
Abstract
Objectives:
We conducted a quality improvement project to determine (1) what information providers and patients most wanted to learn about complementary and integrative health (CIH) therapies and (2) in what format they wanted to receive this information. The overall aim was to develop educational materials to facilitate the CIH therapy decision-making processes.
Design:
We used mixed methods to iteratively pilot test and revise provider and patient educational materials on yoga and meditation. We conducted semistructured interviews with 11 medical providers and held seven focus groups and used feedback forms with 52 outpatients. We iteratively developed and tested three versions of both provider and patient materials. Activities were conducted at four Veterans Administration medical facilities (two large medical centers and two outpatient clinics).
Results:
Patients want educational materials with clearly stated basic information about: (1) what mindfulness and yoga are, (2) what a yoga/meditation class entails and how classes can be modified to suit different abilities, (3) key benefits to health and wellness, and (4) how to find classes at the hospital/clinic. Diverse media (videos, handouts, pocket guides) appealed to different Veterans. Videos should depict patients speaking to patients and demonstrating the CIH therapy. Written materials should be one to three pages with colors, and images and messages targeting a variety of patients. Providers wanted a concise (one-page) sheet in black and white font with no images listing the scientific evidence for CIH therapies from high-impact journals, organized by either type of CIH or health condition to use during patient encounters, and including practical information about how to refer patients.
Conclusions:
Providers and patients want to learn more about CIH therapies, but want the information in succinct, targeted formats. The information learned and materials developed in this study can be used by others to educate patients and providers on CIH therapies.
Introduction
A
Patients and medical providers often approach CIH therapies from diverse perspectives, knowledge, and experience with those therapies, making it potentially difficult for them to have shared decision-making conversations about CIH therapies as potential treatment options. Shared decision-making is a central component of patient-centered healthcare and describes the process of providers working together with informed patients to make shared, sustainable decisions about treatment. One key to facilitating this conversation is to provide educational materials targeting patients and providers. To develop effective education materials, it is the key to understand what salient information patients and providers want to know about CIH therapies and in what format they want to receive it.
We conducted a quality improvement project in the VA to establish what information about CIH therapies providers and patients most wanted to learn and in what format they wanted it, with the aim of developing materials to facilitate the CIH therapy decision-making processes. During this knowledge-gathering process, we iteratively created, evaluated, and revised patient and provider educational materials on yoga and meditation. The information learned and materials developed can serve as templates in future efforts to educate patients and providers on CIH therapies.
Materials and Methods
Overview
We conducted a quality improvement project using mixed methods to iteratively pilot test and revise existing or newly developed provider and patient educational materials on yoga and meditation. To pilot test the materials, we conducted (1) provider semistructured interviews and (2) outpatient focus groups with feedback forms. Activities were conducted at four West coast VA medical facilities (two large medical centers and two community-based outpatient clinics).
Materials
We focused on developing materials for yoga and meditation because they are among the most effective types of CIH for addressing common health conditions and were available at all four medical facilities (we did not include a broader range of types of CIH so as not to influence patient demand for unavailable CIH). To find existing materials and content to build new materials, we searched websites for the NIH's National Center for Complementary and Integrative Health (NCCIH), the VA's Office of Patient Centered Care and Cultural Transformation (OPCC&CT, the office guiding CIH operations and policy), and the VA's War Related Illness and Injury Study Centers (WRIISC, some VA centers that have been providing CIH therapies). For patient materials, we found videos and audio files 17 –20 and developed new handouts. For provider materials, we showed two pages from VA OPCC&CT educational materials, 21 abstracts to several randomized controlled trials and healthcare cost reduction studies published in top journals 1 –3,22,23 and visual depictions of reviews of systematic reviews of the scientific literature (or evidence maps) commissioned by the VA OPCC&CT. 5 –10
Patient materials feedback process
We conducted seven 1-h focus group sessions with 52 veteran outpatients to gather feedback on the patient materials. Subsequently, we either revised the materials or created new ones. We used existing patient groups or classes that either addressed health behaviors (e.g., diet and physical activity) or were patient advisory councils (groups of patients who advised the VA on research or operations). The patients appeared to range in age from their 20s to 80s, most were White, and about three quarters were male.
