
Abstract
Objectives:
Burnout, a state of emotional exhaustion associated with negative personal and occupational outcomes, is prevalent among healthcare providers. A better understanding of the psychological factors that may be associated with resilience to burnout is essential to develop effective interventions. Self-compassion, which includes kindness toward oneself, recognition of suffering as part of shared human experience, mindfulness, and nonjudgment toward inadequacies and failures, may be one such factor. The purpose of this study was to examine the relationships between burnout, depression, and self-compassion in Veterans Affairs (VA) mental health staff.
Design:
Cross-sectional study.
Setting:
VA medical center and affiliated community-based clinics.
Participants:
VA mental health staff.
Outcome measures:
The 19-item Copenhagen Burnout Inventory, the 26-item Self-Compassion Scale, and the Patient Health Questionnaire 2-item depression screen. Demographic information included age, sex, years worked in current position, and number of staff supervised.
Results:
One hundred and twenty-eight of a potential 379 individuals (33.8%) responded. Clerical support, nursing, social work, psychology, and psychiatry were the major professions represented. Self-compassion was inversely correlated with burnout (r = −0.41, p < 0.001), and inversely correlated with depression (r pb = −0.39, p < 0.001). The inverse relationship between self-compassion and burnout remained significant even after accounting for depressive symptoms and demographic variables in a multiple linear regression model. Of all the variables examined, self-compassion was the strongest predictor of burnout.
Conclusions:
The results of this study support the hypothesis that self-compassion may be associated with resilience to burnout. Alternatively, decreased self-compassion may be a downstream effect of increased burnout. Prospective, longitudinal studies are needed to determine the directional relationship between these factors, and whether interventions that cultivate self-compassion may decrease burnout and/or protect against its negative personal and professional outcomes.
Introduction
H
Despite these issues, effective interventions to reduce healthcare provider burnout are lacking. A 2015 Cochrane review examined the evidence of 58 studies, totaling >7000 participants, on interventions to address occupational stress or burnout in healthcare providers. While the quality of evidence for relaxation versus no intervention was moderate, quality of evidence for other interventions such as cognitive-behavioral therapy and organizational strategies (changing work schedules, changing working conditions, increasing communication skills) was low. 4 Additionally, a recent meta-analysis examined person-directed versus organization-directed interventions for burnout in mental health providers. 5 Person-directed interventions teach stress-coping skills and relaxation techniques, whereas organization-directed interventions modify aspects of the work environment such as poor staff cohesion, work overload, and insufficient job resources. The results of the meta-analysis showed that “person-directed interventions were more effective than organization-directed interventions at reducing emotional exhaustion,” though overall, “the field has made limited progress in ameliorating mental health provider burnout.” 5
Mindfulness-based interventions (e.g., Mindfulness-Based Stress Reduction [MBSR]) are of increasing interest in the treatment of a wide range of stress-related issues. 6 Mindfulness involves paying full attention to the present moment without judgment, supported by underlying attitudes of openness, acceptance, and curiosity. Mindfulness is associated with multiple benefits, including increased subjective well-being, reductions in negative psychological symptoms and emotional reactivity, and improved emotional and behavioral self-regulation. 7 A systematic review of MBSR or MBSR-based interventions in healthcare providers concluded that while such approaches are associated with improvements in burnout, stress, anxiety, and depression, there remains a need to understand the specific mechanisms facilitating these benefits, including potential impacts of the interventions on empathy and emotional competencies. 8
One of the mechanisms by which mindfulness-based interventions may achieve their beneficial effects is through the cultivation of self-compassion. 9 Self-compassion incorporates mindfulness along with the concepts of kindness toward oneself, recognition of one's experience as an integral part of being human, openness to one's own suffering, and holding a nonjudgmental attitude toward one's inadequacies and failures. 10 A self-compassion scale has been developed, validated, and widely used in studies of psychological health. 10 Self-compassion is consistently associated with lower levels of anxiety and depression, and is related to positive changes in behavior such as the ability to cope effectively with a variety of negative outcomes including academic failure and divorce. 11,12 Self-compassion is a stronger predictor than mindfulness of symptom severity and quality of life in individuals with anxiety and depression. 13
Individuals higher in self-compassion are less likely to suppress unwanted thoughts and emotions, and they are more likely to acknowledge their emotions as valid and important. 14 Individuals higher in self-compassion also have decreased negative response to negative self-relevant events. 15 Self-compassion may lessen the impacts of negative experience, by helping to counterbalance the negative feelings resulting from such experiences, allowing for a more positive and balanced state of mind. These aspects may underlie why self-compassion is correlated with positive psychological strengths like emotional intelligence, wisdom, life satisfaction, and feelings of social connectedness. 16
Since 2015, a few studies on healthcare providers support the idea that self-compassion may promote resilience to burnout in nurses, 17,18 midwives, 19 and pediatric/medicine-pediatric residents. 20 However, these studies used varying definitions and measures of the burnout construct, and generalizability to a broader multidisciplinary healthcare provider population is limited. The purpose of this study was to investigate the relationship between burnout and self-compassion in a group of Veterans Affairs (VA) mental health staff, with the hypothesis that these factors are inversely correlated.
