
Abstract
Objectives:
Postpartum hemorrhage (PPH) is one of three main causes of maternal mortality and a life-threatening condition throughout the world. PPH can have irreversible complications for the mother even if it does not lead to death. This study was conducted to determine the effect of hydroalcoholic extract of Capsella bursa pastoris on early PPH.
Design:
The present study was a single-blinded, randomized, clinical trial.
Setting:
The study was conducted in Afzalipour Hospital of Kerman in 2015.
Subjects:
The subjects included 100 women who had given vaginal birth and met the study inclusion criteria.
Intervention:
The participants were selected and randomly assigned into an intervention group (n = 50) and a placebo group (n = 50). Immediately after placental expulsion, the intervention group was given 10 sublingual drops of the hydroalcoholic extract of Capsella bursa pastoris plus an infusion of 20 U of oxytocin in 1 L of Ringer's solution, and the control group was given 10 sublingual drops of the placebo plus an infusion of 20 U of oxytocin in 1 L of Ringer's solution.
Outcome measures:
The amount of bleeding was assessed in both groups. Hemoglobin and hematocrit levels were measured in all the participants 6 h after childbirth. The statistical analysis of the data was performed in SPSS-17 using the following tests: independent t, paired t, repeated measures ANOVA, Friedman's, Wilcoxon, Mann–Whitney, Fisher's exact, and chi square. P-value <0.05 was considered statistically significant.
Results:
There were no significant differences between groups in baseline characteristics (p > 0.05). After the intervention, there was significant decrease in the amount of postpartum bleeding in both groups. However, the mean decrease in the amount of bleeding was significantly more in the Capsella bursa pastoris group (p < 0.001).
Conclusion:
Compared with the mere administration of oxytocin, sublingual Capsella bursa drops appear to be effective in reducing PPH in this study. Further research regarding the efficacy and safety of various doses of Capsella bursa pastoris is required.
Introduction
A
Hemorrhage is the cause of one-third of all maternal deaths in Africa and Asia, where most maternal deaths occur. The majority of these deaths happen in the first 4 h postpartum and are caused by complications developed in the third and fourth stages of labor. 3
In Iran, there were 162 cases of maternal death in 1997, and 40% of them were caused by hemorrhage. Hemorrhage was indeed identified as the most common direct cause of maternal death in the 1990s in Iran. 4
Only one-third of the risk factors of PPH have been identified to date, including a history of PPH, hyperextended uterus (such as in the case of multiple pregnancies and a large fetus), placental abnormalities (such as placenta previa or placenta accreta), and coagulation problems. Although most women with PPH have no previous risk factors, multiparity is associated with an increased risk of PPH. 5,6
PPH entails consequences such as anemia, postpartum infection, acute renal failure, Sheehan's syndrome, blood transfusion complications and hysterectomy, infertility, and conditions such as adult respiratory distress syndrome and even death in some cases. 7
Since uterine atony is the most common cause of PPH, the prevention of uterine atony is the first line of treatment that includes uterine fundal massage, bimanual uterine massage, the use of uterine contractors such as oxytocin, methergine, prostaglandins, especially misoprostol, and invasive procedures. Because of its fewer side-effects, oxytocin is used as the first line of treatment for PPH. 8
Today, the use of herbal products is increasing across the entire world and the use of herbal medicine has, therefore, become a subject of interest for the prevention of hemorrhage. The use of herbal medications has a long history and is widely accepted by all societies. According to a World Health Organization report, 80% of the world's population use medicinal herbs. Nonmedical therapies, including herbs such as dill seed extract, Xuesaitong, and dates are effective in reducing hemorrhage after vaginal childbirth. 9 –11
Capsella bursa pastoris, also known as Shepherd's purse, is from the Cruciferae family and contains various compounds such as tannin, choline, acetylcholine, flavonoids, amino acids, fatty acids, sterol, thiamine, ascorbic acid, calcium, potassium, β-carotene, vitamin K, niacin, and iron. 12 –14 According to previous studies, Capsella bursa pastoris has oxytocic activities and antiulcer and anti-inflammatory properties. 15 This plant affects uterine smooth muscles and increases their contraction and is an astringent that is used orally in the treatment of heavy menstrual bleeding or uterine bleeding between menstrual periods. 12,16
Early PPH is the main cause of maternal mortality in the world and especially in Iran. Furthermore, uterus atony is the most common cause of PPH. The contractile and anti-inflammatory properties of Capsella bursa pastoris 15 can alleviate this condition. Since no studies examined the effect of this plant on early PPH, this study was conducted to determine the effect of the hydroalcoholic extract of Capsella bursa pastoris on early PPH, so that this plant can be used as a low-cost treatment with few complications if proven effective.