Each focus group had four phases in which patients: (1) completed a brief feedback form, (2) reviewed the materials, (3) completed a second feedback form, and (4) participated in discussions guided by the feedback forms. The first feedback form asked: (1) if they had tried meditation (or yoga), (2) if they were interested in learning about meditation (or yoga), and (3) what might make them want to try meditation (or yoga). The second form asked: (1) how easy was it for them to understand the information, (2) how likely were they to try meditation/yoga after looking at the materials, (3) what they liked/did not like about the materials, and (4) what about the materials did they think we should change.
Provider materials feedback process
We conducted 11 30-min, in-person, individual semistructured interviews with physicians from primary care and women's health clinics, hospitalists, and mental health providers. We iteratively gathered feedback from providers and subsequently revised the materials. In each interview we asked providers: (1) what they liked/did not like about the materials, (2) what they wanted us to change about the materials, and (3) after reading the materials, how influenced might they be to talk to their patients about yoga or meditation for pain and symptoms of anxiety and depression.
Data analysis
We used detailed, often verbatim notes from the interviews and focus groups to draft transcripts that were evaluated immediately after each interview/group using a method of constant comparison, in which any newly collected data are compared with previously collected data to elucidate common themes. 24 Our team qualitative methodologist free-coded all text and, with another team investigator, sorted it into emergent themes as interviews were conducted. We reached saturation 25 for both provider and patient themes at the third round of iteration, so stopped collecting data. Under each theme, we identified emergent actionable recommendations. Also, we aggregated the quantitative data from the feedback form responses into bar charts to examine patient CIH experiences and feedback on the educational materials.
Results
Two-thirds (62%) of patients (n = 52) reported having tried yoga or meditation in the past and, of those, few (15%) currently practiced yoga or meditation, but almost all (96%) were somewhat or very interested in learning more about them. Of the 38% who had not tried yoga or meditation, 82% were interested in learning about them.
