
Abstract
Objective:
Arthrocentesis and prolotherapy are nonsurgical treatments for temporomandibular joint (TMJ) diseases. This study aimed to evaluate the treatment of hypermobility, pain, and displacement of the TMJ by consecutively performing arthrocentesis and prolotherapy in the same session.
Materials and Methods:
In this study, 10 adults with disc displacement and painful, hypermobile TMJ were selected. Arthrocentesis and prolotherapy were consecutively performed using a 30% dextrose solution that was simultaneously injected into five areas: posterior disc attachment, superior joint space, superior and inferior capsular attachments, and stylomandibular ligament. Paired t-test, McNemar test, and chi-square test were used to assess the maximum mouth opening, clicking sounds, pain, and subluxation of the TMJ. Patients with rheumatoid arthritis and parafunctional habits such as teeth clenching and grinding and biting of the cheeks or any other objects and those who had undergone surgery were excluded from this study.
Results:
A total of 10 participants (36.20 ± 7.06 years old, 7 women and 3 men) received a single treatment session of combined arthrocentesis and prolotherapy at the same office visit. Subluxation frequency and pain significantly decreased after the first week of treatment (p < 0.05). Subluxation also decreased at the 3-month follow-up (p < 0.05). Clicking sound values did not significantly change at any of the follow-up time points. Maximum mouth opening values decreased at all follow-up time points compared to baseline (p < 0.05).
Conclusion:
A single session of combined arthrocentesis and prolotherapy to treat symptomatic TMJ safely and significantly improved the subluxation and pain after 1 week and subluxation after 3 months compared to baseline status. The maximum mouth opening significantly decreased at all follow-up time points. Future studies assessing multiple treatment sessions are warranted.
Introduction
T
TMJ hypermobilities can be treated with surgical or nonsurgical methods. Nonsurgical methods include limitation of mandibular movement and injection of botulinum toxin and sclerosing agents into the muscles and TMJ tissues, respectively. Surgical procedures include eminectomy, condylectomy, and lateral pterygoid myotomy. 3 –5 Furthermore, effects of prolotherapy on TMJ hypermobilities have been discussed in several publications. 1,3,6 –8
For over 60 years, tendons, ligaments, and joint diseases have been treated using proliferative injection therapy, also known as prolotherapy. 6 This technique, which has been used since 1937, has been reported to have a beneficial effect on pain and TMJ hypermobility. 9 Prolotherapy is a technique used to strengthen lax ligaments by injecting various types of sclerosing or proliferating solutions and is used to treat general chronic musculoskeletal pain. 1,10,11 Prolotherapy involves injecting a solution such as dextrose 1,3,10,12 ; combinations of dextrose, glycerin, and phenol 13 ; and rarely, psyllium seed oil 9 near the site with connective tissue dysfunction. The underlying mechanism of action is unclear, 10 and prolotherapy has been hypothesized to promote the release of growth factors by initiating both inflammatory and noninflammatory reactions. 3 Studies supporting this hypothesis have reported that some cell types directly exposed to dextrose show interesting growth patterns. 6
Arthrocentesis of the TMJ involves irrigation of the superior joint space and is used to treat acute closed lock. 14 Painful TMJ is associated with inflammatory mediator concentrations within the joint such as substance p. Lavage of the superior joint space reduces the inflammatory mediators. Therefore, arthrocentesis is also used to reduce pain. 15 –17 Furthermore, arthrocentesis promotes disc repair/repositioning in temporomandibular articular disorders. 18 In this study, repositioning of the disc was not assessed.
The treatment for pain and displacement of the TMJ accompanied by hypermobility can be long and tiring because of the involvement of the joints as well as the surrounding tissues and muscles, which must also be treated. Consecutively, performing arthrocentesis and prolotherapy may be an effective method to shorten the duration of treatment. Therefore, this study has been conducted.