Materials and Methods
The present single-blinded, randomized, clinical trial was conducted in 2015 on the effect of the hydroalcoholic extract of Capsella bursa pastoris on early PPH in women presenting to the maternity ward of Afzalipour Hospital in Kerman. This study was approved by the ethics committee of Shahid Beheshti University of Medical Sciences (SBMU2.REC.1394.16) and was registered at the Iranian Registry of Clinical Trials (IRCT2016072529066N1).
The study inclusion criteria consisted of age between 20 and 35 years, less than three pregnancies, gestational age between 37 and 42 weeks, single fetus with a cephalic presentation, fetal weight between 2500 and 4000 g, no known systemic diseases (diabetes, hypothyroidism, and coagulation disorders), no history of cesarean section, uterine surgery, or PPH, no pregnancy complications (polyhydramnios and gestational bleeding and hypertension), no maternal anemia, no use of magnesium sulfate during pregnancy, clear amniotic fluid in the first stage of labor, no extensive episiotomy in the second stage of labor (third or fourth-degree tears), and a normal duration in stage 1 of labor (4.6–11.7 h for the nulliparous cases and 2.4–5.2 h for the multiparous), in stage 2 (50 min for the nulliparous cases and 20 min for the multiparous), and also in stage 3 (30 min for both).
The study exclusion criteria consisted of cesarean section, unwillingness to continue the study, sensitivity to Capsella bursa pastoris, and severe hemorrhage. The data collection tools used included a demographic and obstetrics information questionnaire that collected data on previous and current pregnancies and childbirths, and an observation checklist for recording data on the first, second, third, and fourth stages of labor. Complete blood count (CBC) was performed using a Sysmex xp-300 (made in Japan). The qualitative control of the Sysmex xp-300 device was performed every month using a control blood sample.
First, the researcher visited the study setting, that is, the labor and postpartum wards of the hospital, and selected women who met the inclusion criteria. She introduced herself, ensured them of the confidentiality of their data, obtained their consent, and briefed them on the objectives and methods of the study.
Capsella bursa pastoris was purchased from an herbalist at Tabriz medicine market and its identity was confirmed at the botanical laboratory of Shahid Beheshti School of Pharmacy. The plant was then powdered and soaked in 96% ethanol three times overnight for extraction and concentration and then poured into a 30-mL dropper. According to the literature, this plant is safe and harmless and has no side-effects, especially in therapeutic doses (12 g/day). Doses in excess of 25 g/day are best avoided. 17 The plant extract was given in the form of 10 single-dose drops, each drop containing 50 mg of the hydroalcoholic extract of Capsella bursa pastoris. The Capsella bursa pastoris and placebo drops were prepared in completely similar shapes, sizes, and doses. The participants were told that they would be randomly placed in one of the two groups.
The information questionnaire was completed in both groups and the data pertaining to the first and second stages of labor were recorded in the observation checklist. The researcher monitored the duration of the participants' third stage of labor and recorded all the pertinent data. After the complete removal of the placenta and fetal membranes, the control group received an infusion of 20 U of oxytocin in 1 L of Ringer's solution and 10 drops of the placebo, whereas the intervention group received an infusion of 20 U of oxytocin in 1 L of Ringer's solution and 10 drops of Capsella bursa pastoris, which was poured under the participant's tongue and kept there for 1 min.