In this study, burnout was defined specifically as a state of emotional exhaustion. Across the various research and clinical definitions of burnout, emotional exhaustion is the most consistent, core feature. 21 Meanwhile, the other components of burnout as defined in the commonly used Maslach Burnout Inventory (MBI)—depersonalization and low personal accomplishment—are less consistently found in the varying definitions of burnout. 22 The MBI potentially confounds the core feature (emotional exhaustion), with a coping strategy (depersonalization), and one of the many consequences (reduced personal accomplishment) of burnout. 2 Therefore, this study aimed to avoid the tautological concerns that have been raised against the MBI: “Burnout is what the MBI measures, and the MBI measures what burnout is.” 2
Additionally, this study took into account depressive symptomatology in participants, for several reasons: (1) To address a gap in prior studies of burnout and self-compassion that have not accounted for depression, (2) to examine whether an inverse relationship between self-compassion and burnout is specific to burnout and not predominately driven by an inverse relationship between self-compassion and negative affective states generally, and (3) to place these results in the context of ongoing debate on the distinction between burnout and depression, given criticisms in the literature on the lack of consensual burnout diagnostic criteria. 23
Materials and Methods
Participants and procedures
This study was entirely conducted within the VA Healthcare System. Institutional Review Board (IRB) exempt status and Research and Development (R&D) committee approval was obtained for all parts of this study. All Minneapolis VA mental health service line staff were invited to participate, via the internal e-mail distribution list. Individuals on this list consist of a multidisciplinary group of staff. Their primary work site is either the central Minneapolis VA, or one of several affiliated community-based outpatient clinics within the Veterans Integrated Service Network. The total number of individuals on this list, at the time of survey distribution, was 379.
Potential participants were sent an e-mail describing the survey, informing them of any potential risks and benefits of participating, and inviting participation through Survey Monkey (
Measures
In addition to providing information on age, sex, job position, years worked in current position, and number of staff supervised, participants completed the following self-report measures:
The 19-item Copenhagen Burnout Inventory (CBI) consists of three scales measuring personal burnout, work-related burnout, and client-related burnout. The rationale for using the CBI was to focus on emotional exhaustion as the primary feature of burnout, with an inventory that is nonproprietary and publically available. As described in the original CBI article: Personal burnout is “the degree of physical and psychological fatigue and exhaustion experienced by the person,” work-related burnout is “the degree of physical and psychological fatigue and exhaustion that is perceived by the person as related to his/her work,” and client-related burnout is “the degree of physical and psychological fatigue and exhaustion that is perceived by the person as related to his/her work with clients.” Responses are given on a 5-point scale ranging from 1 (never or to a very low degree) to 5 (always or to a very high degree). Scores for each scale and a total burnout score can be calculated. In the initial study of this inventory, internal reliability of the scales was high, ranging from 0.85 to 0.87. The overall measure demonstrated good concurrent, criterion-related, and predictive validity. 2
The 26-item Self-Compassion Scale (SCS) assesses the positive and negative aspects of self-compassion: self-kindness versus self-judgment, common humanity versus isolation, and mindfulness versus over-identification. Response are given on a 5-point scale ranging from 1 (almost never) to 5 (almost always). A mean score of self-compassion is then calculated. Internal consistency for the 26-item SCS, in its initial study, was 0.92. 10
The Patient Health Questionnaire-2 (PHQ-2) is a 2-item screening measure for depression that assesses severity of depressed mood and anhedonia over the past 2 weeks. Each symptom is scored from 0 (not at all) to 3 (nearly every day). Utilizing a structured interview by a mental health professional as the criterion, scores greater than or equal to 3 had a sensitivity of 83% and specificity of 92% for major depression. Likelihood ratio and receiver operator characteristic analysis identified a score of 3 as the optimal cutoff point. 24
Data analysis
In Survey Monkey, items were provided weights to automatically reverse-code as appropriate. Data were exported from Survey Monkey into a Microsoft Excel spreadsheet, for further calculations. Demographic variables were summarized using descriptive statistics.