As shown in Figure 1, when we asked patients how much the four informational vehicles we examined made them want to try yoga or meditation, before showing them the actual materials, the most influential factor for those having tried yoga/meditation was learning some scientific facts about how it might be effective for certain health conditions (28%), whereas the most influential factor among the uninitiated was watching a demonstration (32%) followed by learning some scientific facts. Hearing about yoga/meditation from their provider was the third most influential factor among both groups. We then presented three of the four informational vehicles (we did not show them a demonstration of yoga or meditation). Afterward, 94% of patients who had not already tried meditation or yoga were willing to try it and 93% of those who had tried yoga were likely to try it again either because of the materials or because they already practiced it.
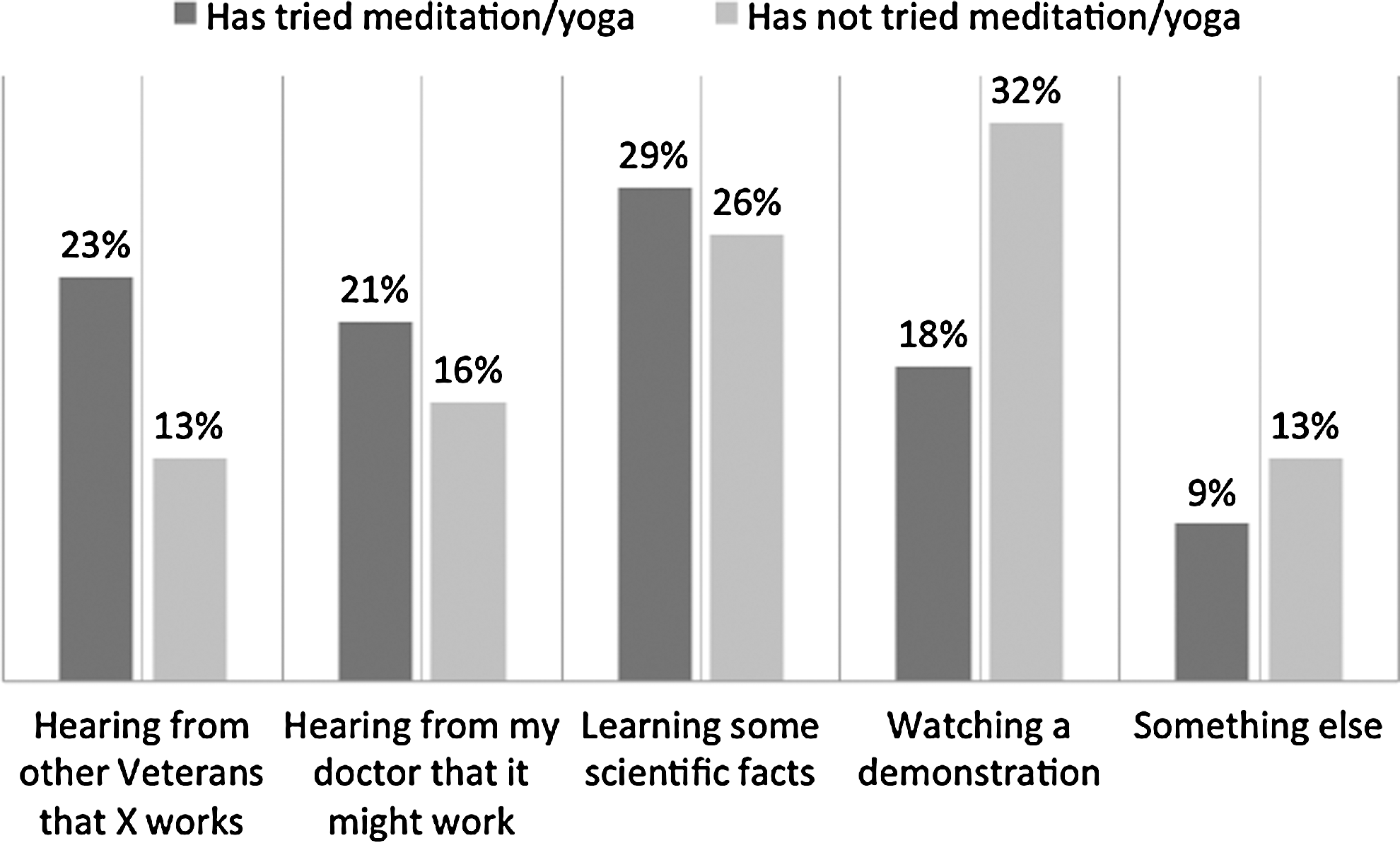
What makes veterans want to try meditation or yoga (n = 52).
Themes from focus group discussions with patients
Five themes emerged from the patient focus groups as being important aspects of patient education material and within each, actionable recommendations for CIH providers or educators emerged. Also, after viewing the final materials, the majority of patients said they would be likely to try meditation or yoga.
Theme 1: Patients' perspectives on content
Recommendation 1: Include information on who would be able to participate in yoga or meditation. For example, one patient noted, “I need to know that I can do it with my (physical and mental) limitations.” Another said, “One of the first things you usually think about something like yoga is ‘It's not for me…maybe you can include [specifics], like’ you can participate even if you're not flexible.” Recommendation 2: Include information on the benefits of meditation or yoga. As one patient said, “I especially like knowing what the benefits are.” Recommendation 3: Include information on how patients could participate and where they could find additional information. For example, one patient said, “Maybe the handout can include a link for more information so I can look at it at home before I talk to someone about it.” Others said, “Include information on the handout on what meditation resources exist and through what modality (classes, by phone, online, etc.)” and “Provide detailed information about the classes (i.e., are they drop in classes, and… what time are they offered?”)
