
Abstract
Background:
More than 230 randomized controlled trials (RCTs) of danshen dripping pill (DSP) and isosorbide dinitrate (ISDN) in treating angina pectoris after the first preferred reporting items for systematic reviews and meta-analyses-compliant comprehensive meta-analysis were published in 2010. Other meta-analyses had flaws in study selection, statistical meta-analysis, and evidence assessment. This study completed the meta-analysis with an extensive assessment of the evidence.
Methods:
RCTs published from 1994 to 2016 on DSP and ISDN in treating angina pectoris for at least 4 weeks were included. The risk of bias (RoB) of included RCTs was assessed with the Cochrane's tool for assessing RoB. Meta-analyses based on a random-effects model were performed on two outcome measures: symptomatic (SYM) and electrocardiography (ECG) improvements. Subgroup analysis, sensitivity analysis, metaregression, and publication bias analysis were also conducted. The evidence strength was evaluated with the Grades of Recommendation, Assessment, Development, and Evaluation (GRADE) method.
Results:
Among the included 109 RCTs with 11,973 participants, 49 RCTs and 5042 participants were new (after 2010). The RoB of included RCTs was high in randomization and blinding. Overall effect sizes in odds ratios for DSP over ISDN were 2.94 (95% confidence interval [CI]: 2.53–3.41) on SYM (n = 108) and 2.37 (95% CI: 2.08–2.69) by ECG (n = 81) with significant heterogeneities (I2 = 41%, p < 0.0001 on SYM and I2 = 44%, p < 0.0001 on ECG). Subgroup, sensitivity, and metaregression analyses showed consistent results without publication bias. However, the evidence strength was low in GRADE.
Conclusion:
The efficacy of DSP was still better than ISDN in treating angina pectoris, but the confidence decreased due to high RoB and heterogeneities.
Introduction
A
In China, compound danshen (Salvia miltiorrhiza) dripping pill (DSP) is one of the most popular drugs approved (National Medicine Permit No. Z10950111) to treat coronary heart disease in 1995 by the State Food and Drug Administration. DSP was the first Chinese medicinal product listed in 1997 as an investigational new drug (IND No. 56956) by the U.S. Food and Drug Administration. In addition, it was the first Chinese proprietary medicine that completed a Phase II clinical trial (
The authors' previous meta-analysis
4
of 60 included randomized controlled trials (RCTs) published from 1994 to 2010 was the first preferred reporting items for systematic reviews and meta-analyses (PRISMA)-compliant
5
meta-analysis to compare the efficacy of DSP and isosorbide dinitrate (ISDN) in treating angina pectoris. ISDN is the most commonly used chemical antianginal drug and is often compared with Chinese herbal drugs. More than 200 of clinical trials of DSP and ISDN in treating angina pectoris have been published since year 2010. Moreover, eight meta-analyses
6
–13
have been published to assess the efficacy of DSP. The characteristics and inadequacy of previous meta-analyses are detailed in Supplementary Table S1 (Supplementary Data are available online at
Basically, there were three main flaws of previous meta-analyses as the following: (1) only a few (ranged from 11 to 28) RCTs were included; (2) inadequate statistical analyses, including the choice of fixed-effect model or random-effects model, sensitivity analyses, and subgroup analyses, were conducted to assess the efficacy; and (3) none applied the Grades of Recommendation, Assessment, Development, and Evaluation (GRADE) 14 method to assess the evidence from meta-analysis, while over 20 organizations, including the World Health Organization, BMJ Clinical Evidence, and the National Institute for Health and Clinical Excellence in the United Kingdom, have adopted the GRADE system. 15 Only one meta-analysis 13 was the updated study. One meta-analysis 6 did not assess the risk of bias (RoB) of included RCTs. Three meta-analyses 7,8,13 applied random-effects models for generalizable results. A recent qualitative systematic review 16 used the GRADE method to assess the overall quality of evidence without data analysis for the past (until year 2013) systematic reviews as limited (range “very low” to “moderate”).