SCS scoring was performed by taking the average score of all 26 items (score range 1.0–5.0), with a higher score representing a higher degree of self-compassion. Individual subscale scores were not calculated, as the factor structure for these subscales has been questioned when looking at populations outside of those in whom the survey was originally developed. 25 CBI scoring was performed by scaling all of the individual item responses to a 0–100 range, for consistency with the original study. 2 Then, the average score was calculated for each subscale and the total score. Possible score range for all subscales and total was 0–100, with a higher score representing a higher degree of burnout. PHQ-2 scoring was performed by adding the scores on the two items (score range 0–6). Participants were then categorized as either screening negative (total score <3) or positive (total score ≥3) for depression.
For any job position in which fewer than eight individuals responded, their data were combined with at least one other group, to maintain a high level of anonymity. Descriptive statistics were calculated using Microsoft Excel 2013. Cronbach's alphas, Pearson's correlations (r), point-biserial correlations (r pb), phi correlations (r φ), linear regression models, and analyses of variance (ANOVAs) were calculated using R version 3.3.1, in RStudio version 0.99.902. For correlations, self-compassion score, total burnout score, and depression screening were the primary analysis variables. Additional, exploratory correlation analyses were conducted using the burnout subscales and demographic variables. For linear regression models, total burnout score was the outcome of interest. Predictors for total burnout included self-compassion, depression, and the demographic variables.
Results
Participant characteristics
One hundred and twenty-eight out of a potential 379 participants responded to the survey, for an overall response rate of 33.8%. Demographic characteristics of respondents are shown in Table 1. The sex distribution of the 128 respondents was similar to those of the total group of 379 potential respondents: 96 (75%) of the 128 respondents were female, while the total group consisted of 267 (70.4%) women. Clerical support, nursing, social work, psychology, and psychiatry were the main disciplines represented among the 128 respondents. Comparing the percentage of respondents belonging to these disciplines to their percent representation in the full group of 379 also showed high similarity: Clerical support (6.3% vs. 11.9%), nursing (20.3% vs. 21.4%), social work (20.3% vs. 19.8%), psychology (21.9% vs. 21.9%), and psychiatry (12.5% vs. 11.1%). Those who identified as “Other” were likely to have been in positions of vocational rehabilitation, pharmacy, peer support, housing specialist, and neuropsychological assessment technician. Descriptive statistics for self-compassion, burnout, and depression in the total group are shown in Table 2.
Correlations
Self-compassion was negatively correlated with total burnout (r = −0.41, p < 0.001) and negatively correlated with depression (r pb = −0.39, p < 0.001), while depression and total burnout were positively correlated (r pb = 0.27, p < 0.01). Multiple additional significant correlations were present between variables, as determined in exploratory analysis of the burnout subscales and demographics (Table 3). Figure 1 is a scatterplot of self-compassion versus total burnout scores for all 128 respondents.
