
Abstract
Background:
Cardiovascular disease is a common health problem resulting from many factors, including dyslipidemia. T'ai chi is one of the interventions assigned to improve lipid profiles and other physical outcomes. However, conflicting results might be attributed to different study designs and interventional approaches. A systematic review and meta-analysis are needed to evaluate existing evidence.
Objective:
The aim of this systematic review and meta-analysis is to evaluate existing randomized clinical trials (RCTs) regarding the overall effect of t'ai chi exercise on lipid profiles.
Methods:
Electronic databases (MEDLINE and Cumulative Index to Nursing and Allied Health Literature) were searched. The authors included only English peer reviewed published RCTs that used a t'ai chi intervention and high-density lipoprotein cholesterol (HDL-C) as the primary outcome along with low-density lipoprotein cholesterol (LDL-C) and/or total cholesterol (TC) as secondary outcomes.
Results:
The authors identified 37 potentially eligible studies. Only eight RCTs were eligible for their qualitative review, and seven studies were eligible for meta-analysis. The included studies were rated as having a low risk of bias. Despite the overall low risk of bias, all studies failed to blind participants to group assignment and were generally unclear about whether they were selectively reporting data. A fixed effect model (I 2 = 38.16%) demonstrated a small positive effect of t'ai chi on HDL-C (Cohen d = 0.12; standard error [SE] = 0.067; p = 0.037). A random effect model demonstrated a medium effect and small effect for LDL-C (Cohen d = 0.47; SE = 0.347; p = 0.089) and TC (Cohen d = 0.34; SE = 0.225; p = 0.066), respectively.
Conclusion:
T'ai chi may potentially be beneficial on lipid profiles across different age groups and populations. Although there were conflicting results regarding the effect of t'ai chi on lipid profiles, the majority of studies had at least a small positive effect indicating a potential positive effect of t'ai chi on HDL-C, LDL-C, and/or TC. Therefore, further research is needed to confirm the small positive effect of t'ai chi on lipid profiles found in this review.
Introduction
C
Previous research has shown an inverse relationship between levels of HDL-C and CVD risk. For example, a high level of HDL-C was associated with decreased incidence of CVD, as well as mortality rate. 3,4 In addition, a decreased level of HDL-C has been shown to be a strong predictor of CVD regardless of wide range of LDL-C levels even below the normal level. 5 –7 In a population-based study, a decrease of 5 mg/dL in HDL-C was associated with a 25% increased risk of myocardial infarction. 8 Furthermore, low levels of HDL-C, regardless of other lipid profiles, were strongly associated with coronary heart disease events in an Asian population. 9 The benefits of increased HDL-C included a longer period of time without CVD, 10 maintenance of endothelial functions, 11 LDL-C oxidation protection, 12 and inflammation protection. 13 Thus, HDL-C is one of the significant targets for any intervention in managing CVD risk.
In addition to the link between HDL-C and CVD risk, LDL-C and total cholesterol (TC) are also related to CVD risk. Increased levels of LDL-C and TC are both shown to be related to increased CVD risk. 14,15 In regard to LDL-C, previous research has shown an association between high levels of LDL-C and CVD. 16,17 A previous study examined the link between dyslipidemia, including LDL and mortality rate, and this study found an independent association of mortality and blood cholesterol concentration. 16 Another recent study investigated the impact of exposure to low levels of LDL-C on coronary heart disease. 17 This study demonstrated that the exposure to low levels of LDL-C in early life was associated with a substantially decreased risk of coronary heart disease. 17 In regards to TC, multiple studies have demonstrated the link between TC and components of CVD. One study found TC to HDL-C ratios to be good predictors of negative cardiovascular events, 18 which translate to CVD risk. While high levels of TC are not optimal, the risk of high TC levels is dependent upon various factors within individuals. For example, high TC levels are only linked with coronary heart disease for women who are premenopausal or who have relatively high levels of TC (e.g., >265 mg/dL). 19,20 While the diagnostic circumstances rely on more than LDL-C and TC, efforts are generally taken to reduce LDL-C and TC levels given that CVD risks tend to decline with lower levels of LDL-C and TC. 14,15 Therefore, LDL-C and TC are two additional targets when attempting to manage CVD risk.
