
Abstract
Objectives:
GuiZhi-ShaoYao-ZhiMu decoction (GSZD), a traditional Chinese herbal medication for the management of rheumatoid arthritis (RA), has a long history of use and modern scientific research support for efficacy, but the studies have not been systematically evaluated. Therefore, this study systematically reviewed the efficacy of GSZD using the available human clinical trials and conducted a meta-analysis.
Methods:
The available databases were searched using proper languages of English, Korean, and Chinese. The key erms used for searching were “GSZD,” “Cassia Twig,” “Guizhi,” “Paeonia lactiflora,” “Shaoyao,” “Anemarrhena Rhizome,” “Zhimu,” “rheumatoid arthritis,” “randomized,” “controlled trial,” and “clinical trial.” Randomized clinical trials (RCTs) using GSZD were included in the review and meta-analysis. According to heterogeneity, odds ratio and confidence intervals in the pooled RCTs were assessed by a fixed or random model in meta-analysis. Risk of bias was evaluated for all included studies.
Results:
Thirteen RCTs met the inclusion criteria and were included in the meta-analysis. All studies evaluated the efficacy of GSZD for treating RA, but the herbal formulations varied since some studies added herbs to the basic GSZD formulation. However, all formulations contained the essential herbs: Guizhi, Shaoyao, and Zhimu. Each RCT included an experimental group (GSZD with or without Western-style medicine) and a control group (either standard Western-style medicines or placebo). When compared to placebo, the GSZD treatment was found to be three to six times more effective than standard Western drugs for some symptoms. Furthermore, only two studies reported any adverse events associated with the GSZD group, whereas several reported serious adverse events in the control groups.
Conclusions:
The Traditional Chinese Medicine, GSZD, may have equal or superior effectiveness and safety for treating RA compared to Western RA drugs. It should be considered a viable alternative to Western medicine. However, more long-term research is needed in larger patient groups to better establish its safety and efficacy.
Introduction
A
Like other autoimmune diseases, the etiology of RA is not fully understood. The objective of RA treatment is to suppress the overactivity of the immune system and inflammation, thereby relieving the symptoms and delaying the joint damage. 2 The first strategy of RA treatment is to minimize the effects so that no signs or symptoms of active inflammation are observable, thereby inducing remission as early as possible. 5 Drugs used to treat RA include corticosteroids, nonsteroidal anti-inflammatory drugs (NSAIDs), and disease-modifying antirheumatic drugs (DMARDs). 2 Since corticosteroids have adverse effects, 6 they are not appropriate to treat RA. As the second-generation drugs, NSAIDs are commonly used for easing pain and inflammation and the most commonly used prescription NSAIDs are cyclooxygenase 2 (COX-2) inhibitors such as celecoxib. DMARDs, including methotrexate, leflunomide, cyclophosphamide, and biogenics, and Janus kinase inhibitors are specified for RA to reduce the inflammation and overactive immune responses in the joints. 2,6 However, these NSAIDs and DMARDs have some adverse effects and some patients do not respond to these drugs. 6 Natural phenolic compounds, including thymoquinone, resveratrol, hesperidin, curcumin, celastrol, and gambogic acid, can reduce the production of inflammatory mediators and normalize the abnormal immune responses characteristic of RA. 7,8 Thus, the combination of herbs and conventional drugs can lead to the remission of RA.
Some Traditional Chinese Medicines, including GuiZhi-ShaoYao-ZhiMu decoction (GSZD), are accepted as the most prevalent and effective treatments for RA in many Asian countries. 9 GSZD is mainly composed of Ramulus Cinnamomi cassia Presl. (Guizhi), Paeonia lactiflora (Shaoyao), Anemarrhena asphodeloides (Zhimu), Glycyrrhiza uralensis (Gancao), Glycyrrhiza uralensis (Mahuang), Zingiber officinale (Ginger), and Atractylodes macrocephala (Baizhu). The efficacy of GSZD for relieving RA has been confirmed in basic and clinical studies. 9 GSZD is known from the book as follows: “Synopsis of the prescriptions of the golden chamber.”
In RA rats induced with type II collagen, GSZD administration did not reduce the level of type II collagen antibody compared to the control group. However, GSZD intake did decrease tumor necrosis factor (TNF)-α, interleukin (IL)-1, and nitric oxide (NO) in both serum and peritoneal macrophages and it reduces inflammatory cell numbers infiltrating the synovium and the hyperplasia of the synovial lining cells. The swelling index also decreased more than the control. 10 Thus, GSZD alleviates RA symptoms by reducing inflammation, not by preventing the production of type II collagen antibody in RA-induced animals.