These meta-analyses published between 2012 and 2015 are now outdated. Thus, a comprehensive meta-analysis, which includes the exhaustive searching for RCTs, the appropriate RoB assessment of included RCTs, the adequate conventional data analysis, and the complete evidence graded, is required to provide a better picture of the efficacy estimates from all eligible RCTs.
To evaluate the comparative efficacy of DSP in treating angina pectoris, the authors extensively updated the previous meta-analysis 17 and assessed the evidence with the GRADE method.
Methods
The present meta-analysis followed the authors' registered protocol (PROSPERO Registration No. CRD42016042748) 17 in accordance with the PRISMA 20095 for meta-analyses.
Data sources and searches
PubMed, Cochrane Library, ScienceDirect, EMbase, Blackwell (Interscience), Cambridge Journals Online, EBM reviews, China National Knowledge Infrastructure, WanFang Data, China Master Theses Full-text Database, Chinese Electronic Periodical Services, China Info, Social Sciences Citation Index, and China Doctor Dissertations Full-text Database were searched between the inception dates of databases and July 2016. Medical Subject Heading terms were used as search terms whenever available, or keywords were used wherever appropriate. Keywords included “danshen,” “salvia” (Latin name of danshen), “dripping pill,” “dropping pill,” “droplet pill,” and “diwai” (Chinese pinyin of dripping pill”). For instance, the search in PubMed using the keyword “danshen dripping pill” found 44 records, “danshen dropping pill” found 9 records, and “danshen droplet pill” found 1 record. The last search was performed on 12 July, 2016.
Eligibility criteria, study selection, and data extraction
Head-to-head RCTs that compared DSP and ISDN in treating angina pectoris with at least 4 weeks' follow-up period were included. Outcome measures included the symptomatic (SYM) and electrocardiography (ECG) improvements. 18 All database records were screened by both reviewers independently. Studies that did not meet eligibility criteria were excluded. Data were extracted from the included RCTs. Extracted data items included (1) outcome measures, (2) sample sizes, (3) follow-up periods, (4) dosages, (5) baseline characteristics of participants between groups, (6) years of publication, (7) number of authors, and (8) type of angina.
Statistical meta-analyses
A random-effects model
19
was selected for the assumption that all included RCT were sharing a normal distribution of effect sizes. Meta-analyses of RCTs were conducted to estimate the effect sizes on SYM and ECG improvement in terms of odds ratios (ORs)
20
and 95% confidence intervals (CIs).
21
Spearman correlation
22
between ORs of SYM and ECG was performed. The heterogeneity among studies was assessed by using Cochran Q test and estimated by using the I-squared (I
2
) statistic.
23
If the heterogeneity was high (e.g., 40%), the differences in efficacy and characteristics among included RCTs were explored by subgroup analyses,
24
sensitivity analyses,
25
and metaregression analyses
26
based on characteristics, such as RCT quality, sample size, follow-up period, publication year, and baseline comparable. Metaregression based on the mixed-effects model was conducted with the restricted maximum likelihood approach. The Mann–Whitney–Wilcoxon test
27
was used to compare two subgroups, and the Kruskal–Wallis test
28
was used to compare multiple subgroups. Trim-and-fill method for funnel plots,
29
Begg's test,
30
and Egger's test
31
were used to assess publication bias. The gray studies were searched in
RoB assessment and evidence grading
The RoB of included RCTs was assessed with the Cochrane Collaboration's tool for assessing RoB, 34 which included seven criteria. RCTs were rated as low RoB, at least four criteria were judged as low RoB. Otherwise, RCTs were rated as high RoB. The quality of evidence from meta-analysis was assessed with the GRADE method 15 in one of four grades, which were high, moderate, low, and very low.
Results
Characteristics of included RCTs
Database search identified 2517 citations and the process of citation is depicted in Supplementary Figure S1. According to the prespecified eligibility criteria, 4,17 109 head-to-head RCTs (References in the Supplementary Data) were included. The 109 RCTs with 11,973 participants were published in Chinese between years 1997 and 2016. The mean sample size was 109.8, and the median was 98. The follow-up periods were at least 4 weeks, in which 53 RCTs reported follow-up period for 4 weeks (or 30 days or 1 month) and 39 RCTs for 8 weeks (or 60 days or 2 months). The mean follow-up period was 44.6 days, and the median was 42 days. The dosage of DSP in 100 RCTs was 10 pills (27 mg/pill), three times daily. The daily dosage of ISDN in 79 RCTs was 30 mg. Eighty-three included RCTs used both SYM and ECG as outcome measures. Twenty-five RCTs used only SYM, and one RCT used only ECG as outcome measure. The characteristics of included RCTs are detailed in Supplementary Table S2.