T'ai chi is one of the exercise forms involving rhythmic body movement, meditation, and deep breathing with several benefits on body systems. 21,22 The integration between body and mind may promote the self-healing, release of neuro-hormones, and facilitation of health-recovery mechanisms inside their body. 23 Previous research has shown t'ai chi's beneficial effects in improving balance, 24 muscle strength, 25 stress response, 26 and cardiorespiratory fitness. 27 T'ai chi is an effective intervention in managing hypertension 28 and diabetes, 29 which both increase the risk of CVD. However, the mechanism of t'ai chi in managing risks of CVD is still unknown. Some researchers suggested that meditation might distract attention to stress 30 or that physical expenditure might reduce stress. 31 Reduction in stress response has been linked to reduction in carotid atherosclerosis and hypertension. 32,33 Other researchers investigated the effect of t'ai chi exercise on lipid profiles as CVD risk factors in randomized clinical trials (RCTs) and reported various results. 34 –36 A previous study examined the effect of t'ai chi exercise in obese individuals with diabetes. 37 The exercise program was a 1-h supervised session of t'ai chi, three sessions a week for 12 weeks. This study found significant improvements in levels of LDL-C, HDL-C, and triglycerides (TGs) compared to the control group. Another study in people with borderline hypertension reported similar findings in terms of lipid profiles. 36 The exercise group performed t'ai chi exercise for 50 min per session, three sessions a week for 12 weeks. Their results revealed significant decreases in LDL-C and TC along with a significant increase in HDL-C, indicating that t'ai chi was effective for improvement in lipid profiles.
A few systematic reviews have examined the effect of t'ai chi on lipid profiles. Wang et al. 38 reviewed the effect of traditional Chinese exercise on physiologic and biochemical outcomes, physical function, quality of life, and depression in people with CVD. The review included 35 clinical studies and found that traditional Chinese exercises such as t'ai chi, qigong, or baduanjin have positive effects on blood pressure, HDL-C and LDL-C, physical function, quality of life, and depression. Of these 35 studies, six studies examined changes in HDL-C and observed an overall increase in HDL-C after the exercises in people with CVD. A limitation of this review was that it did not evaluate the effect of each form of exercise separately since t'ai chi may be closer to a form of aerobic exercise 39 than qigong or baduanjin. 40 Another meta-analysis assessed the effect of t'ai chi on lipid profiles in people with dyslipidemia. 41 Their review included six clinical trials that evaluated any lipid profile (e.g., LDL-C, HDL-C, TC, TG). Five of those trials examined the effect of t'ai chi on HDL-C. The TG was the only variable that showed significant changes in the t'ai chi group compared to the control after t'ai chi exercise. In general the overall benefits of t'ai chi on lipid profile are still unclear.
Few systematic reviews examined the effect of t'ai chi as secondary prevention of CVD risk in people with coronary heart disease 42 or CVD. 43 It is of public interest to review and summarize results of clinical trials on the effect of t'ai chi on lipid profiles, including HDL-C due to their strong association with CVD risk and cardiovascular health. The objective of the current systematic review and meta-analysis is to evaluate current research evidence regarding the overall effect of t'ai chi exercise on lipid profiles, especially HDL-C as a primary outcome and LDL-C and/or TC as secondary outcomes.
Methods
Protocol and registration
The protocol for this systematic review was registered prospectively in the PROSPERO database with the registration number CRD42016036120 that is available online:
Data source and search strategy
A comprehensive literature search was conducted using MEDLINE and Cumulative Index to Nursing and Allied Health Literature databases up to May 16, 2017 to identify eligible studies. The search process used the following terms: “(“tai ji”[MeSH Terms] OR (“tai”[All Fields] AND “ji”[All Fields]) OR “tai ji”[All Fields] OR (“tai”[All Fields] AND “chi”[All Fields]) OR “t'ai chi”[All Fields]) AND (“lipoproteins”[MeSH Terms] OR “lipoproteins” [All Fields] OR “lipoprotein”[All Fields]).” The search was limited to adults, clinical trials, and studies published in English. All identified articles were screened by title, abstract, and full text to determine their eligibility based on the following inclusion criteria: • Design: RCT. • Participants: Samples that include both males and females. These individuals may have chronic diseases, such as CVD or diabetes that do not limit their ability to exercise or perform t'ai chi exercise, or the individuals may be physically inactive middle aged adults or older adults whose lipid profile may be altered due to inactive lifestyle. • Intervention: T'ai chi exercise or a related type of exercise such as t'ai chi chuan; other forms of exercise such as qigong were excluded. • Comparison: Other type of exercise, usual care, sham or control. • Outcome measures: Lipoproteins or lipid profiles that include HDL-C as one of the outcomes.