In a more recent study using drug target prediction analysis and in in vivo studies in rats with experimentally induced arthritis, Guo et al. 11 confirmed that the active components in GSZD could target TNF-α and also nuclear factor kappa B, and the inhibitor of kappa light polypeptide gene enhancer in B cells, which are known targets for RA. Furthermore, in the experimentally induced arthritic rats, GSZD suppressed the bone destruction by osteoclasts and caused bone restoration by osteoblasts. Overall, the authors found the effects of high-dose GSZD to be comparable to methotrexate treatment in the experimentally induced arthritic rats. Therefore, there is a solid mechanistic rationale for the efficacy of GSZD for treating RA, which is confirmed in experimental animal models. In clinical observations, GSZD has also shown superior efficacy for RA ranging from 87.5% to 95.8% in comparison to those of indometacin, tripterygium glycosides, and prednisone. 3,12 –16 Furthermore, no significant side-effects have been observed for GSZD in several long-term trials in China. However, there have been no systematic reviews about the efficacy and safety of GSZD.
Here, the authors systematically review the relevant human research to elucidate the efficacy and safety of GSZD for RA symptoms. After exploring all randomized clinical trials (RCTs) of GSZD for treating RA, they conducted a meta-analysis from the outcomes of studies using GSZD for treating RA. This is the first systematic review and meta-analysis of RCTs on the efficacy and safety of GSZD for RA.
Methods
Data sources and selection criteria
For the systematic review, all the RCT articles related to GSZD and RA were extracted from the available electronic databases up to December 2016. The following databases were used: PubMed, EMBASE, Cochrane Library, Korean databases such as DBpia, the Research Information Service System (RISS) and the Korean Information Service System (KISS), Chinese medical databases such as the China National Knowledge Infrastructure (CNKI) and the Chinese Scientific Journal Database, and the Indian Medical Journals and the Indian Journals. Dissertations were also included. The search was conducted in the databases using proper languages of English, Korean, and Chinese. The key terms used for searching were “Guizhi-Shaoyao-Zhimu decoction,” “Ramulus Cinnamomi cassia Presl,” “Cassia Twig,” “Guizhi,” “Paeonia lactiflora,” “Shaoyao,” “Anemarrhena asehodeloides,” “Zhimu,” “arthritis,” “rheumatoid arthritis,” “randomized,” “controlled trial,” and “clinical trial.”
RCT evaluation and selection of publications
Two independent reviewers (T.Z. and S.C.) screened the articles using the key words from the databases. The selected articles were identified by the titles and abstracts and the full text of the related articles was retrieved and validated for relevancy to include in the systematic review. The third reviewer (S.P.) independently validated the selected articles. Only RCT studies about GSZD and RA were selected for systematic review. Duplicate studies had been removed. In vitro studies and in vivo studies in nonhuman species were not included for the review. Among human studies, studies published only in abstract form or which included insufficient outcome data, nonclinical trial studies, and studies in which RA was a secondary outcome measure were eliminated. The process of selecting RCT articles is illustrated in Figure 1. Dissertations about RCTs were also included.

Flowchart of the selection process of the randomized clinical trials related to GSZD and rheumatoid arthritis for systematic review. GSZD, GuiZhi-ShaoYao-ZhiMu decoction; RCT, randomized clinical trial.
The RCTs included in the systematic review investigated the efficacy of GSZD for treating RA. In Chinese medicine, the herbal decoction known as GSZD contains the major common herbs such as Cinnamomum cassia Presl., P. Lactiflora, and A. asphodeloides, but the other herbal components were different in each GSZD. Although the ingredients and contents of GSZD herbal treatments were somewhat different, the GSZD medicines with the same major components were included (Table 1). The subjects in each study were instructed not to use any medications or herbs other than those provided by the study during the experimental periods of the RCTs.
p < 0.05; ** p < 0.01; *** p < 0.001.
CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; GSZD, GuiZhi-ShaoYao-ZhiMu decoction; JTI, joint tenderness index; LEF, leflunomide; LGTDG, tripterygium glycosides; MSI, morning stiffness index; MTX, methotrexate; RF, rheumatoid factor.
Eligibility criteria for subjects in the RCTs
Subjects with RA were recruited in all RCTs. They had some inclusion criteria for including subjects. RA patients were between 18 and 65 years, except in one article. 17 Both genders were included in the RCT articles and in the systematic review, but women were the primary gender in all of the RCTs except one RCT. 13 All subjects had RA with mild-to-moderate severity. The severity of RA was defined in the method as inclusion criteria in the RCT studies except one study.