RoB assessment
The RoB assessment of included RCTs was high with the Cochrane RoB tool (Fig. 1; Supplementary Table S3). A few RCTs had low RoB with random sequence generation (1 RCT), allocation concealment (25 RCTs), blinding of participants and personnel (7 RCTs), and blinding of outcome assessment (6 RCTs). Most RCTs had low RoB with incomplete outcome data (81 RCTs) and selective reporting (92 RCTs). Out of the total included RCTs, 19 RCTs were rated as low RoB, and other 90 RCTs were rated as high RoB according to prespecified criteria. The correlation of the RoB and published year was −0.12 (p = 0.1955), which indicated that the RoB of RCTs did not vary with time going. The correlation of the RoB and sample size in RCTs was 0.23 (p = 0.0154), which indicated that the RoB of RCTs improved with an increase in sample sizes.
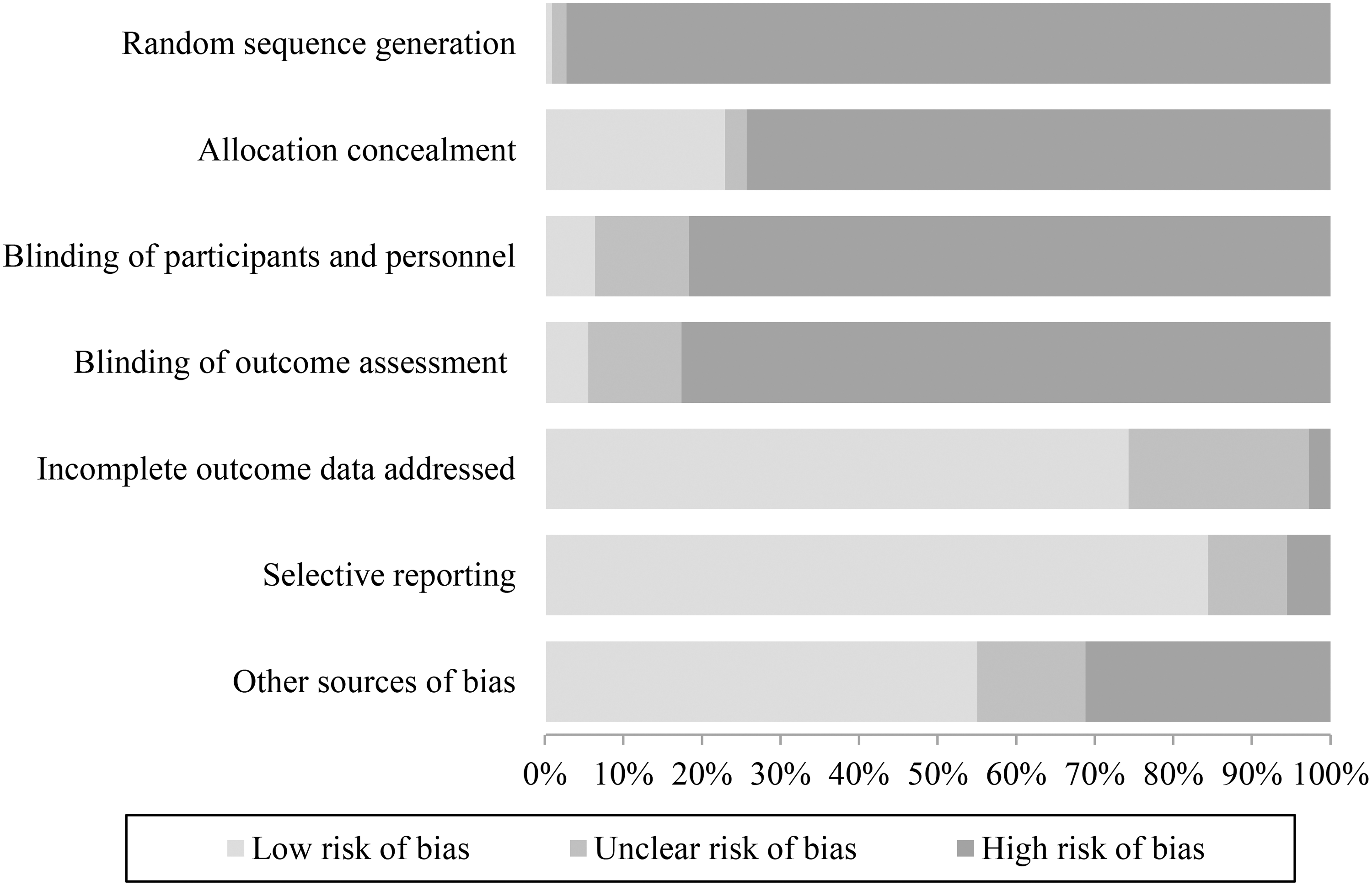
Risk of bias of included randomized controlled trials with the Cochrane risk of bias tool.