Quality assessment
Two reviewers independently evaluated included studies. When the reviewers had a conflict, a third independent reviewer evaluated the studies, and his rating was final. Included articles were assessed for risk of bias using Cochrane risk of bias tool, including random sequence generation, allocation concealment, blinding of subjects and personnel, blinding of assessors, incomplete data, selective reporting, and other sources of bias. Level of evidence is also classified based on level I and level II of evidence. 44 Level I is defined as being supported by at least one large-scale RCT with clear results and low risk of error. Level II is defined as being supported by at least one small RCT with uncertain results and moderate-to-high risk of error. 45
Results
Qualitative description of included studies
The authors' initial search found a total of 37 articles from the databases, and four additional articles were found from other sources (e.g., meta-analyses, systematic reviews). After removing duplicate articles, title screening, and abstract screening, the authors found 19 studies for initial review. The detailed search process is shown in Figure 1. A total of eight RCTs were included based on the selection criteria and quality assessment. 34 –37,46 –48 Table 1 summarizes the characteristics of all included studies such as the design, participants, intervention, outcome variables, and main findings. The number of participants in each study ranged from 21 to 372. Five studies included two groups, 35 –37,48,49 and three studies included three groups. 34,46,47
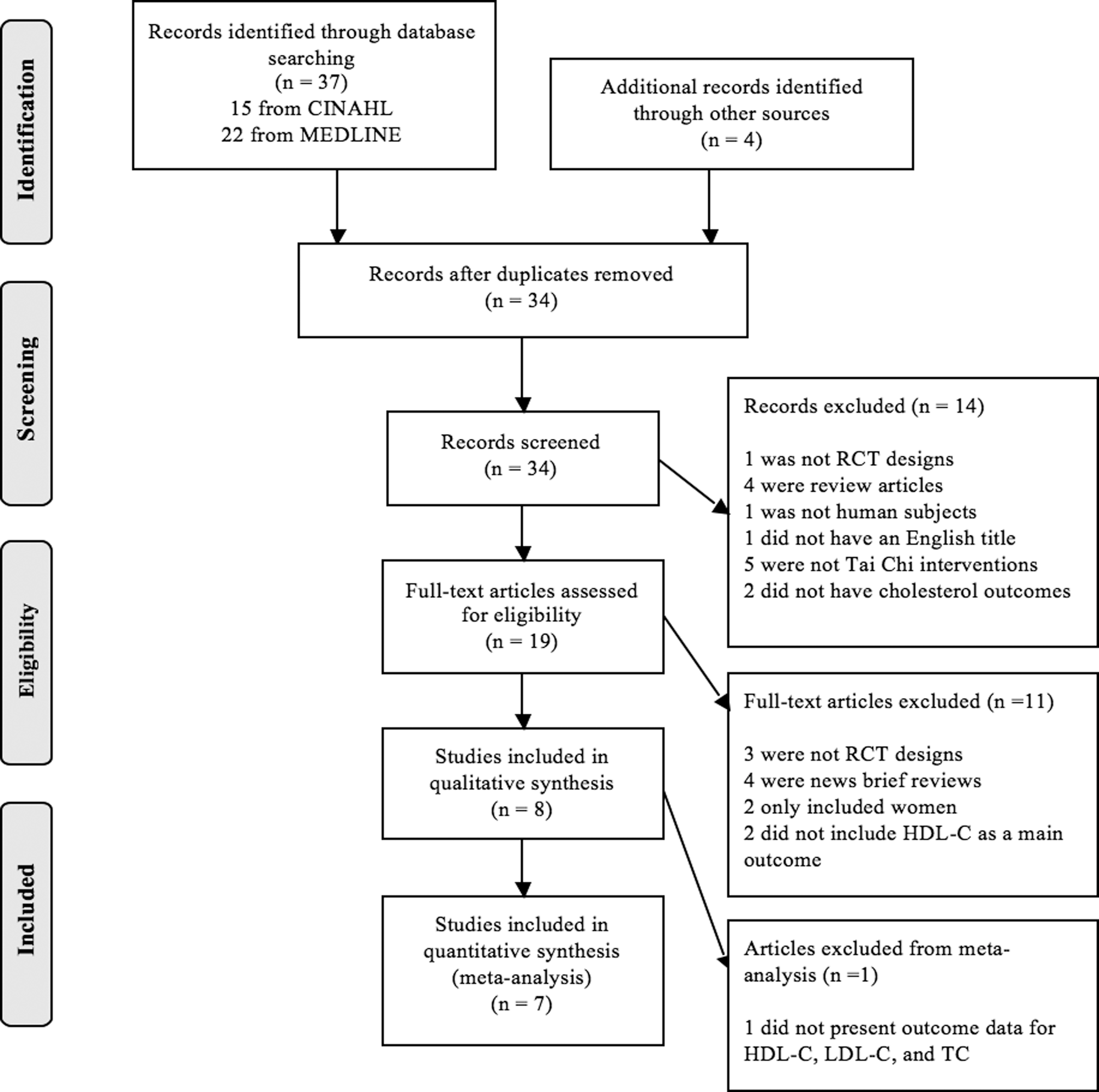
Flowchart for article selection process.