Previous studies reported that both arthrocentesis and prolotherapy reduce pain. 6,15,19 However, arthrocentesis effectively relieves pain by reducing inflammation, whereas prolotherapy activates inflammation. In this study, arthrocentesis was initiated by performing a lavage of the proinflammatory mediators that cause pain and tissue degeneration in the maxillary joint space. Prolotherapy causes an inflammatory response but does not cause tissue destruction. Prolotherapy is believed to initiate a cellular-level “therapeutic trauma” by activating the healing cascade with connective tissue proliferation in the desired locations, such as TMJ ligaments. 1
This study aimed to treat patients with painful, hypermobile TMJ and disc displacement. Arthrocentesis was performed to reposition the articular disc and reduce pain. Prolotherapy was then consecutively performed to treat TMJ hypermobility in the same session. The effectiveness of this treatment was evaluated.
Materials and Methods
Context
In this study, the investigators designed a prospective, open-label, single-arm study involving patients with disc displacement and painful, hypermobile joints who presented to the Oral and Maxillofacial Surgery Department of the Dentistry Faculty of Ordu University from April 2016 to January 2017. Arthrocentesis and prolotherapy were consecutively performed in the same session. The follow-up period was 3 months. Pain values, maximum mouth opening, subluxation frequency, and click sounds were recorded after 1 week, 1 month, and 3 months. All patients underwent the same intervention.
This study was approved by the Research Ethics Committee of the Faculty of Medicine at Karadeniz Technical University, Trabzon, Turkey (24237859372).
Participants
Preprocedure data of the 10 adult patients were collected (Fig. 1). At baseline, joint pain and increased mouth opening were observed in all patients, frequent subluxations in five patients, and click sound in six patients (Table 1).

Patient flow diagram. n, number.
SD, standard deviation; TMJ, temporomandibular joint.
Arthrocentesis was performed first to relieve the patient's pain by removing the inflammatory mediators from the upper joint space and helping to reposition the disc. Prolotherapy was consecutively performed to treat TMJ hypermobility. The same procedure was performed in all patients with painful joints. The patients were followed up after 1 week, 1 month, and 3 months (Fig. 1).
The primary inclusion criteria of this study were patients experiencing painful and hypermobile TMJ. All patients had painful, chronic, and recurrent subluxation at right side of the TMJ. Patients with inflammatory connective tissue disease such as rheumatoid arthritis and/or parafunctional habits (clenching, teeth grinding, cheek biting, etc.) or those who had undergone surgery were excluded from this study. The TMJ hypermobility was diagnosed based on the patient's history and the clinically identified excessive abnormal excursion of the condyle that slides over the articular eminence. The radiographic observation of anterior positioning of the mandibular condyle to the articular eminence on wide opening confirmed the clinical diagnosis. Painful joints could be diagnosed and temporarily relieved by injecting a local anesthetic into the joint 20 ; therefore, this method was used to distinguish between muscle and joint pains.
Treatment technique
The nature of this study was explained to the patients, who provided informed consent to undergo arthrocentesis and prolotherapy. Arthrocentesis and prolotherapy injection protocols used in the present studies have been published. 1,8,19 First, a guideline was drawn from the canthus to the tragus (Fig. 2a). Povidone–iodine solution was used to disinfect the skin in the preauricular region. The ear was covered with a sponge to prevent the solution from coming in contact with the inner ear. After palpating the superior joint space, 2 mL of 4% articaine and 0.5% epinephrine was administered to this region (Fig. 2b). A 21-gauge needle was inserted into the superior joint space 10 mm anterior to the tragus and 5 mm inferior to the tragal–canthal line. A second 21-gauge needle was inserted into the same space 20 mm anterior to the tragus and 5 mm inferior to the line. For irrigation, 400 mL of lactated Ringer's solution was used (Fig. 2c). Then, 30% dextrose solution was injected into five areas: posterior disc attachment, superior joint space, superior and inferior capsular attachments, and stylomandibular ligament. Next, 1 mL of the prepared solution was injected into each area when the mouth was open (Fig. 3). The concentration of the dextrose solution to establish a prolonged effect was 30%. This procedure was performed after all conservative approaches failed to resolve the patient's symptoms.

