing the effects of different drugs within the same dentition in a split mouth design, randomly selected sites were chosen from different quadrants. Hence only one tooth in each quadrant was chosen for the study. 12 To maintain drug uniformity in both the groups, the concentration of turmeric chip was formulated to be 5%, which was equal to 2.5 mg of CHX present in commercially available PerioCol CG chip.
Evaluation of SRP + LDD versus only SRP on the changes in PI and GI scores
The PI and GI scores were significantly reduced in all the three groups (CHX, turmeric, and SRP) when compared from baseline up to 3 months. This reinforces the fact about the importance of a thorough mechanical debridement that can reduce the inflammation of the soft tissues as well as bring about low plaque scores provided the patient maintains a strict oral hygiene regimen.
A significant reduction in the PI and GI scores were noted from baseline to 3 months in all the three groups. This states that all the three treatment modalities were efficient in reducing microbial load (PI) and the degree of inflammation (GI), 13 but none of the treatment modalities superseded the other modalities with respect to PI and GI. The results were similar to those by Pai et al., 14 wherein the reduction in bleeding on probing (BOP) was similar in both the experimental and control groups tested. Kranti et al., 12 Grover et al., 15 Gill et al., 16 Paolantonio, 17 and Dinca et al. 18 also observed a similar trend in the reduction of GI scores between test and control sites. The findings of this study are in accordance with those of Azmak et al., who found a mean reduction in bleeding index score at 1 month and 3 months for both the combination group and the SRP alone group when compared with the baseline; however, at all periods of observations, a statistically nonsignificant correlation was observed in the bleeding scores between combination groups. 19
In a similar study by Gottumukkala et al., aimed at comparing CHX and curcumin (CU), the mean PI scores did not show any significant difference between both the test groups at any time interval. 20
Evaluation of SRP + LDD versus only SRP on the changes in PPD and RAL scores
Although SRP proved equally beneficial in reducing plaque and gingival inflammation when compared with CHX and turmeric, mechanical debridement alone may not prove very beneficial in sites displaying varying pocket depths and calls for additional therapy to either reduce or eliminate the pocket or cause gain in attachment levels. This was clearly evident in this study wherein the SRP group showed an improvement in the PPD and RAL scores only in the first 1 month after therapy, after which the probing depths and attachment loss significantly increased. It has also been demonstrated that the time spent on therapy, the number of sites that require instrumentation, and the experience of the clinician may influence the success of SRP. 21 Also, some microbiota simply cannot be mechanically eradicated as bacterial invasion in cementum, radicular dentin, and the surrounding periodontal tissues has been reported. 21 Furthermore, recolonization of pockets can occur as early as 60 days after SRP. 1,2,22 A probable explanation for the deteriorating PPD and RAL scores after 1 month could be attributed to the latter.
The benefits of adjunct therapy such as delivering drugs directly into the pocket in addition to SRP were observed in this study, wherein a significant reduction in PPD and gain in clinical attachment level were evident over a 3-month period. Thus in addition to the benefits of SRP, the effects of the drugs in the pocket placed were evident as reducing PPD scores or gain in RAL values, which was seen maximum in the first 1 month after placement of the drug in the pocket and later remained stable without further deterioration. This was similar to the previous studies by Pai et al., 14 Gottumukkala et al., 23 Nayyar et al., 24 Mizrak et al., 25 and Soskolne et al. 26
The three treatment modalities performed in this study were compared using ANOVA and ANCOVA to unearth the differences if any in their efficacy to reduce PPD or cause a gain in RAL. Accordingly, it was observed that there were significant differences between the groups tested after 1 month and 3 months. Both CHX and turmeric led to significant improvement in reducing pocket depths and gain in attachment levels as compared with only SRP up to the 3-month recall period. Reduction in PPD scores was seen in similar studies conducted by various authors, that is, Kranti et al., 12 Grover et al., 15 Paolantonio 17 Azmak et al., 19 Jaswal et al., 21 Soskolne et al., 26 Singh et al., 27 Suhag et al., 28 Behal et al., 29 Varghese et al., 30 Bhatia et al., 31 and Rodrigues et al. 32 In this study, the change was significant in the first month but not significant from 1 month to 3 months. This was similar to the results obtained by Pai et al., 14 Jeffcoat et al., 33 Heasman et al., 34 and Grisi et al. 35
Evaluation of CHX versus turmeric as LDD on clinical parameters
This study also aimed to compare the efficacy of CHX and turmeric chip on the clinical parameters examined. Both the drugs were equally effective not only in reducing plaque and gingival inflammation but also in reducing pocket depths and causing significant gain in attachment level as evident by the significant reduction in all the scores obtained.
This is in accordance with the study by Anitha et al. 36 who found an equivalent effect of CU gel when compared with the CHX gel for the treatment of localized chronic periodontitis at 30 days when compared with the baseline. Similarly, another study by Jaswal et al. 21 who evaluated and compared the clinical effects of 2% whole turmeric gel versus 1% CHX gel as an adjunct to mechanotherapy in the treatment of chronic periodontitis found that turmeric gel showed a comparable improvement in all the clinical parameters as CHX gel. This may be explained on the basis of comparable mechanism of actions of CHX and turmeric as explained in Table 7.
GC, gingival crevicular fluid; iNOS, inducible Nitric Oxide synthase; TGF-β1, transforming growth factor.
Adverse events and complications
In this study, no adverse events were seen after placement of either of the two chips. Most of the studies that used CHX or turmeric reported no adverse effects, except for a few studies such as by Kaner et al., 41 in which 50% of the patients reported discomfort, soreness of gingival tissues, and pain after the insertion of CHX chips. According to the authors, they noticed gingival swelling, redness, and gingival exudation, but the signs disappeared after 3–7 days without therapeutic intervention. 41
Conclusion
This study reveals the excellent clinical properties of turmeric and CHX when evaluated over a period of 3 months. Although CHX is considered as a gold standard agent, this study shows an equally effective agent that can bring about a significant change in inflamed gingival tissues and reduction in PPD as well as gain in attachment. Added to this, turmeric displays very few side-effects as compared with the varying side-effects produced by CHX. Also, the cost of CHX chip is substantially expensive as compared with that of turmeric chip. Hence, turmeric chip may show a promising result as an LDD agent in the treatment of periodontitis.
Footnotes
Acknowledgment
The authors thank Dr. Srinivasan SA, Professor and Head, Guru Nanak Institute of Pharmacy, Ibrahimpatnam, Hyderabad, who spent his valuable time in preparation of turmeric chip as a local drug delivery system. CTRI number-CTRI/2016/09/007280.
Author Disclosure Statement
No competing financial interests exist.