Comparative efficacy on outcome measures
One hundred and eight head-to-head RCTs that included 11,873 participants compared the efficacy on the SYM outcome. The overall OR of SYM was 2.94 (95% CI: 2.53–3.41, Z = 14.10, p < 0.0001) with a significant heterogeneity (Q = 180.81, I 2 = 41%, p < 0.0001, τ 2 = 0.2391), which is shown as Supplementary Figure S2. Eighty-one RCTs that included 9251 participants compared the efficacy on the ECG outcome. The overall OR of ECG was 2.37 (95% CI: 2.08–2.69, Z = 13.06, p < 0.0001) with a significant heterogeneity (Q = 148.42, I 2 = 44%, p < 0.0001, τ 2 = 0.1441), which is shown as Supplementary Figure S3. The SYM and ECG were moderately correlated (ρ = 0.55) with a high statistical significance (p < 0.00001), indicating that SYM and ECG findings corroborated with each other to provide positive evidence.
Sensitivity and subgroup analyses
Sensitivity and subgroup analyses were conducted according to RCT characteristics, including improvement criteria, follow-up periods, sample sizes, published years, RCT RoB, numbers of authors, adverse effects (AEs) report, trial date report, comparable baselines, DSP daily dosages, ISDN daily dosages, and treatments on both outcome measures SYM (Table 1) and ECG (Table 2). The efficacy of low RoB RCTs was slightly better than that of high RoB RCTs; however, the difference was not statistically significant (p = 0.8559 on SYM and p = 0.1876 on ECG). The overall results of subgroups remained efficacy for each OR more than 1.00. The difference of ORs from subgroups with different improvement criteria (p < 0.0001) and different published years (p = 0.0108) on the outcome SYM and subgroups with improvement criteria (p < 0.0001), different published years (p = 0.0122), and number of authors (p = 0.0399) on the outcome ECG were statistically significant. The difference of ORs from other subgroups was not statistically significant. Sensitivity and subgroup analyses indicated that the efficacy of DSP and ISDN was consistently stable. Twelve among all 74 subgroups were of low heterogeneity (I 2 < 30%, p > 0.05) when the heterogeneity in the overall effect size was statistically significant based on SYM (I 2 = 41%, p < 0.0001) and ECG (I 2 = 44%, p < 0.0001). The heterogeneity in subgroups of study publication year from 2010 to 2016 based on SYM (I 2 = 25%, p = 0.1040) and ECG (I 2 = 25%, p = 0.1127), subgroups of study with less than mean sample size based on SYM (I 2 = 26%, p = 0.06) and ECG (I 2 = 21%, p = 0.1059), and subgroups of study with low RoB based on SYM (I 2 = 29%, p = 0.11) was low without statistically significant. It seems that these characteristics, including sample sizes and publication years, may affect the study of heterogeneity.
AEs, adverse effects; CI, confidence interval; DSP, danshen dripping pill; ISDN, isosorbide dinitrate; OR, odds ratio; RoB, risk of bias.