The weighted blood loss (WBL) and peripartum CBC measurement were utilized to detect PPH. The WBL seems to be more promising as a blood loss diagnostic technique in a high prevalence setting. 18 In both groups, a previously weighed plastic covered drape was immediately spread under the mother's pelvis and a previously weighed sanitary pad was given to her as well. The pad and drape were changed and weighed on the scale every hour until the third hour after the removal of the placenta. Blood loss was estimated as 1 mL per each gram of weighted pad or gauze. This was subtracted from the dry pad, as previously described. 19 If perineal repair was required, no pad was given to the subject in the first hour; instead, her bloody gauzes were weighed. The participants' vital signs were measured and recorded 15, 30, 45, 60, 120, and 180 min after delivery. A total of 2 mL blood samples were taken from all the participants at the onset of labor and 6 h after their delivery so as to measure their hemoglobin and hematocrit levels. All the blood samples were taken by the same laboratory personnel and assessed using the same device. The research assistant who measured blood loss and the laboratory staff who performed laboratory tests were blinded to treatment groups.
Three hours after the third stage of labor and once all the weighed pads and drapes were distributed by the assistant researcher and the stability of their vital signs was ensured, the participants were transferred to the postpartum ward. The participants were once again assessed by the researcher 6 h after delivery. They were additionally followed up with more than 10 phone calls with 4-day intervals, and each time, the participant was asked about symptoms such as severe bleeding or the hospitalization of herself or the infant and any other complications such as gastrointestinal conditions and allergies. The researcher gave her phone number to all the participants, so that they could call to get help about any problems or whether they had any questions.
The eligible participants were randomly assigned to the Capsella and control groups using Excel software. Sample size was determined as 50 per group, considering the significance level of 0.05, the effect size of 0.6, the statistical power of 0.84, the minimum sample size of 90, and the potential attrition of 10%. Data were analyzed in SPSS-17 using descriptive statistics (including frequency distribution tables and mean and standard deviation indices) for describing the participants' characteristics and their medication side-effects and also using analytical tests (including the independent and paired t tests, the repeated measures ANOVA, Wilcoxon's test, Mann–Whitney's test, Fisher's exact test, and the chi-square test) for the inter- and intragroup comparison of the intervention and control groups.
Results