RCT, randomized clinical trial; CVD, cardiovascular disease; BMI, body–mass index; LDL, low-density lipoprotein; HDL, high-density lipoprotein; TG, triglyceride; TC, total cholesterol; BP, blood pressure; FBG, fasting blood glucose; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; Scr, serum creatinine; eGRF, estimated glomerular filtration rate; PSQI, Pittsburgh Sleep Quality Index; CRP, C-reactive protein; FFQ, Food Frequency Questionnaire; BMD, bone mineral density; BUN, blood urea nitrogen; CH, cholesterol; SBP, systolic blood pressure; DBP, diastolic blood pressure; VLDL, very low-density lipoprotein; HgA1C, glycosylated hemoglobin; FVC, forced vital capacity; FEV1, forced expiratory volume in the first second; MABP, mean arterial blood pressure; CBT, cognitive behavioral therapy; TCC, t'ai chi chih; SS, sleep seminar; TCE, t'ai chi exercise; CE, conventional exercise; HRQOL, health related quality of life.
The primary diagnoses and populations were different among the studies. Two studies included participants with hypertension, 35,36 one study included patients with primary insomnia, 46 one study included middle-aged inactive adults, 47 one study included patients with chronic kidney disease and CVD, 48 one study included patients with diabetes and obesity, 37 one study included Chinese healthy older adults, 34 and one study included Taiwanese healthy adults over the age of 45. 49
Despite focusing on different diagnoses and populations, all of the included studies focused on t'ai chi exercise as the intervention and assessed HDL-C as one of the outcome measurements. Two studies performed t'ai chi exercise for 12 months, including breathing, balance, and flexibility exercises. 34,35 One study performed t'ai chi exercise for 4 months, including slow-paced movements designed to learn control over physical function and arousal. 46 Four studies performed t'ai chi exercise for 3 months. 36,37,47,49 One study performed t'ai chi for 4 weeks with supervision followed by 8 weeks of home-based t'ai chi exercise. 48 Seven studies utilized usual care, educational sessions, nonexercise related activities, or maintained usual lifestyle for the control groups. 34 –36,46 –49 One study did not have a control group, but it had aerobic exercise group. 37
The following subheadings show the results from five reviewed studies which significantly improve the HDL-C, LDL-C, and TC after t'ai chi exercise in both within-group and between-group differences. 36,37,46,48,49
Effect of t'ai chi on HDL-C: qualitative and meta-analysis
The majority of the included studies showed some improvements in HDL-C, even though some of those results were not statistically significant. Although Carroll et al. 46 did not report scores for HDL-C in their study, they reported improvement in HDL-C after intervention. Shi et al. 48 reported significant improvement in HDL-C after t'ai chi exercise (p < 0.05), with small effect (Cohen d = 0.13). 50 Hui et al. 47 reported no significant improvement in the HDL-C for t'ai chi group, small effect size (Cohen d = 0.25). Chen et al. 37 reported significant improvement in HDL-C for the t'ai chi group compared to the aerobic exercise group after treatment (p = 0.043), with large effect size (Cohen d = 0.21). Sun and Buys 35 showed no significant improvement in the HDL-C (p = 0.18) after a 12-month intervention program. Tsai et al. 36 reported significant improvement (p < 0.05) in HDL-C in the t'ai chi group compared to the control group, with a medium effect size, Cohen d = 0.60. Thomas et al. 34 reported no significant difference between groups in HDL-C (p = 0.24), with small effect size of the t'ai chi intervention compared to control, Cohen d = 0.30. Lu and Kuo 49 reported no significant difference between groups regarding HDL-C, with small effect size (Cohen d = 0.24). The results of the meta-analysis indicated that there was a generally positive effect of t'ai chi on HDL-C. A fixed effect model (I 2 = 38.16%) demonstrated a small but positive effect of t'ai chi on HDL-C (Cohen d = 0.12; standard error [SE] = 0.067; p < 0.05). Figure 2 displays the results of the meta-analysis along with the upper and lower bounds for the effect size estimates for HDL-C.