Stages of arthrocentesis technique.
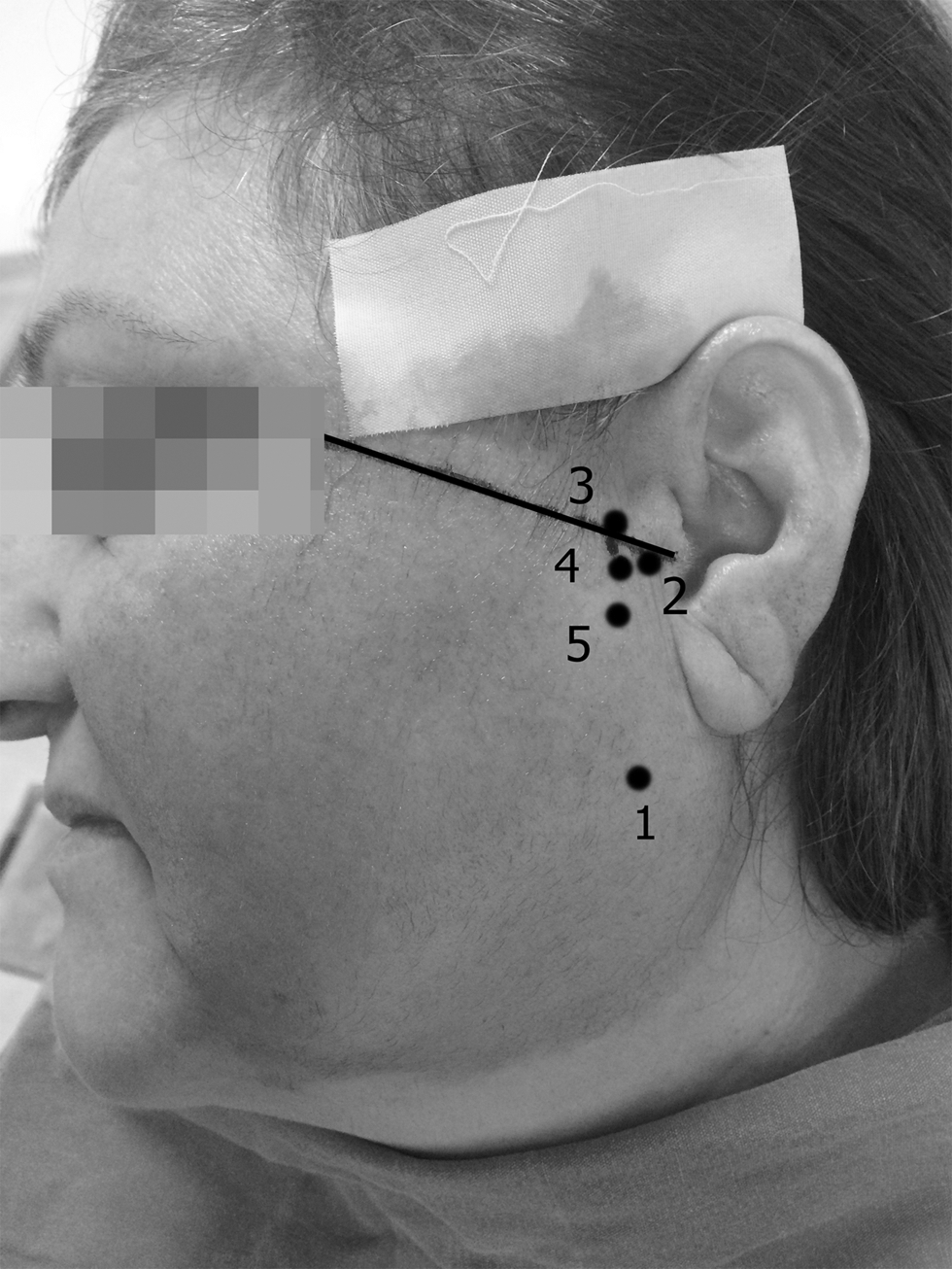
Injection points for prolotherapy. (1) Stylomandibular ligament; (2) posterior disc attachment; (3) superior capsular attachment; (4) superior joint space; (5) inferior capsular attachment.