This study reviewed 310 potential candidates and selected 100 of them as the study participants. By the end of the study, five of the participants in the intervention group were excluded: three due to the infant's hospitalization at the NICU and two because of having spit the drops. In the control group, five were excluded: three due to unwillingness to continue participation and two due to a prolonged second stage of labor. All these were replaced, so that each group still consisted of 50 participants (Fig. 1).
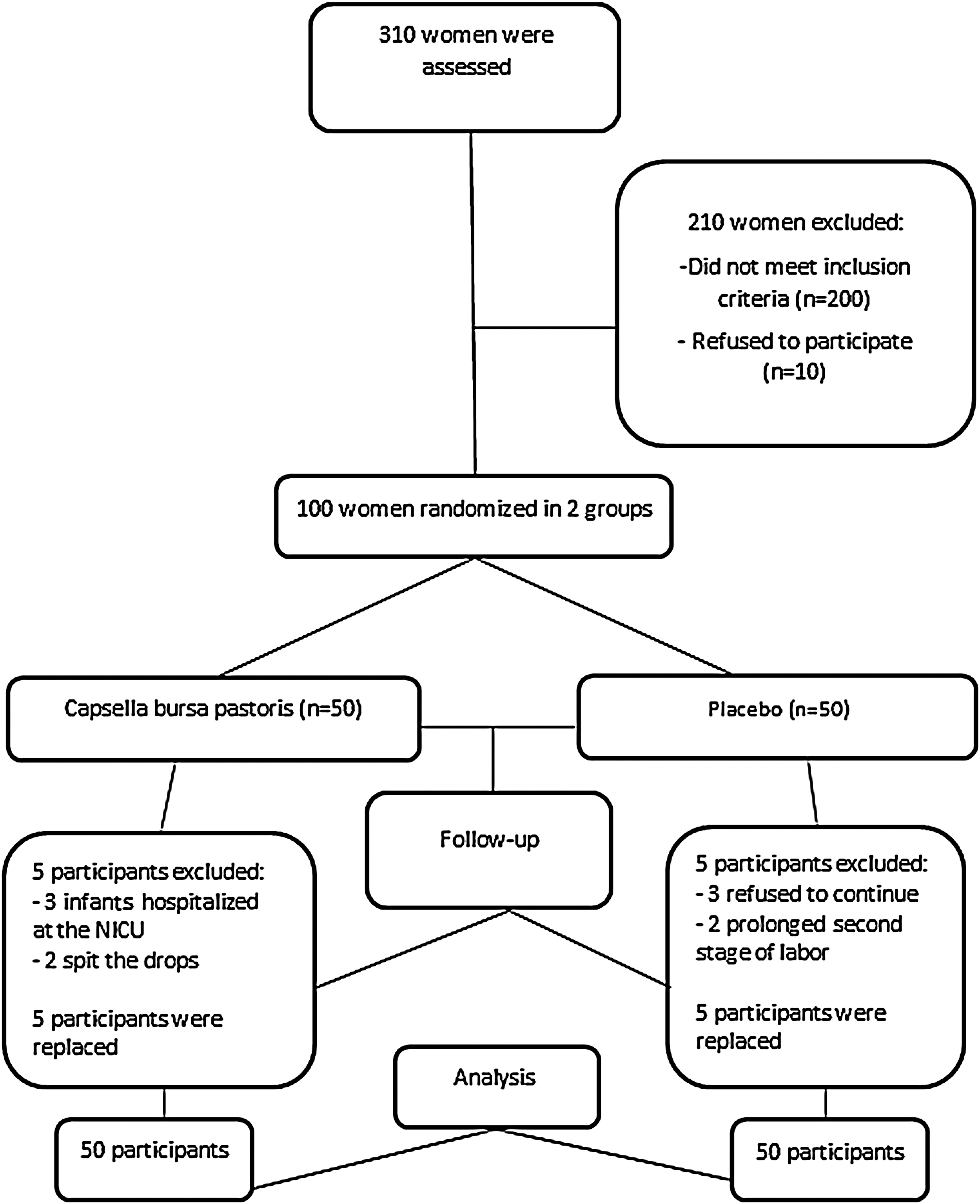
Flow of the participants through the study.
The results showed no significant differences between the two groups in terms of education (p = 0.695), mother's occupation (p = 0.401), pregnancy interval (p = 0.373), body–mass index (p = 0.789), and gestational age (p = 0.721), and the groups were matched. The two groups were also homogeneous in terms of labor induction (p = 0.410), duration of induction (p = 0.475), amount of oxytocin administered for induction (p = 0.512), hemoglobin and hematocrit levels at the onset of labor (p = 0.179 and p = 0.132), episiotomy (p = 0.0414), the weight of the gauzes soaked due to episiotomy (p = 0.711), and the amount of oxytocin administered after delivery (p = 0.08). Table 1 presents some of the demographic and obstetric characteristics of the participants.
t test.
Mann–Witney test.
Table 2 presents the mean amount of blood loss in the first, second, and third postpartum hours and the entire 3 h in the “oxytocin plus placebo” group (the control group) and the “oxytocin plus Capsella bursa pastoris extract” group (the Capsella group). The statistical tests showed a significant difference between the two groups in terms of the amount of blood loss (p < 0.001).
t test.
Mann–Witney test.
The two groups were also significantly different in terms of their mean hemoglobin and hematocrit levels 6 h after delivery (p < 0.0001), such that the amount of decline in hemoglobin and hematocrit level was lower in those in the Capsella group than those in the control group (Table 3).
The t test.
Mann–Whitney's test.
The results showed a significantly higher level of satisfaction with the treatment in those in the Capsella group (28% highly satisfied and 82% satisfied) than in those in the control group (2% highly satisfied and 28% satisfied; p < 0.0001).
As for medication side-effects, only one of the participants (2%) in the Capsella group experienced a sore and itchy throat, and one of the controls (2%) experienced nausea; no statistically significant differences were observed between the two groups in terms of side-effects.
Discussion
According to the finding of this study, hydroalcoholic extract of the aerial shoots of Capsella bursa pastoris was more effective in reducing early PPH. Given the lack of studies on the effect of this plant extract on PPH, this study discusses similar studies on medications or plants with similar active compounds and mechanisms.