Forest plot for the effect of t'ai chi interventions on high-density lipoprotein cholesterol.
Effect of t'ai chi on LDL-C: qualitative and meta-analysis
The majority of the included studies showed improvements in LDL-C. While some of these improvements were relatively small, 34,47 some were actually quite large, 36,48 which provides evidence supporting the effectiveness of t'ai chi interventions in respect to improving LDL-C levels. Shi et al. 48 reported significant improvement in LDL-C after t'ai chi exercise (p < 0.05), with large effect size (Cohen d = 0.83). 50 Hui et al. 47 reported no significant improvement in the LDL-C for t'ai chi group, with large effect size (Cohen d = 0.99). Chen et al. 37 reported significant improvement in LDL-C for the t'ai chi group compared to the aerobic exercise group after treatment (p = 0.043), without reported scores. Sun and Buys 35 showed no significant improvement in the LDL-C (p = 0.3) after a 12-month intervention program. Tsai et al. 36 reported large effect size of LDL-C in the t'ai chi group compared to the control group (Cohen d = 1.42). Thomas et al. 34 reported no significant difference between groups in LDL-C (p = 0.26), with higher effect size in the t'ai chi group compared to the control group (Cohen d = 0.30). Lu and Kuo 49 also reported no significant difference between groups regarding LDL-C, with effect size Cohen d = −0.55. The results of the meta-analysis indicated that there was a generally positive effect of t'ai chi on LDL-C. A random effect model demonstrated a medium effect and small effect for LDL-C (Cohen d = 0.47; SE = 0.347; p = 0.089). Figure 3 displays the results of the meta-analysis along with the upper and lower bounds for the effect size estimates for LDL-C.

Forest plot for the effect of t'ai chi interventions on low-density lipoprotein cholesterol.
Effect of t'ai chi on TC: qualitative and meta-analysis
The majority of the included studies showed improvements in TC. Only Chen et al. 37 or Lu and Kuo 49 found a relatively small or negative effect size for TC, respectively. While some of these improvements were relatively small, 34,47 some were actually quite large, 36,48 which provides evidence supporting the effectiveness of t'ai chi interventions in respect to improving TC levels. Shi et al. 48 reported significant improvement in TC after t'ai chi exercise (p < 0.05), with large effect size (Cohen d = 0.76). 50 Hui et al. 47 reported no significant improvement in the TC for t'ai chi group, with small effect size (Cohen d = 0.33). Chen et al. 37 reported significant improvement in TC for the t'ai chi group compared to the aerobic exercise group after treatment (p = 0.043), with large effect size (Cohen d = −0.08). Tsai et al. 36 reported large effect size of TC in the t'ai chi group compared to the control group (Cohen d = 1.27). Thomas et al. 34 reported no significant difference between groups in TC (p = 0.56), with higher effect size in the t'ai chi group compared to the control group (Cohen d = 0.1). Lu and Kuo 49 also reported no significant difference between groups regarding TC, with small effect size (Cohen d = 0.26). The results of the meta-analysis indicated that there was a generally positive effect of t'ai chi on TC. A random effect model demonstrated a medium effect and small effect for TC (Cohen d = 0.34; SE = 0.225; p = 0.066). Figure 4 displays the results of the meta-analysis along with the upper and lower bounds for the effect size estimates for TC.

Forest plot for the effect of t'ai chi interventions on total cholesterol.