Inclusion criteria for each RCT are summarized by study in Table 1. RA patients were selected with positive rheumatoid factors (RF) and subcutaneous nodules confirmed by X-ray examination in most of the RCT articles. They had at least 1 h of morning stiffness, swelling of three or more joints (wrist, finger, proximal interphalangeal joint), and symmetry joint swelling for over 6 weeks. The subjects had RA for the ranges of 0.5–15 years. Most studies recruited subjects with RA for a relatively short term (average of ≤5 years 3,13 –16,18 –21 ) and subjects in the other studies had RA for long duration (average of >5 years). 17,22,23 The RCTs had some restrictions for the inclusion of subjects according to age and other conditions. All RCTs except one study 17 excluded subjects younger than 18 years and older than 65 years. Subjects with severe RA such as joint deformity and inability to work were excluded. In addition, subjects with severe metabolic diseases such as cardiovascular, liver, kidney, and hematopoietic system, drug allergy, and mental illness were not included. Pregnant or lactating women were also excluded from the RCTs.
Intervention in the RCTs
GSZD was made by boiling the herbal GSZ mixtures for 30 min, after which the herbal mixture was soaked with cold water for 20–30 min. The water extracts were given to the subjects in the experimental group. In seven studies, the experimental group was orally provided only GSZD and the control group was orally administered with pain medicine and/or NSAIDs. 3,12 –14,16,17,22 However, in four studies, the experimental group consumed GSZD and analgesic and/or immunosuppressant medications such as methotrexate (MTX), whereas the control group consumed the RA medicine given in the experimental group plus an extra pain killer. 18 –20,23 In the two groups, the experimental group was orally provided with GSZD plus pain killer or NSAIDs, whereas the control group had the same drugs except GSZD. 15,21
Outcome measures
The symptoms of RA are similar to those of osteoarthritis, but the etiology is different. RA, but not osteoarthritis, is characterized by the presence of RF in the blood, which triggers inflammation leading to joint damage. Thus, subjects were recruited who tested positive for RF in the 13 RCTs. 3,12 –23 Subjects with RA exhibit increased systemic inflammation that was measured by C-reactive protein (CRP) in the blood and erythrocyte sedimentation rate (ESR). 5 CRP, an acute-phase protein, is produced by the liver in response to inflammatory factors released by macrophages and adipocytes. 5 ESR, a rate of red blood cell sediment in a period of 1 h, is a nonspecific measure of inflammation. RA exhibits the following symptoms: pain, joint tenderness, joint swelling, and morning stiffness. 5 The severity of RA was determined by the 2010 American College of Rheumatology and European League Against Rheumatism classification criteria and pain scale. 24 The efficacy of GSZD and drugs was mainly categorized into clinical remission, markedly effective, effective, and ineffective groups at the end of the intervention. After the administration of GSZD and drugs, the doctors decided the efficacy of the treatment in each subject as one of clinical remission, markedly effective, effective, or ineffective categories in all included RCTs. 3,12 –23
In addition, each symptom of RA was scored as a continuous variable. Morning stiffness was measured by the length of time to have stiffness in the morning. The severity of joint tenderness, swelling, and ache was determined by a 10 cm horizontal scale and it was represented by the scores of 0 to 10. Hand grip was measured by pressure (kPa). One or more of these factors related to pain were measured in all studies. 3,12 –23 Among inflammation indices (CRP and/or ESR), the ESR was measured in 11 studies 12 –16,18 –23 and CRP and ESR were determined in eight studies. 12 –14,16,18,19,22,23 All the factors related to inflammation and pain were used as outcome measures for meta-analysis.
Quality assessment of the studies
The quality of studies included in the systematic review was determined by the risk of bias (ROB) designated from the Cochrane tool. 25 The validation for the RCTs was determined by the following eight categories: (1) random sequence generation, (2) allocation concealment, (3) blinding of participants, (4) assessor blinding, (5) reporting dropout or withdrawal, (6) intention to treat, (7) selective outcome reporting, and (8) other potential bias. ROB of each category was scored as H, high ROB, U, uncertain ROB, or L, low ROB. The quality of RCTs was assessed by three independent reviewers (T.Z., S.C. and S.P.). If the reviewers disagreed on scores, they resolved it through discussion.