Theme 2: Patients' perspectives on medium
Patients did not express a preference for any of the three educational mediums we examined. Recommendation: Show videos with patients doing CIH and recommending it and offer practice guides for at-home use. “Videos are powerful because I Iike to see veterans talking to veterans.” Patients said they listen to what their provider suggests they do to improve their health, but hearing from other patients was “more influential” to them. Patients who currently practiced yoga liked having a “how to” pocket guide to support their practice at home: “I try to remember what I've seen in yoga before, but something like this would make it so that I could do it at home in between times I'm at the VA.”
Theme 3: Patients' perspectives on written material format
Patients want brief and ascetically appealing materials. Recommendation 1: Keep it brief. The yoga or meditation-naive patients wanted all information on one page with brief, bulleted information. Those who have some idea of what yoga or meditation are want additional information on the second and third pages, printed on both sides so the material appears to be only one to two pages in total. Patients noted: “If it's long like that [3+ pages] my peers won't read it, they won't even pick it up” Recommendation 2: Use colors and images (see Theme 4): “Can you make it [the brochure] more vibrant, more active, more appealing to read?”
Theme 4: Patients' perspectives on images to include
For the meditation handout, we originally included a commonly used picture of a stack of gray, small smooth stones on a beach. For the yoga handout, we originally used a picture of a fit man doing a yoga posture. Patients said it would be better to use images that are specific to them and their conditions. Recommendation 1: Use images targeted toward patients and their health conditions. For example one veteran said: “I'm an x-Marine Corps Vietnam veteran. Don't show skinny girls, show people who are the same as me and with the same problems I have.” Furthermore, other veterans indicated “Images should convey that you don't have to be whole or perfect to benefit [from yoga].” Veterans reminded us: “We [veterans] are different from the rest of the public; we have more physical and mental limitations.” “I need to be shown [with images in recruitment materials] I can do it with my limitations.” Recommendation 2: Patients want images to convey “inclusivity” to all patients (i.e., women, fit and not fit people, and diverse races and ethnicities): “Picture needs to feel inclusive.”
Theme 5: Patients' perspectives on language to engage target audiences
Recommendation 1: Patients want language that can apply to many patients regardless of previous exposure to yoga/meditation. Suggestions included, “Do you have problems sleeping? Yoga might be able to help you…” “I love the word ‘relaxed’. A lot [of people] don't know what meditation is, but if I see the word ‘relax’ or ‘get calm’ or ‘calm down’, they are simple but bold and help [people] visualize the state they want to achieve.” Recommendation 2: Patients are sensitive to language that could be construed as pandering or condescending: “The language has to speak to me, I'm older, less patient… no platitudes, no patronizing.”
Themes from individual interviews with providers
Analysis of individual interviews with providers revealed five themes. Also, all providers said they would be likely to discuss yoga or meditation with some of their patients based on the materials we developed.
Theme 1. Providers wanted scientific evidence from top journals
Recommendation: Providers want evidence on the effectiveness of CIH. “It would impress me to see a high impact journal [when looking at academic evidence supporting CIH].” “I do want to see this type of material [scientific journal articles on CIH effectiveness].” Some providers considered the VA's CIH “evidence maps” 5 –10 (visual displays synthesizing the results of systematic reviews) to be useful for conveying the evidence concisely. However, some felt they should be simpler, having fewer dimensions (“I'm daunted”; It's “overwhelming to me, and I'm a researcher”).
Theme 2. Providers wanted concise information
Recommendation 1: Providers prefer all information be on one page with electronic links to additional information. Given their time demands prevent them from being able to read lengthier documents: “Ideally I want a one pager for each [CIH] modality.” Recommendation 2: Scientific journal abstracts are a good way to present information to providers without being overwhelming or time consuming: “I want to see an abstract [not the full paper].” Recommendation 3: Use links instead of attachments, as providers reported being more likely to access additional information if it could be reached through an electronic link instead of an attachment: “I want a list of articles with links embedded online so I don't have a million things in my email but I have the ability to go to these articles.” “I would like an email with a title so that when I file it I can find it again. It needs to be short so I can skim it. I don't need to open any attachments to see information–attachments are a hindrance and generally make me not want to open emails.”