Quality review
Table 2 shows the results of the risk of bias assessment for the included studies. All of the studies 34 –37,46 –49 (n = 8, 100%) were rated as low risk for random sequence generation bias. Allocation concealment was unclear in three of the studies 35,37,48 (38%), but allocation concealment was rated as low risk in four of the studies 34,36,46,47,49 (50%). All of the studies 34 –37,46 –49 (n = 8, 100%) failed to blind the participants to their group assignment status. Five of the studies 35,46 –49 (63%) had a low risk of bias due to whether assessors were blinded. Three of the studies 34,46,47 (38%) demonstrated low risk of presenting incomplete outcome data. Five of the studies 35 –37,48 (63%) were unclear regarding their risk of incomplete outcome data bias, primarily by failing to present how they addressed missing data. All of the studies 34 –37,46 –49 (n = 8, 100%) were unclear regarding whether they selectively reported data. Five of the studies 34 –36,46,49 (62%) demonstrated a low risk regarding potentially biasing factors, while the remaining three studies 37,47,48 (38%) demonstrated a high risk for potentially biasing factors.
Level of evidence
The level of evidence of the included studies ranged from level I to level II as shown in Table 1. All of the reviewed studies were RCTs with at least two groups (t'ai chi and either control or other intervention). Three level I studies were RCTs with large sample sizes, lower bias, and assessors blinded. 35,46,47 The other five studies presented level II evidence with small sample sizes and/or higher bias. 34,36,37,48,49 All reviewed studies implemented t'ai chi interventions that were 12 weeks in length or longer. However, the length of follow-up differed between studies ranging from 12 weeks after the intervention to 12 months after the intervention.
Discussion
The objective of this systematic review was to evaluate studies that examined the overall effect of t'ai chi exercise on lipoprotein profiles, including HDL-C as a main outcome and LDL-C or TC as secondary outcomes. Eight articles were found in the literature that examined the effect of t'ai chi exercise on lipoprotein profiles. The majority of these studies were published in the last 6 years, which indicates a growing interest in the effect of t'ai chi on risk factors for CVD such as lipoprotein profiles. The quality of the reviewed studies was good for the majority of studies, including randomized design, blinding assessors, monitored intervention, and accounting for all subjects in the final analyses.
Interventions in the included studies focused on t'ai chi exercise in one group and another form of exercise or educational sessions in the other group(s). The duration of intervention differed across studies ranging from 3 to 12 months of weekly t'ai chi exercise sessions. In addition, the targeted populations were different and included hypertension, insomnia, inactive individuals, chronic kidney disease, type 2 diabetes, and healthy older adults. Because of the differences in populations, control groups, and intervention characteristics, heterogeneity of the included studies may limit the interpretation of the results.
The results from the meta-analysis demonstrate that t'ai chi interventions have a positive effect on lipid profiles. Although the results for HDL-C (Cohen d = 0.12), LDL-C (Cohen d = 0.47), and TC (Cohen d = 0.34) may be viewed as having small effect sizes, they may all indicate clinically significant improvement. Taken together, these results suggest that t'ai chi may have a demonstrably positive effect across populations on LDL-C and TC and a somewhat positive effect across populations on HDL-C.
As stated in the results, the SEs of the effect size estimates were 0.067, 0.347, and 0.225 for HDL-C, LDL-C, and TC, respectively. While the SE estimate for HDL-C was rather small, the somewhat larger SE estimates for LDL-C and TC indicated that there was increased variability between the effect sizes in these variables. Additional research could further specify which components of the t'ai chi interventions are positively impacting the outcomes so that future interventions can reduce the variability in the outcomes. In sum, the results of this meta-analysis demonstrate the positive impact of t'ai chi on HDL-C, LDL-C, and TC. Future research may figure out which component of t'ai chi intervention is generating these positive effects.
Although four studies reported improvement in HDL-C after t'ai chi intervention, 36,37,46,48 four studies reported no significant change in HDL-C. 34,35,47,49 Improved HDL-C might be partially attributed to change in diet as reported by Chen et al. 37 However, Tsai et al. 36 reported the improved HDL-C without diet change in t'ai chi group. Medications and/or diet plans usually have faster short-term effects on outcomes of lipid profiles, 51 but the possibility of their long-term effect is not strong. 37 Although 1 h of t'ai chi may help in burning 300–400 calories that is comparable to energy consumption from moderate physical activity, 52 t'ai chi exercise produced better effects on lipid profiles compared to aerobic exercise. 37 The improvements might not be attributed to calorie consumption only but to metabolism enhancement, as well as anti-inflammatory activation. 37 However, the conflicting findings on HDL-C in past studies require further investigation.