Outcome measures
Table 1 was created to record and compare the outcome variables in four sessions: baseline, 1 week, 1 month, and 3 months. Pain intensity was classified under the following categories: “no pain,” “little pain,” “moderate pain,” and “severe pain” and consecutively scored from 0 to 3 for statistical analysis. The mouth opening distance (measured in millimeters using a ruler) was defined as the distance between the first right incisors. Subluxation frequencies were measured based on a scale from “1” (least frequent) to “6” (most frequent). Clicking sounds (diagnosed using a stethoscope) were recorded as “yes” or “no.” Statistical analysis was used to assess TMJ pain, maximum mouth opening, subluxation frequency, and click sound. The follow-up period was 3 months.
Assessment and analysis
Statistical Package for the Social Sciences version 20.0 (SPSS, Inc., Chicago, IL) was used for data analysis. Quantitative data are presented as means and standard deviations. Paired t-test and McNemar test were used to compare the maximum mouth opening and clicking sound values in the sample group, respectively. The chi-square test was used to analyze the differences in pain and subluxation frequency between the sessions. The level of significance was established at 5%.
Results
Ten patients who came to the clinic of the Oral and Maxillofacial Surgery Department, Faculty of Dentistry at the Ordu University and met the criteria were selected. The 10 selected patients (three men and seven women), ages 27–48, were a mean age of 36.20 ± 7.06 years. Table 1 shows the demographic data of the selected patients. All patients went through the same procedure. After lavage of the TMJ using Ringer's solution, 1 mL of 30% dextrose was consecutively injected into five areas of TMJ in all 10 patients. Table 1 shows the recorded data before and after the procedure.
Maximum mouth opening
Maximum mouth opening values were obtained by measuring the distance between the maxillary and mandibular incisors. After evaluating the descriptive analysis, maximum mouth opening values decreased during the 1-week follow-up in all patients. The mean maximum mouth opening values were 51.96 (±8.43) mm at baseline, 43.16 (±7.51) mm after 1 week, 46.08 (±6.18) mm after 1 month, and 46.72 (±6.07) mm after 3 months. The maximum mouth opening values between 1 week and 1 month increased in eight patients. After 3 months, the maximum mouth opening values were lower than the baseline in all patients (Table 1). The maximum mouth opening values are statistically and significantly lower between the baseline and after 1 week (p < 0.001), 1 month (p < 0.001), and 3 months (p < 0.005) (Table 2).
p < 0.05 reduction in maximum mouth opening was significant at all follow-up time points compared to baseline.
p < 0.05 reduction in pain was significant at first week compared to baseline (p = 0.033).
p < 0.05 reduction in subluxation frequency was significant at first week (p = 0.009) and third month (p = 0.032) compared to baseline.
SD, standard deviation.
Subluxation
Five patients reported subluxation at baseline and the frequency decreased and completely disappeared in all five and two patients, respectively (Table 1). The mean subluxation frequencies were 1.7 (±1.94) at baseline, 1.2 (±1.61) after 1 week, 0.7 (±1.33) after 1 month, and 0.6 (±1.26) after 3 months. Values of subluxation frequency significantly decreased between baseline and 1 week (p = 0.009) and between baseline and 3 months (p = 0.032) (Table 2).
TMJ pain
The pain of the TMJ decreased in six patients. However, it did not completely disappear in five patients (Table 1). The mean pain values were 1.9 (±0.56) at baseline, 1.0 (±0.66) after 1 week, 1.0 (±0.94) after 1 month, and 0.9 (±0.99) after 3 months. Between the baseline and 1 week, pain in the TMJ was significantly reduced (p = 0.033) (Table 2); however, between the baseline and 3 months, changes were not statistically significant (p = 0.179) (Table 2). At the end of the treatment, the pain returned.