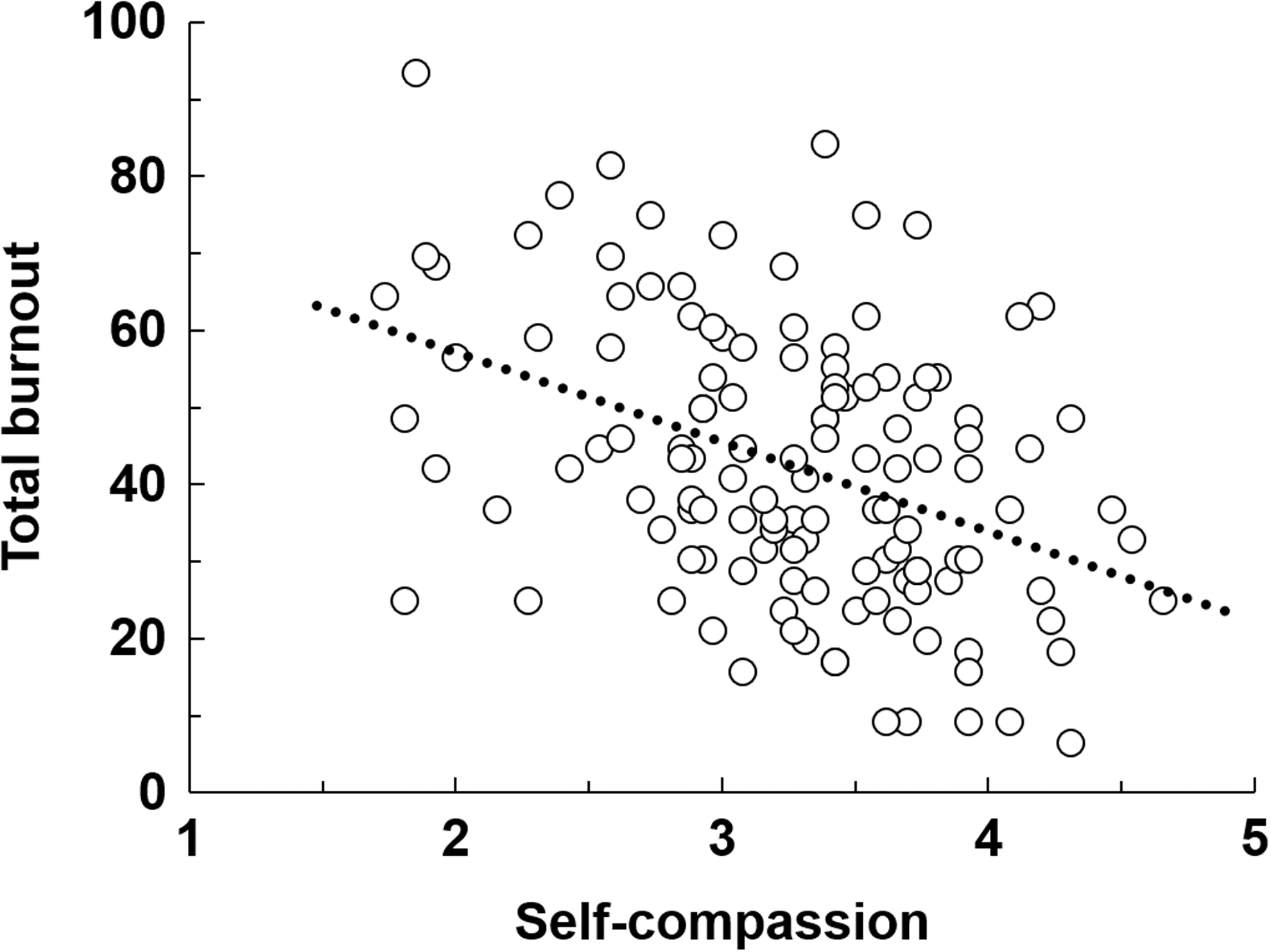
Scatterplot of self-compassion versus total burnout scores for all respondents (n = 128, r = −0.41, p < 0.001).
p < 0.05; ** p < 0.01; *** p < 0.001.
CB, client-related burnout; Dep, depression; PB, personal burnout; SC, self-compassion; Staff, staff supervised; TB, total burnout; WB, work-related burnout; Years, years worked.
Linear regression models
Linear regression models predicting total burnout as a function of the other variables are shown in Table 4. Only respondents without missing data for any of the variables were included (n = 118). In model 1, which examined demographics (age, sex, years worked, staff supervised) as predictor variables, a nonsignificant regression equation was found (F (4, 113) = 1.48, p = 0.21), with an adjusted R 2 of 0.02. Model 2 added depression as a predictor variable. A significant regression equation was found (F (5, 112) = 3.48, p < 0.006), with an adjusted R 2 of 0.10. Model 3 added self-compassion as a predictor variable. A significant regression equation was found (F (6, 111) = 4.53, p < 0.001), with an adjusted R 2 of 0.15. In the full model, self-compassion was the strongest predictor of burnout. ANOVAs were conducted between the successive models to determine whether the addition of predictor variables at each step conferred significant change in explanation of variance. The addition of depression as a predictor resulted in a statistically significant change in R 2 between Model 1 and Model 2 (ΔR 2 = 0.08, p < 0.002). The addition of self-compassion as a predictor resulted in a statistically significant change in R 2 between Model 2 and Model 3 (ΔR 2 = 0.06, p < 0.005).