Metaregression and publication bias analyses
The metaregression was performed between outcome measures and RCT characteristics (Table 3). There was no significant correlation between efficacy and characteristics except for characteristics of sample size on ECG (p = 0.0173) and publication year on both SYM (p = 0.0082) and ECG (p = 0.0447). All seven characteristics may be the sources of heterogeneity on outcome SYM, while six characteristics, except for RCT RoB, may be the sources of heterogeneity on outcome ECG. Both the Egger's test (SYM: t = 0.7266, p = 0.4691; ECG: t = −1.3006, p = 0.1972) and the Begg's test (SYM: Z = 0.1071, p = 0.1008; ECG: z = 0.098, p = 0.196) indicated no statistically significant publication biases. Funnel plot (Supplementary Fig. S4) from trim-and-fill method indicated 28 potential missing RCTs for SYM and 15 potential missing RCTs for ECG on the left side of the funnel plots. The overall OR on SYM was 2.16 (95% CI: 1.84–2.54; Z = 9.39; p < 0.0001) and heterogeneity was statistically significant (Q = 347.47, df = 135, I 2 = 60%, p < 0.0001) after trim-and-fill adjustment. The overall OR on SYM was 2.01 (95% CI: 1.75–2.30; Z = 10.05; p < 0.0001), and heterogeneity was statistically significant (Q = 254.59, df = 95, I 2 = 57%, p < 0.0001) after trim-and-fill adjustment. The results from trim-and-fill adjustment indicated that DSP was still more efficacy than ISDN.
ECG, electrocardiography; RCT, randomized controlled trial; SYM, symptomatic.
As the trim-and-fill method indicated potential missing RCTs,
Evidence grading
Initial evidence level was awarded as high (⊕⊕⊕⊕) because this meta-analysis was based on RCTs. The criteria of “likelihood of bias” were decreased to two levels () for the high RoB in blinding and allocation process. The criterion of “unexplained heterogeneity or inconsistency” was decreased to one level () for the high heterogeneity. Other criteria were not decreased or increased. The evidence from subgroups with high quality of RCT was graded as low (⊕⊕), while evidence from other subgroups was graded as low to very low. The evidence from this meta-analysis was graded as very low (⊕) on outcome measures SYM and ECG with the overall GRADE scores.
Discussion
Summary of updated findings
This is an updated meta-analysis on the efficacy of DSP and ISDN in treating angina pectoris that is based on 109 RCTs with 11,973 participants published between years 1997 and 2016. Overall, OR of SYM was 2.94 (95% CI: 2.53–3.41, p < 0.0001), and OR of ECG was 2.37 (95% CI: 2.08–2.69, p < 0.0001). Meta-analysis of head-to-head comparison showed that differences of DSP and ISDN in efficacy for the treatment of angina pectoris were statistically significant. Substantial differences in efficacy were found when little differences were seen in subgroup analyses, sensitivity analyses, and metaregression analyses. No statistically significant difference was found for publication bias with Egger's test and Begg's test. However, the RoB of included RCTs was high, especially in the domains of allocation concealment and blinding. The evidence from this meta-analysis on both outcome measures SYM and ECG was graded as low for the high RoB of included RCTs and high heterogeneities.
New findings over previous meta-analyses
A total of 49 new RCTs with 5042 participants comparing DSP and ISDN have been published since 2010. Previous systematic reviews except one 13 on DSP were not up-to-date. In this meta-analysis, additional methods, e.g., metaregression for explaining possible heterogeneity across included studies and trim-and-fill method for identifying publication bias, were used to test the consistency and robustness of the results. The Cochrane RoB tool for RCT RoB assessment and the GRADE method for meta-analysis evidence grading were also taken into account in the meta-analysis. The authors specifically conducted subgroup analysis and meta-regression between the RoB of RCTs and the efficacy measures, which indicated that the RoB did not affect efficacy estimates. Six characteristics, including sample size and follow-up period, may be the sources of heterogeneity on outcomes SYM and ECG. Furthermore, whenever possible, meta-analysis of head-to-head randomized placebo-controlled trials and network meta-analysis of DSP and other treatments with high quality would be performed to explore the relative efficacy.