Clicking sounds of the TMJ
Clicking sounds were observed at the baseline, which did not change in all patients at 1-week follow-up. At 1 and 3 months of follow-up, clicking sounds disappeared in two and three patients, respectively (Table 1). After 3 months, clicking sounds were only observed in three patients. Clicking sounds were not reported in the remaining four patients. Although decreased clicking sound values were statistically insignificant at all follow-up time points, clicking sounds disappeared in three patients at the end of treatment (Table 1).
Discussion
This study reports the first cases of patients with TMJ disorders treated with arthrocentesis and prolotherapy in a single therapeutic session. The primary findings are that pain, subluxation frequency, and mouth opening outcomes significantly improved after 1 week and that subluxation and maximum mouth opening improved throughout the follow-up to 3 months. Jaw clicking did not improve at any follow-up time points. These outcomes suggest a modest positive effect.
Arthrocentesis and prolotherapy were performed with the aim to reduce TMJ pain and dysfunction, including hypermobility. Another goal of this study is to complete the treatment within a short period of time. This approach was successful in the short term, however, whether outcome improvements would extend after 3 months or whether increased sample size would have reduced variability remains to be seen. Whether additional treatment sessions would improve the outcomes should also be determined.
The literature reports some studies that evaluated the effects of prolotherapy on osteoarthritis, 10,21 iliac joint disorders, 22 and wrist disorders 23 ; however, literature on the treatment of TMJ disorders is limited. As some authors reported that prolotherapy has only a placebo effect, 8 others also reported successful outcomes in treating osteoarthritis, 10 TMJ hypermobility, 1 subluxations, 3,19 joint pain, and clicking sounds. 6 Arthrocentesis has also been used to treat similar symptoms. 15 –18 As other studies have described both positive and negative findings, no one has yet combined these two therapies together in a single session and assessed outcomes.
Regarding the rationale of the procedures used in this study, pain in a hypermobile patient is often caused by stretching the retrodiscal tissues during mouth opening. In this study, pain was observed on palpation of the TMJ region, which is often a symptom for intra-articular inflammatory process. To date, studies show that pain and dysfunction are often refractory to care with a single treatment modality. Therefore, arthrocentesis and prolotherapy were consecutively performed to treat pain and disc dislocations and to reduce hypermobility in a single session.
In this study, treatment results of the patient group with pain, disc dislocation, and hypermobility symptoms were reported, but repositioning of the disc was not assessed. In hypermobility, patient's pain was often caused by stretching the retrodiscal tissues while opening the mouth. In this study, pain was observed on palpation of the TMJ region, which is often a symptom of intra-articular inflammatory process. Treating all these symptoms using one treatment modality was considered insufficient to knowledge. Therefore, arthrocentesis and prolotherapy were consecutively performed to treat pain and disc dislocations and to reduce hypermobility in a single session. Arthrocentesis was performed in the superior joint space to reduce the concentrations of proinflammatory mediators and pain mediators, as well as for disc repair/repositioning. Thereafter, prolotherapy was performed to cause reinflammation and strengthening of the tax ligaments. Many studies in the literature showed the efficacy of arthrocentesis to reduce pain up to 6 months. 24 –26 This study reports that combined application of arthrocentesis and prolotherapy significantly reduced joint pain at 1 week. Although the pain values were lower after 3 months, the results were statistically insignificant. The authors believe that the long-term result was caused by the presence of hypermobility. However, no similar studies show that these two methods were performed together and evaluated. The results of applying any single or multiple sessions with a large sample size remain unknown.