B, unstandardized coefficient; DF, degrees of freedom; RSS, residual sum of squares; SE, standard error; SS, sum of squares; β, standardized coefficient.
Internal consistency of measures
Cronbach's alphas for the 26-item SCS (α = 0.94), the 19-item CBI (α = 0.95), and the 2-item PHQ-2 (α = 0.77) all showed satisfactory degrees of internal consistency.
Discussion
The results of this study support the hypothesis that self-compassion is inversely associated with burnout in a multidisciplinary group of mental health staff, and that this inverse relationship holds after accounting for depressive symptomatology. Given that self-compassion has been inversely associated with various negative affective states, 11,12 the preservation of a significant inverse association between self-compassion and burnout even after accounting for depression supports the strength and specificity of this relationship. Although self-compassion was the strongest predictor of burnout in the full model, there was still a large degree of unexplained variance in this final regression model. This is not surprising, considering that multiple other unmeasured variables—such as organizational and institutional factors—have been implicated in burnout. 3
These results are consistent with other research on self-compassion and burnout in various healthcare populations. A cross-sectional study of 280 registered nurses found a significant negative correlation (r = −0.44) between self-compassion and the burnout subscale of the Professional Quality of Life scale, which defines burnout as “feelings of hopelessness and difficulties in dealing with work or in doing one's job effectively.” 17 Another study of 45 first-year pediatric and medicine-pediatric residents found a significant negative correlation (r = −0.35) between self-compassion and the emotional exhaustion subscale of the MBI. 20
While a cross-sectional design precludes determination of causal relationships between the variables measured, one potential interpretation of this study's results is that self-compassion is a protective factor against burnout. This interpretation is consistent with self-compassion's association with effective coping and decreased negative response to stressful life events. 15,16 Additionally, self-compassion may modify the degree or impact of individual etiological factors for burnout, such as high expectations of oneself, perfectionism, and suppression or neglecting of one's own health and well-being needs. 22,26 An alternative interpretation of the results is that decreased self-compassion may be a result of increased burnout. Just as burnout is associated with multiple negative occupational and personal impacts, 2,3 diminished self-compassion may be another downstream effect of burnout.
Preliminary research on an 8-week mindful self-compassion program provides initial support that self-compassion is trainable, with positive gains maintained at 6-month and 1-year follow-up. 27 If self-compassion is ultimately demonstrated to be a protective factor against burnout, and is modifiable through such programs, then self-compassion training may be a beneficial intervention for burnout resilience. If longitudinal studies determine that decreased self-compassion is a result of burnout, then self-compassion programs may still have a place in mitigating the negative impacts of burnout, within the context of other individual and organizational efforts to address burnout's underlying causes.
Strengths
This present study builds upon and extends the findings of other studies on healthcare provider self-compassion and burnout. To the authors' knowledge, this study is the first to simultaneously examine self-compassion, burnout, and depression in a multidisciplinary health provider population. Additionally, this study utilized a less-known measure of burnout, the CBI, which is nonproprietary and thereby more readily available for use in further research. In using the CBI rather than the MBI, this study examined burnout's core feature (emotional exhaustion), while reducing the potential conflation of this concept with a coping strategy (depersonalization) and consequence (reduced personal accomplishment). 2
Limitations
This study has several limitations. As described, due to the cross-sectional study design, determination of causality between the variables examined is not possible. A second limitation is the voluntary nature of the survey, along with the modest (33.8%) response rate. Potentially, participants more likely to respond to a voluntary survey may differ in variables of interest from the larger group invited to respond. A third limitation is the use of the PHQ-2 in assessing depression. Although the PHQ-2 has high accuracy relative to the PHQ-9 in identifying cases of depression, 28 it is neither capable of assessing the full array of depressive symptoms nor designed to discriminate between different severities of depression. Future studies should utilize a more in-depth instrument to assess depression.
Conclusions
This study expands upon the current literature on healthcare provider burnout and potential resilience factors. Prospective, longitudinal studies are needed to determine the causal relationship between these factors, and whether interventions that cultivate self-compassion may decrease burnout and/or protect against its negative personal and professional outcomes.
Footnotes
Acknowledgments
The authors thank all who participated in this study. Compliance with ethical standards: This study was determined as IRB exempt under 45 CFR 46.101(b). This study was reviewed and approved by the Research & Development committee at the primary study site. No individually identifiable information was collected from participants.
Author Disclosure Statement
No competing financial interests exist.