Theme 3. Providers differ in how they want the materials organized
No clear theme emerged as a recommendation. Some providers want information organized by type of CIH (“Ideally I want [information] for each [CIH] modality”) and others want it organized by health condition (“What I want to know, as a provider, is: for what conditions does evidence support my use of acupuncture, for example?”), to quickly determine what type of CIH is a good treatment match for their patient's condition. Another provider recommended a combination approach: “I would like to have more of a flow chart of all the modalities at once so that I can look at patient circumstances to figure out which of the modalities would be best given each patient's specific circumstance and condition.”
Theme 4. Providers want practical, logistical information they can use during patient care
Recommendation 1: Providers want information to clearly explain CIH to their patients: “I really just want the tool for what I need in the exam room. I want to know [which of my patients] I should explain the experience of acupuncture to… I want to know how to explain the risks and benefits [of CIH to my patients] including the magnitude of the benefits, just as I would explain them for any other drug or therapy.” Recommendation 2: Providers want information on how to refer their patients to CIH in the hospital or community. “The thing that's really missing from the packets of information involves a local resources element. In order to make the information accessible locally, I need to know the name of the consulting provider and the restrictions on me in terms of which patients I can refer to each treatment modality and how many sessions I can prescribe.”
Theme 5. Providers felt colors and images made the provider facing materials less professional
Recommendation: Make provider materials look professional by not using bright colors, which providers considered “clown-like” or “juvenile,” and not using images. Providers wanted to see only black and white text with no images. Providers also did not want to see diagrams of poses as they felt that would be relevant only to someone considering practicing yoga or meditation.
Discussion
Our project elicited from patients and providers information on the key elements and formats to consider in developing CIH educational materials that can be used in shared decision making. We found patients did not express a preference for any particular educational medium. They were influenced by seeing patients in videos and want written educational material to be one to two pages. Materials should include: (1) a brief description of what occurs in typical yoga or meditation classes, (2) a brief description of who can join and that classes can be modified to suit different abilities, (3) the key benefits to health and wellness, and (4) how to find classes at the hospital or clinic. Similarly, providers wanted educational information to be one page of brief black and white text without images, with practical information for referral, and containing a bulleted listing of scientific evidence on the effectiveness of CIH therapies in high-impact journals with journal abstracts in email links.
Our findings have implications for patient-centered, nonpharmacological clinical care. Educational materials with the components and formats we found to be key might assist in any shared decision-making process about CIH therapies, a process which is essential to delivering patient-centered care. That is, better informed patients and providers might be more able to have effective conversations about the use of CIH therapies to address their health concerns. Such materials materials might also facilitate the uptake of CIH therapies.
The Department of Health and Human Services National Pain Strategy 26 and the Center for Disease Control and Prevention's guidelines for prescribing opioids for chronic pain, 27 emphasize a need to better understand the effectiveness of Non Pharmacologic Therapies for chronic pain as well as broaden their availability. Facilitating the uptake of CIH therapies has never been more timely.
This project has some limitations. Our findings might not be generalizable to the average patient population because 80% of veteran patients are male and they tend to have higher rates of pain. 28,29 They are, however, similar to male Medicare beneficiaries in the general population. 30
Also, a surprisingly high percentage (62%) of patients had prior experience with meditation or yoga, possibly because yoga and meditation are available to active military through the Department of Defense programs. We also do not know if patients actually used yoga or meditation as a result of these materials, nor do we know if providers actually referred their patients to these classes; we only assessed intent.
Conclusions
Providers and patients want specific types of information on CIH therapies in particular formats. The information learned and materials developed in this project can be used in others' efforts to educate patients and providers on CIH therapies.
Footnotes
Acknowledgments
This project was funded by the Department of Veterans Affairs' Office of Patient-Centered Care and Cultural Transformation, Health Services Research and Development, and Quality Enhancement Research Initiative.
Author Disclosure Statement
No competing financial interests exist.