Current issues of RCTs on DSP and ISDN
Nevertheless, there are some limitations in this updated meta-analysis. Heterogeneity of the included RCTs was similar to previous meta-analysis. 4 The heterogeneities of efficacy estimates were high and that could not be explained by the performed subgroup analyses and sensitivity analyses on RCTs characteristics. Metaregression found publication year and sample size correlating with heterogeneity. The efficacy was estimated on both outcome measures SYM and ECG. However, included RCTs seldom reported other outcome measures, such as quality of life, cardiovascular deaths, or adverse events.
Publication bias is a concern for all systematic reviews and has been empirically found to be problematic for RCTs of Chinese herbal medicines. 35,36 Selective availability of RCTs with positive results may seriously bias conclusion. 37 It was more likely that Chinese authors published studies, including systematic reviews, with positive results. 38,39 All included RCTs in this updated meta-analysis were published in Chinese journal by Chinese authors. Similarly, there were a small number of RCTs with negative results, in which the number was 6.48% (7/108) for the outcome SYM and 7.71% (6/81) for the outcome ECG. Although Egger's test, Begg's test, and trim-and-fill method did not find significant publication bias, stakeholders should interpret these positive findings more critically.
The high RoB of included RCTs was also similar with their previous meta-analysis. 4 In this study, the threshold for RCTs to be low RoB was that the RCTs must be evaluated to be at low risk in at least four out of seven domains, while only 1.76% (19/108) RCTs on SYM and 1.73% (14/81) RCTs were of high quality. If the threshold of low RoB studies was raised to having at least six out of seven domains to be at low risk, no RCT would be deemed low RoB.
ISDN was not the first choice in treating angina pectoris. Beta blockers or calcium channel blockers are the first-line treatment in treating angina pectoris for the balance of efficacy and safety. 1,2 DSP should be compared with the first-line antianginal drugs.
Meta-analysis on RoB assessment, efficacy estimates, and evidence grading
Conclusions from meta-analyses on the RCTs with high RoB should be drawn with reservations. 40 High RoB of included RCTs can weaken the conclusions. Two reviews demonstrated that clinical trials without the features such as blinding and allocation concealment tended to report a more exaggerated treatment effect than those trials included such features. 41,42 When subgroup analyses and metaregression analyses were performed based on RoB of RCTs, the differences of efficacy estimates were not statistically significant. Consolidated Standards of Reporting Trials (CONSORT) statement and checklist had been published in 2010, 43 which offered a standard way to improve the RoB of RCTs reports. The quality of items, including random sequence generation and allocation concealment, seems a little increasing while the quality of items on blinding seems decreasing after 2010 (Supplementary Fig. S5). For the other items, RCTs RoB published after 2010 and before 2010 remained poor. In short, RoB of RCTs on DSP had not improved since 2010.
When meta-analyses, including subgroup analysis, sensitivity analysis, metaregression analysis, and additional analysis, were conducted adequately, DSP was more efficacious than ISDN in treating angina pectoris, in agreement with most other meta-analyses. However, significant heterogeneities were found on both outcome measures SYM and ECG. Due to the high RoB of included RCTs and high heterogeneity, the evidence strength of this updated meta-analysis was deemed low to very low in accordance with the GRADE method. Overall, conclusions with strong evidence strength are only obtainable from the RCTs with low RoB, sufficient efficacy estimates, low heterogeneity, and insignificant publication bias. Thus, the conclusion should be drawn with comprehensive balance of these factors in meta-analysis.
Conclusion
The efficacy of DSP was still better than ISDN in treating angina pectoris, but the confidence was decreased due to high RoB and significant heterogeneities.
Footnotes
Acknowledgment
The work of both authors was supported by research grants (MYRG190-Y3-L3-ICMS11-LSW and MYRG2014-00117-ICMS-QRCM) from the University of Macau.
Authors' Contributions
Y.J. and S.L. designed and conducted this study, including search strategy, eligibility criteria, and meta-analysis. They also wrote, proofread, and approved all versions of the article.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.