Data analysis
All 13 publications were included in meta-analysis. 3,12 –23 The outcomes given in the RCTs mainly showed similarities, but all outcomes were not given in all RCTs. The same outcomes in RCTs were pooled. The data used for the meta-analysis were used as categorical and continuous variables of RA symptoms. RA symptoms were objectively evaluated by doctors after the assigned treatment and the efficacy of treatments (either of GSZD or Western-type drugs) in each subject was categorized as “clinical remission,” “markedly effective,” “effective,” or “ineffective.” The number of subjects in each category was used as dichotomous outcomes in meta-analysis to determine which treatment showed better efficacy and the results were represented as odds ratio of GSZD when the control group was the reference. The other continuous outcomes were measurements such as inflammatory indices (CRP and ESR), indices of pain and clinical symptoms (morning stiffness, joint tenderness, joint swelling, and ache), and RF levels. The continuous outcomes were represented as means and standard deviations in each RCT and standard mean differences (SMD) and 95% confidence intervals (CI) were calculated in the pooled RCT meta-analysis using the Cochrane Collaborations software (RevMan Version 5.0 for Windows, Copenhagen: The Nordic Cochrane Centre). The SMD and 95% CI indicated the significant differences of continuous outcomes in pooled data.
According to heterogeneity of RCTs included in the meta-analysis, odds ratio and SMD in the pooled RCTs were assessed by a fixed or random model. The heterogeneity of included RCTs was quantitatively validated with Cochran's Q test of RCTs in meta-analysis. In the Cochran's Q test, the I 2 index represents the degree of heterogeneity in a meta-analysis. I 2 ≤ 25%, 25% ≤ I 2 ≤ 50%, and I 2 > 75% were considered to be low, moderate, and high heterogeneity, respectively. 26 When I 2 value was moderate and high, the random effect model was selected; otherwise, the fixed genetic model was used. However, I 2 was not the only reason to choose the type of model. The heterogeneity was qualitatively validated to consider the heterogeneity of subjects in the included RCTs. In the present review, although the range of age varied among the RCTs, the average age of subjects was about 40–50 and age of subjects indicated low heterogeneity. Subjects in all RCTs were Chinese. However, other factors were somewhat heterogeneous among the RCTs. Both men and women were included as subjects of the RCTs. Subjects had RA for a duration ranging from 1 to 15 years. In addition, the components of GSZD varied in all RCTs although the herbal prescription of GSZD was designated as GSZD. All prescriptions of GSZD contained C. cassia Presl., P. Lactiflora, and A. asphodeloides, but other components were somewhat different. The control group treatments including placebo, other Chinese medicine, and Western-style medicine were different among the 13 RCTs. 3,12 –23 Treatment duration ranged from 4 to 16 weeks. Thus, the RCTs exhibited moderate heterogeneity. Therefore, due to heterogeneity of the subjects in the 13 RCTs, random effect models were better to use when the outcomes were pooled.
Among heterogeneity of 13 RCTs, control treatment should be categorized into three subgroups, such as Western-style medicine, other Chinese medicine plus Western-style medicine, and placebo, since their efficacy cannot be pooled together. In addition, since 13 RCTs used GSZD with some different herbal components, the authors made three subgroups such as using seven basic herbs, basic herbs plus one to three herbs, and modified GSDZ adding and subtracting herbs from the basic herbs. Funnel plots were used to detect publication biases for this systematic review.
Results
Summary of included studies
In the initial electronic search of PubMed, EMBASE, Wanfang, CNKI, RISS, KISS, and IndMED, 97 papers were identified, in that they were related to RA and GSZD. The 16 duplicated articles were eliminated. The authors then checked 81 remaining publications by titles and abstracts and a total of 52 studies were removed: 12 animal studies, 23 Chinese medicine decoction studies but not about GSZD, and 17 nonclinical trials were excluded (Fig. 1). After careful evaluation of the full texts, 16 studies were eliminated due to non-RCT. Eventually, 13 RCTs 3,12 –23 met the inclusion criteria (Fig. 1) and they were used for the systematic review and meta-analysis.
The subject characteristics and intervention treatments of the included RCTs are summarized in Table 1. Subjects had the symptoms of arthritis such as 1-h morning stiffness, three or more joints with swelling, wrist and palm joint swelling over 6 weeks, and they had RF. However, they did not have severe metabolic diseases such as cardiovascular, hepatic, kidney, and hematopoietic diseases and gastrointestinal diseases. In addition, the subjects had no mental illness, allergy, and there were no pregnant or lactating women. Mean age of subjects in the selected RCTs was about 40–50 years, but some young subjects were included. However, the mean age was comparable between the control and experimental groups. Subjects had RA ranging from 0.5 to 15 years in different RCTs, but most of the subjects had RA for more than 1 year. The majority of studies recruited subjects who had RA for a short duration (≤5 years), but three studies recruited subjects with an average duration of >5 years. 17,22,23 Moreover, the duration for RA was similar between the control and treatment groups.