Results related to prolotherapy vary in the literature. Successful outcomes of different clinical symptoms are inconsistent among these studies. Klein et al. 13 and Ungor et al. 19 reported an insignificant decrease for maximum mouth opening in their studies. Furthermore, Kilic et al. 8 claimed that prolotherapy and placebo treatment have the same efficacy in treating any of the outcome variables of TMJ hypermobility. However, some studies reported improved clicking sound, 1,7,8, 12 pain, 7,8,10,20,22,27 maximum mouth opening, 1,8,22 subluxation frequency, 1,3,12,20 and dysfunction. 10,20,27 –29 Similar to some of these studies, 1,8,22 in this study, decreased maximum mouth opening values were statistically significant in all follow-up time points. According to Oh et al., 30 these findings could be explained based on the histologic findings. The TMJ treated with prolotherapy had progressive noninflammatory subsynovial connective tissue fibrosis, with vascular proliferation and thickening of collagen bundles in their study. 30 Similar histologic findings have also been reported by Yoshii et al. 31 They reported that tissue fibrosis stabilizes the joint and prevents the increase of mouth opening in a hypermobile joint. 31 However, pain reduction values were significant in most studies. 7,8,10,20,22,27 In this study, although pain levels were significantly reduced at the 1-week follow-up, no significant difference was observed at the 3-month follow-up compared to the baseline.
Recently, prolotherapy has been performed using different concentrations and with local anesthetics and has been described as generally effective. 3,6,10 Zhou et al. 3 reported that among 41 patients who had undergone rehabilitation, 26 (63%) required only a single injection. When examining the postprocedure results in patients who had undergone multiple procedures, a single procedure is preferable to ensure patient comfort. However, in this study, performing arthrocentesis and prolotherapy in the same session was regarded as a temporary treatment. The treatment should be performed in three to five sessions to obtain optimal efficacy. 3,19 If multiple sessions were performed in this study, treatment would have been permanent. Therefore, further research on this approach and its long-term success should be conducted.
The potential mechanism of action underlying prolotherapy may be related to the concentration of dextrose. 1 A wide range of dextrose concentrations (10%–25%) have been used to treat TMJ disorders. 1,6,19 Dextrose concentrations of >10% work partly by inflammation, 1,3,32 which initiates the biologic process of wound healing. After the injury, the granulocytes, monocytes, and macrophages migrate to the injured area. Growth factors are released and they activate fibroblasts, which produce matrix and new collagen fibrils. 33 Similar results may be observed when comparing the results of this study with those of other studies conducted using different dextrose concentrations. 1,3,6,10,12 Another study used 50% dextrose concentration, which was administered to a single site in the posterior periarticular tissues. 3 Multiple administrations were performed based on requirement.
In previous studies, different local anesthetics were used to treat TMJ disorders during prolotherapy. 1,3,19 These could block the auriculotemporal nerve and prevent the patient from feeling the pain during the procedure. Zhou et al. 3 used lignocaine as a local anesthetic agent and hypertonic glucose was injected to deal with the pain caused by joint dislocation. Lignocaine was effective in ∼5–10 min. However, the effect of articaine lasts longer; therefore, articaine was used as the local anesthetic in this study.
Study limitations
The primary limitations of this study were the small sample size and absence of a control group. Furthermore, dextrose concentrations reported in the literature vary widely. A 30% concentration was used, hoping to administer effective dextrose values. Moreover, treatment in only a single session may have caused the temporary results. Second, arthrocentesis is purported to remove inflammatory meditators; however, these were not measured in this study so whether they were present before the procedure or removed remains to be identified. Further studies are required to evaluate the effectiveness of this combined approach with wide sample sizes in single or multiple sessions.
Conclusion
Compared to the baseline status, a single session of combined arthrocentesis and prolotherapy for TMJ signs and symptoms resulted in safe and significant improvement in pain at 1 week, subluxation at 1 week and 3 months, and maximum mouth opening in all follow-up time points. These findings suggest the need for studies assessing this treatment regimen using multiple treatment sessions in a larger cohort with a longer follow-up time period.
Footnotes
Acknowledgments
No funds were used in completing this analysis. The views expressed in this study are only those of the authors.
Author Disclosure Statement
No competing financial interests exist.