Capsella bursa pastoris extract contains several active compounds, including tannin, choline, acetylcholine, sterol, and flavonoids, 13 and all of them contribute to the control of PPH. Some of these compounds control inflammation through their antioxidant and anti-inflammatory properties and some others cause uterine contraction, whereas others exert hormonal effects to control bleeding. Previous studies have shown that this plant has contraction and anti-inflammatory activities. 15
Dates have been used in several studies for controlling early PPH. Tannin is an active compound of dates that causes the contraction of the uterine muscles and the myometrium through its astringent properties and thus results in a significant reduction in early PPH compared with when oxytocin is used. 9 Tannin is also one of the active compounds of Capsella bursa pastoris that must have reduced early PPH compared with oxytocin. 20 In the study conducted by Mojahed et al., by the end of the second postpartum hour, the amount of bleeding was lower in the “oxytocin plus dates” group than in the group that had received only oxytocin. 9
Khadem et al. also examined the effect of oxytocin and dates on PPH in 62 women divided into two groups, and found that by the end of the first postpartum hour, the mean amount of bleeding was significantly lower in the group consuming dates. 21 Another study conducted by Mahdavian et al. entitled “An Investigation of Effectiveness of Oral Dill Extracts on Postpartum Hemorrhage” showed that the oral intake of dill seed extract can reduce PPH more than when intramuscular oxytocin is administered. Dill seed is among the plants that contain tannin and anethol and is an astringent for uterus smooth muscles. 10 Capsella bursa pastoris can probably reduce PPH through the same mechanism as dill seed, that is, through active compounds known as tannin.
In a study entitled “The Effect of the Hydro-Alcoholic Extract of Capsella bursa pastoris on Menorrhagia,” Naafe' et al. showed a significant reduction in the amount of menstrual bleeding in the group receiving the hydroalcoholic extract of the aerial shoots of this plant compared with those in the controls (p < 0.001), and a significantly greater reduction was also observed in the duration of menstrual bleeding in the Capsella group than in the controls (p < 0.001). 22
The aerial shoots of Capsella bursa pastoris contain several types of flavonoids that mediate the plant's strong antioxidant properties. 13 It is likely through this property that Capsella bursa pastoris reduces PPH.
In this study, oxytocin was administered to all the participants due to its well-known effect as a first-line treatment for PPH and because it was unethical to deprive any of the participants from this standard treatment.
All the participants in this study received a standard dose of oxytocin administered through a standard method, that is, the infusion of 20 U of the hormone in 1 L of Ringer's solution. 2 As a result of meeting these standards, the complications normally caused by high and undiluted doses of oxytocin, including gastrointestinal conditions, transient drop in blood pressure, and water poisoning, were not observed in the participants. The recommended dose for Capsella bursa pastoris in liquid form is 5 to 8 g per day 17 ; in this study, the Capsella group received a 5-g dose of the hydroalcoholic extract of the plant in liquid form and no side-effects were, therefore, observed in the participants, except for one case of sore and itchy throat.
The strengths of this study include the measurement of the amount of bleeding through weighing the pads and drapes by the same assistant researcher, the measurement of hemoglobin and hematocrit levels 6 h postpartum, the monitoring of the participants in terms of bleeding and medication side-effects for 6 h postpartum, giving the routine treatment to both groups, the control of the confounding variables, and the control of vital signs by the same assistant researcher. In addition, the follow-up of the participants continued for 40 days postpartum so as to assess the effect of the intervention on late PPH as well and control the medication side-effects. The results of the 1-month follow-up and the effect of the plant on late PPH will be presented in another article.
The limitations of this study include the researcher's sufficing to the patient's verbal declaration of having no underlying diseases. Moreover, the mother's fatigue and psychologic state are factors that can affect the amount of postpartum bleeding, but they could not be measured or controlled.
Conclusion
The results of this study indicate that the hydroalcoholic extract of Capsella bursa pastoris reduces early PPH. It is also suggested that additional study should be carried out using similar methodology and a larger cohort to confirm these findings. Moreover, further study is required to illustrate reliably that Capsella bursa is the safe and low-cost medication for patients who prefer to use herbal medicine or have some contraindications for chemical drugs. Moreover, additional researches are needed in regard to its relevant active ingredients, safety, efficacy of various doses, and treatment durations.
Footnotes
Acknowledgments
This study is the result of an MSc thesis and research project in Midwifery at Shahid Beheshti University of Medical Sciences in Tehran, Iran. Hereby, the authors would like to express their gratitude to the authorities and professors of Shahid Beheshti University of Medical Sciences for their support, to the School of Pharmacy for preparing the Capsella bursa pastoris drops, and to all the mothers who participated in the research.
Author Disclosure Statement
There are no conflicts of interest to disclose.