All 13 studies were conducted in China and they had a two-arm parallel design, including GSZD and control group. Since RA needs drugs to alleviate the symptoms, subjects in the control group received Western medicine such as NSAIDs (benorylate, ibuprofen, diclofenac sodium, celecoxib, meloxicam), 12,13,16 –18,21 –23 DMARDs (leflunomide), 15,16 or immune-suppressant drugs (MTX) 3,14,19 –21,23 and they had additional herbal medicine such as total glucosides of Paeony capsules or tripterygium glycosides in some control groups. 19,20,23 Subjects in all of the studies had the prescribed amount of GSZD two or three times a day in the experimental design and they also had either no extra medicine 3,12 –14,16,17,22 or additional medicine for arthritis (MRA). 15,18 –21,23 As a result, the treatment in the control and experimental groups was not matched in all RCTs. GSZD commonly contained 9–20 g C. cassia Presl., 9–15 g P. Lactiflora, 10–30 g A. asphodeloides, and additional other herbs that were different types of herbs and different amounts in each study although the herbal treatments are considered as GSZD in Chinese medicine. The detailed compositions of GSZD in each study are shown in Table 2. In three studies, 16,19,21 only the basic components of GSZD (Cinnamomum cassia Presl., P. lactiflora, A. asphodeloides, Ephedra sinica, Ledebouriella seseloides, A. macrocephala, Aconitum carmichaelii Debeaux, Z. officinale, G. uralensis) were used; in five studies, 13,14,17,18,22 one to three herbs were added into its basic composition; and in the remaining five studies, 3,12,15,20,23 the herbal composition was modified with different herbs according to the condition of subjects included in the RCT. The given prescriptions were extracted in water and subjects took it orally two or three times a day.
Addition or bdeletion of the herb from the basic formula to improve this symptom.
Outcomes
The RA symptoms were mainly pain and inflammation. The clinical symptoms were classified as pain, stiffness, tenderness, swollenness, impaired movement in the wrist, finger, proximal interphalangeal joints, and grip power and inflammation index were CRP and ESR. In addition, RF levels were also an index of RA. These outcomes at the end of treatment are presented in Table 1. The clinical symptoms in all RCTs except one RCT 23 were represented by severity using scores similar to visual analogue scores. The effectiveness of treatments was determined by meta-analysis of each symptom. In addition, in all 13 RCTs, 3,12 –23 doctors evaluated the changes in RA symptoms in each subject at the end of treatment and classified the efficacy of the treatment as “remission” if any, “markedly effective,” “effective,” and “ineffective.” The number of subjects and the percentage of subjects in each category are given in Table 1. The numbers of subjects in remission, markedly effective, and effective categories were summed and the number was used for meta-analysis.
Since the types of treatments in the control and experimental groups were not homogeneous, the RCTs were divided into three subgroups: GSZD versus MRA for RA(MRA), 3,12 –14,16,17,22 GSZD + MRA1 versus MRA2 + MRA1, 18 –20,23 GSZD + MRA1 versus MRA1. 15,21 Each symptom and inflammation index were compared between the control and experimental groups in all RCTs and each subgroup by meta-analysis (data not shown). In pooling all the RCTs, effectiveness of GSZD, as decided by doctors, at the end of experiment was better in the GSZD group by 3.15-folds (CI: 1.78–5.59; p < 0.0001) than the control group in subgroup 1 (GSZD vs. MRA). The GSZD efficacy was also greater by 3.3-folds (CI: 1.1–10.07; p = 0.03) than the control group in subgroup 2 (GSZD + MRA1 vs. MRA2 + MRA1) (Fig. 2). However, the efficacy of GSDZ was not significantly different from the control group in subgroup 3 (GSZD + MRA vs. MRA). In some studies that administered only GSZD treatment in the experimental group, 3,16,17,22 clinical remission occurred in both control and experimental groups and the remission rate was slightly higher in the GSZD group than the control group (Fig. 2A). These results suggested that GSDZ may have sufficient efficacy to alleviate or cure RA symptoms in some people.