Four included studies reported statistically significant results demonstrating improvement in LDL-C and TC levels, 36,37,46,48 and three included studies demonstrated improvement as noted through effect sizes in LDL-C and TC levels in the t'ai chi group in comparison to the control/comparison group. 34,36,47,48 Of note, most of the included studies demonstrated either statistical significance or positive effect sizes. Sun and Buys 35 did not report statistical significance, and Chen et al. 37 found a negative effect size for TC and did not report information needed to calculate an effect size for LDL-C. Hui et al. 47 found a negative effect size for LDL-C and TC, and Lu and Kuo found a negative effect size for LDL-C. 49 As noted for HDL-C, more research may be needed to discern the effects of t'ai chi on calorie consumption, metabolic enhancement, and anti-inflammatory activation due to the t'ai chi interventions. Future studies can be used to clarify the intervention components responsible for these large effect sizes. 36,48 Even though further specification is required, the results from the included studies present a generally positive conclusion that t'ai chi is effective in improving LDL-C and TC.
The results of the current review are partially consistent with previous meta-analyses which investigated the effect of t'ai chi exercise on lipid profiles in different populations. 38,41 Wang et al. reported significant improvement in levels of LDL-C in people with CVD after traditional Chinese exercise compared to the control. 38 Although the same change in LDL was observed, results of the current review are inconsistent regarding the improvement in HDL-C and TC compared to a recent meta-analysis. 38 The difference between results of the current review and the meta-analysis by Wang et al. 38 could be attributed to different study populations since the current review was not limited to people with CVD, but also including others such as inactive middle-aged people and older adults. Another difference was that their study covered all traditional Chinese exercises, including t'ai chi, qigong, or baduanjin. There were differences between the current meta-analysis and another recent meta-analysis, which reported only significant improvement in TC after t'ai chi compared to control in people with dyslipidemia. 41 The current meta-analysis, however, found significant improvements in levels of HDL-C and LDL-C as well. There were only two studies included in both of the two meta-analyses. 34,36 Different populations and interventions might have contributed to the inconsistency in the meta-analyses. The authors' study focused on the overall effect of t'ai chi in different populations. However, other meta-analyses focused on specific population such as people with CVD and/or different interventions such as qigong or t'ai chi exercise. The discrepancies among these different reviews and meta-analyses require further study.
Previous studies provided conflicting evidence regarding the effect of physical exercise on lipid profiles due to the standardization of diets 53 and the physical activity level before starting the exercise program. 54 In the reviewed studies, there was no information regarding the physical performance prior the intervention program.
The National Cholesterol Education Program has recommended placing therapeutic lifestyle changes, including diet, exercise, and necessary medications, to manage lipid profiles. 55,56 However, the reviewed studies did not control the intake of medications during the intervention, participation in diet programs, or engagement in extra exercise outside of the experimental study. Therefore, future studies are recommended to demonstrate the effects of a low-fat diet program and t'ai chi exercise in comparison to diet or exercise alone.
All reviewed studies reported improvements in other outcomes, including blood pressure, body–mass index, insomnia, glucose level, lipid profiles, or anxiety. These improvements support the use of t'ai chi exercise as beneficial intervention across different age groups and populations.
The current review has several limitations. The authors included articles only in English language in their search, which omits publications from East Asian countries in other languages. In addition, the authors did not include unpublished data or conference abstracts that may exist. Diet change is another confounding variable that was not assessed in this study. The difference in targeted population among different trials is another limitation that may lead to the mixed results on selected lipoprotein outcomes.
The meta-analysis had limitations. Most notably, the calculated effect sizes were only postintervention estimates. Only one study 34 allowed for the calculation of effect sizes using change scores. The rest of the effect sizes were calculated using post-test results. Thus, these effect sizes may not account for any significant differences existing between groups at baseline. Because all of the included studies were RCT, these differences may be minimal as a consequence of the randomization process.
In conclusion, the available evidence suggested that t'ai chi exercise might be a beneficial intervention across different age groups and diseases. However, conflicting findings about the effect of t'ai chi on HDL-C, as well as LDL-C and TC, have been reported in past studies. Although there have been positive and negative results reported in the past, the majority of studies had at least a small positive effect indicating a potential positive effect of t'ai chi on HDL-C, LDL-C, and TC.
Footnotes
Author Disclosure Statement
No competing financial interests exist.