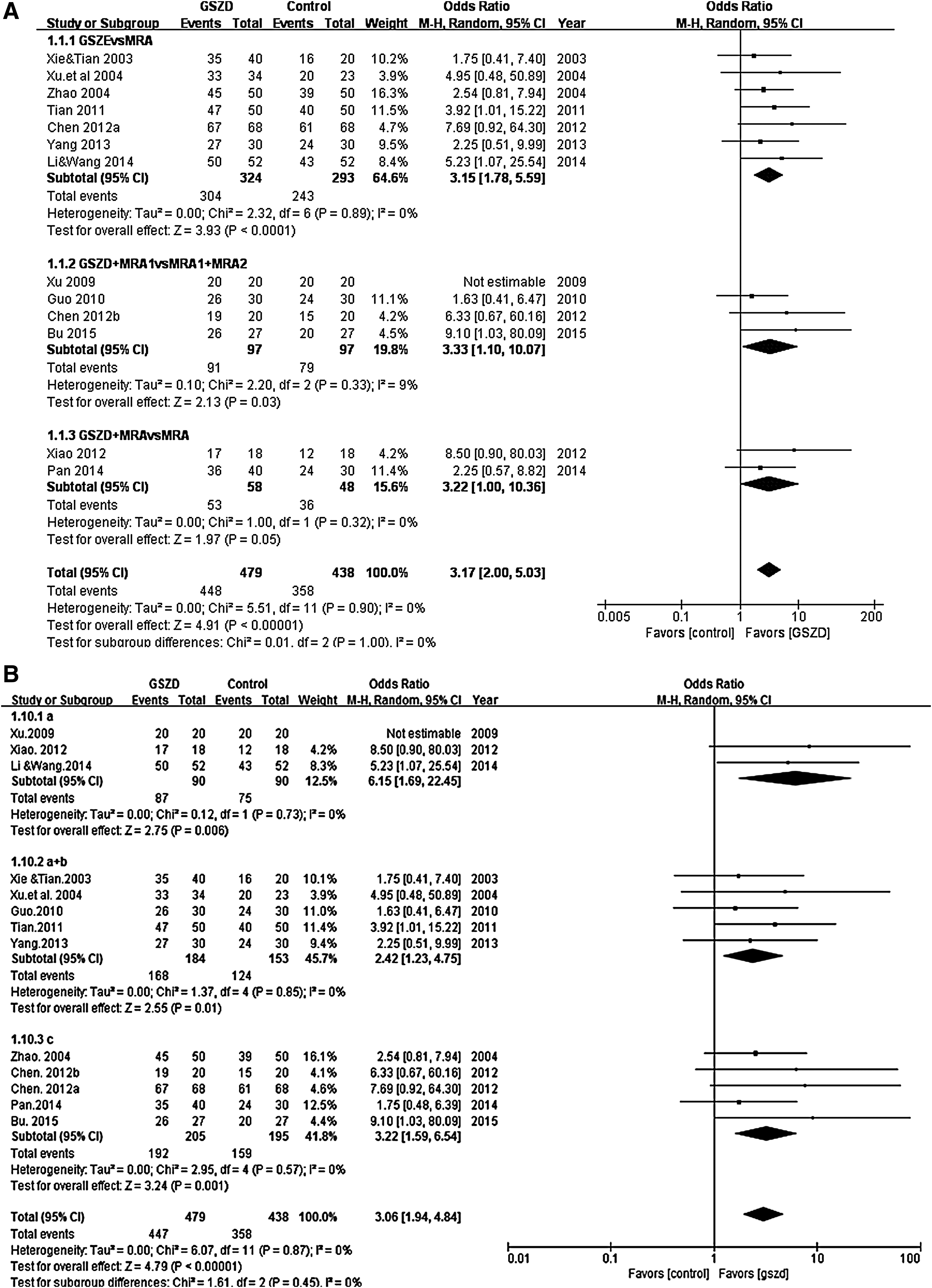
Forest plot of the meta-analysis for the effectiveness of GSZD on rheumatoid arthritis.
When RCTs were divided by composition of GSZD, the basic form of GSZD exhibited better effectiveness by 6.15-folds (CI: 1.69–22.45; p < 0.006) in three RCTs 16,19,21 and the basic form plus 1–3 more herbs also improved the effectiveness by 2.42-folds (CI: 1.23–4.75; p = 0.01) in five RCTs 13,14,17,18,22 (Fig. 2B). Modified GSZD treatments also showed favorable results in the GSZD groups in comparison to the control groups by 3.22-folds (CI: 1.59–6.54; p = 0.001) in the pooling of five RCTs. 3,12,15,20,23 The overall effect of pooling 13 RCTs enhanced the reported effectiveness of the GSZD treatment by 3.06-folds (CI: 1.94–4.84; p < 0.00001). From the subgroup analysis, the difference in the subgroups was not significant (p = 0.45; Fig. 2B). Thus, all basic and modified GSZD formulations showed similar effectiveness for RA symptoms.
GSZD increased the number of subjects in the markedly effective group and it was associated with the improvement of RA symptoms. Table 3 shows the summary of meta-analysis for RA symptoms such as inflammatory index (CRP and ESR), clinical observation (morning stiffness, swelling index, joint tenderness, ache index, and grip power), and RF. CRP and ERS levels were not significantly different between GSZD and drug, whereas they decreased in GSZD + MRA1 in comparison to MRA1 + MRA2 (Table 3). The results indicated that inflammation was reduced by GSZD itself as much as by drug treatment and GSZD exhibited synergistic improvement when combined with drug to reduce inflammation due to RA. Clinical symptoms such as morning stiffness, swelling, and pain were significantly reduced with GSDZ treatment in comparison to the controls (mainly Western-type drugs) (Table 3). However, RF and grip power were not significantly different between the GSZD and control groups (Table 3). These results indicated that GSZD improved RA symptoms by reducing inflammation but not RF.
Standard mean differences from pooled randomized clinical trials (confidence intervals).
p-Value for overall effects in each group comparison. Subgroup 1: GuiZhi-ShaoYao-ZhiMu decoction (GSZD) versus Western-type medicine for arthritis (MRA). Subgroup 2: GSZD + MRA1 versus MRA1 + MRA2. Subgroup 3: GSZD + MRA versus MRA.
Adverse events
Eight RCTs 3,12 –16,18,20 reported adverse effects in some subjects in the control groups who were taking MRA. The adverse effects were similar to those reported in other studies: gastrointestinal discomfort, liver damage, mouth ulcer, nausea, diarrhea, dizziness, stomach discomfort, rash, irregular menstruation, and gastrointestinal discomfort. However, only two RCTs 3,18 reported adverse effects in the experimental group of GSZD: the RCT by Guo 18 indicated two incidences of anorexia, two incidences of nausea, one instance of a subject with liver damage, and two incidences of irregular menstruation, and the RCT by Chen 3 reported one subject with gastrointestinal discomfort. Other RCT studies did not report any adverse effects from the experimental treatment. Furthermore, in the RCT from Guo, 18 it was difficult to tell if the adverse effects were due to GSZD since the experimental group had GSZD plus diclofenac sodium. Thus, the dosage of GSZD indicated a minimal adverse effect in comparison to MRA up to 20 weeks.
Risk of bias
ROB for the included RCTs is shown in Figure 3. Overall, more than sixty percent of the studies exhibited low ROB, and some studies had a blindness of personnel and high rates of dropouts (Fig. 3A). In each RCT, most of the studies included in the meta-analysis showed a proper randomization method, including coin flipping and random numbers, but in two studies, 3,14 the randomization method was not clear (Fig. 3B). The concealment of allocating the groups was reported in the nine articles but not in four RCTs. 19 –21 Eight RCTs had blinding of patients and practitioners in their studies, whereas two studies were not blind to patients and practitioners 3,17 and three studies did not conduct blinding of outcome assessment or did not describe the blindness 17,18,22 (Fig. 3B).

Summary of risk of bias in 13 RCTs.
Publication bias
The funnel assay showed asymmetric funnels indicating some publication bias for the RCTs (Fig. 4). However, the publication bias may not be big, since the meta-analysis included more than 10 RCTs.

Funnel plot of the meta-analysis for the effectiveness of GSZD on rheumatoid arthritis.
Discussion
The Chinese medicinal formula, GuiZhi-ShaoYao-ZhiMu, translated in English means “Cinnamon twig, Peony, Anemarrhena,” the essential herbs in the formula. 20 However, various pharmacies and Chinese medical doctors will add other herbal medicines to the basic formula based on their experience and needs of a patient. However, for most part, this study did not differentiate between the different formulations as long as they contained the essential three ingredients with the same name of prescription. Accordingly, the 13 studies 3,12 –23 that are part of this meta-analysis and systematic review used several variations on the basic medicinal formula. Overall, RA treatment with GSZD was more than threefolds more effective than using just the drug therapies or placebos in meta-analysis. GSZD has been the subject of numerous studies in humans and animals. For the meta-analysis, the authors were able to identify 13 RCTs that met all of the inclusion criteria. Most of the studies were small but of relatively high quality with low or moderate ROB. However, because the number of studies included was sufficient, combining the studies by meta-analysis provided valuable insight into how GSZD compares to standard treatments used in Western medicine.
When evaluating specific symptoms, GSZD was significantly more effective for morning ache index, stiffness, and joint swelling, but not for joint tenderness. Furthermore, ESR, one of inflammatory index, was decreased, but RF and CRP were not significantly improved by GSZD. Therefore, GSZD appears to be highly effective for the RA treatment, but the mechanism is not quite clear and it appears to block the inflammatory cascade somewhere subsequent to the action of RF. GSZD seemed more effective for reducing inflammation than reducing RF from the RCTs included in the systematic review.
Asian traditional medicines have a well-documented record of treatment of chronic diseases of the aging. The Indian herb, turmeric, has been well studied and demonstrated to be effective for osteoarthritis, with efficacy and safety being comparable or superior to those of Western medicines in some studies. 25 The major active ingredient in turmeric, curcumin, appears to act by inhibiting several targets in the inflammatory process, including nuclear factor kappa B (NF-κB), TNF-α, and mitogen-activated protein kinase (MAPK). 25,27 This may be a similar mechanism to that of GSZD, although it remains to be determined.
Currently used Western medicines for treating rheumatoid diseases have well-documented adverse side-effects. NSAIDs are associated with severe gastrointestinal injury and some of the newer COX-2 inhibitors have been found to cause severe cardiovascular toxicity. 28 In this study, there were only two studies that reported any adverse effects with GSZD treatment 3,18 : only one subject (1.5%) showed gastrointestinal discomfort from GSZD in one RCT 3 and in the other RCT, 18 GSDZ was given with diclofenac sodium. The adverse effect in the Guo study 18 may have been due to the administration of analgesic drugs and not the GSZD. However, caution is needed in suggesting that GSZD is much safer than other drugs based on the limited observations in these studies.
There were several limitations of this study that must be considered when interpreting the results. All of the studies were of relatively short duration, 3–16 weeks, and that may not be sufficient time for some adverse effects to be revealed. Another major limitation of the study is the diverse composition of the formulas. Although all studies used the basic GSZD formulation, other herbs were included that may have affected the efficacy, and more studies are needed to compare the safety and efficacy of different formulations. Finally, although overall ROB was not high, the risk of publication bias was high enough to be of some concern. Despite the limitations, this study has important merits and the results remain convincing because the studies very consistently showed a high degree of efficacy for GSZD treatment. Furthermore, this is the first systematic review to determine the efficacy of GSZD for treating RA. This study included 13 RCTs that studied the effects of GSZD treatment on RA, and the total sample sizes of control (n = 438) and experimental (n = 479) groups was quite large. Most of the studies were conducted to determine the efficacy of GSZD for treating symptoms and used scientifically validated methods for measuring biochemical indices for RA such as CRP, ESR, and RF as well as clinical indices for measuring relief from symptoms. In subgroup analysis, GSZD also had a beneficial effect on RA when combined with other drug treatments and it did not have side effects. GSZD alone seemed to improve the symptoms of RA better than GSZD plus MRA although there were fewer studies using GSZD plus MRA than GSZD alone.
In conclusion, this meta-analysis showed that the Traditional Chinese Medicine, GSZD, is both safe and effective for the management of RA symptoms and compares favorably with the standard Western drugs. All of original and modified GSZD formulations had a similar beneficial efficacy for treating RA symptoms. GSZD should be considered a viable alternative to Western medicine. However, since each RCT included a rather small sample size with short-term treatments and had a ROB and publication bias, the strength of the evidence may be limited. Furthermore, it is difficult to determine whether GSZD and Western-type drugs have beneficial additive effects on RA symptoms since only a few studies compared GSZD plus MRA with MRA alone. Therefore, more long-term research of GSZD with and without MRA is needed in larger patient groups to better establish its safety and efficacy. However, despite the limitations, this study provided convincing evidence that the Traditional Chinese Medicine, GuiZhi-ShaoYao-ZhiMu (GSZD), is a safe and effective intervention for treating RA.
Footnotes
Acknowledgment
This research was supported by grants from the National Research Foundation (NRF-2015R1D1A3A01019577).
Author Disclosure Statement
James W. Daily III of Daily Manufacturing, Inc., manufactures dietary supplements which could be considered a conflict of interest even though they do not manufacture Chinese medicinal formulations. Other authors have no competing financial interests.