
Abstract
Objectives:
Chronic pain is a common problem in the United States, one for which there is a dearth of effective treatments. Nonpharmacological options are a promising alternative, especially for Spanish-speaking Latinos. This pilot study would like to assess the feasibility of an adapted Integrative Medical Group Visit (IMGV) curriculum for a Spanish-speaking Latino chronic pain population.
Design and Intervention:
We translated and adapted the curriculum of the IMGV for a Spanish-speaking Latino chronic pain population. We then tested the feasibility of using this model with two pilot groups (N = 19) using a pre–postdesign.
Subjects:
This intervention was targeted for underserved Spanish-speaking Latino patients with chronic pain.
Settings/Location:
This study took place at a safety net academic teaching hospital, the Boston Medical Center, and at a community health center located in a majority Latino neighborhood, the East Boston Neighborhood Health Clinic.
Outcome measures:
We used the validated Spanish translations of the Patient-Reported Outcomes Measurement Information System (PROMIS-29) (short version), Personal Health Questionnaire (PHQ-8), and Perceived Stress Scale (PSS-10). We also gathered qualitative information through focus groups and in-depth interviews.
Results:
Using PROMIS measures, there was a statistically significant reduction in pain interference (p = 0.01), fatigue (p = 0.01), and depression (p = 0.01). Qualitative data also indicated the participants felt they benefited from the visits and having care in Spanish was unique.
Conclusions:
This model offers a promising nonpharmacological option for Spanish-speaking patients with chronic pain and could offer an alternative for addressing disparities for this population.
Introduction
C
There are healthcare disparities in the treatment of chronic pain, especially for primarily Spanish-speaking Latinos. Latino adults are less likely than non-Hispanic white patients to seek care with a primary care provider for pain. 8 Other factors related to disparities in care for pain include low socioeconomic status, language barriers with healthcare providers, low rates of health insurance, and fears related to immigration status. 7,9 –12
Latinos account for the largest growing minority in the United States, and are expected to reach 30% of the population by 2025. 13 Given this growing demand, it is especially important to have culturally sensitive treatments for chronic pain tailored to the needs of this population. 13 Some cultural values related to pain management in Latinos include stoicism, catastrophizing or religious coping when in pain, 14 and a preference for nonprescription-based treatment. 9,15 Acculturation, defined as the process of adapting to the behaviors, beliefs, and cultural elements of the dominant group in a society, can also affect how Latinos express factors related to pain and look for treatment options. 9 Research by Jimenez et al. suggested that when language preference was used to indicate acculturation, older Spanish-speaking Hispanics with pain had fewer functional limitations in contrast to their English-speaking counterparts. 16 Therefore, for example, providing an intervention entirely in Spanish is more likely to be culturally sensitive to this population and provide appropriate care for pain.
This paper describes a pilot clinical study testing the cultural adaption of a model for chronic pain care, the Integrative Medical Group Visit (IMGV). The IMGV combines CIM, medical group visits, and the principles of mindfulness-based stress reduction (MBSR). The group medical visit model of care can increase patients' self-efficacy in managing their pain and increases the time providers spend with patients. 17 Given Latino preferences for nonprescription-based treatments, this model is a promising way of providing access to efficient and effective culturally competent care and access to nonpharmacological services.
The conceptual framework for the IMGV is Engel's biopsychosocial model, which is often used to guide chronic pain interventions. 18,19 This model conceptualizes chronic pain as having interrelated causes and manifestations: physical, psychological, and social. The IMGV model addresses these multiple dimensions through a clinician-facilitated curriculum, which addresses health topics (insomnia, stress, and depression), teaching self-management tools to respond to pain (mindfulness and gentle movement) and increasing patient's social support. 20 Increased levels of social support have been identified as a protective factor in the development of chronic pain for the general population. 9 For Hispanics, who may be recent immigrants and socially isolated and separated from family still residing in their country of origin, social support can be a proxy for the traditional value of family support. It is possible that the social support offered in the Latino IMGV (LIMGV) model could serve as a clinical tool to reduce pain among Hispanics. 21
Previous work assessed the feasibility of an IMGV model to reduce pain and depression in an underserved group of patients, largely composed of racial and ethnic minority patients (Fig. 1). 22,23 The group visit curriculum was designed for low health literacy patients and in a pre–poststudy resulted in a statistically significant reduction in pain, depression, and perceived stress, as well as an improvement in sleep quality. 22
BMC Integrative Medical Group Visits. BMC, Boston Medical Center. MBSR, mindfulness-based stress reduction.
We hypothesized that culturally adapted IMGV model could be beneficial to underserved Spanish-speaking patients suffering from chronic pain, given the focus on nonpharmacological interventions and strong social support. Our aim is to assess the feasibility of the culturally adapted and translated IMGV model in underserved Spanish-speaking patients.
Materials and Methods
This is a pre–postpilot feasibility study conducted between January 2015 and May 2016. The Boston University Medical Center Institutional Review Board approved this study.
IMGV intervention
The nine IMGV sessions were held once a week. The clinician leading the sessions introduced the principles of MBSR, along with other CIM modalities (including acupressure, self-massage, and nutrition counseling) to the participants in a group setting (see Table 1 for a description of health topics and CIM modalities in the curriculum). During the first session, patients learned to measure and record their vitals (weight, blood pressure, and heart rate). They filled out an intake form at the beginning of every session, which included a rating of their pain intensity on a 0–10 scale and reporting their weekly home practice. Each session contained a “facilitated discussion” on a health topic (e.g., stress, insomnia, how pain manifests in the body, and anti-inflammatory foods). The participants also practiced different mind body techniques such a meditation, body scan, mindful yoga, self-massage, and acupressure.
Adapted and modified from Gardiner et al.. 22
Cultural adaptation
This intervention adapted the program developed by Dr. Gardiner at Boston Medical Center (BMC) for Latino Spanish speakers. The adaptation team included a majority Spanish-speaking team of two clinicians (MD), two medical students, a research manager with qualitative experience, two family medicine residents, and one non-Spanish-speaking research assistant. Dr. Gardiner also supervised the adaptation of the CIM practices, and MBSR exercises and concepts in the curriculum. The written curriculum was first translated from English to Spanish, then reviewed by the team for appropriate wording, meaning, and health literacy, and then rerevised accordingly until consensus was agreed upon. The adapted curriculum added unique pieces to make it more culturally relevant to the patients, for example, Hispanic poetry, recipes from different Hispanic countries, simplified wording for certain integrative medicine practices, and an emphasis on how change could be beneficial for the whole family, not just the individual with pain.
Research in overweight Latinos with chronic pain showed the importance of the use of complementary and alternative medicine strategies such as prayer, home remedies, herbs/teas, hot/cold, use of ointments/creams, use of vitamins/injections, relaxation, chiropractic techniques, and massage. 24 While creating the IMGV materials, we included common home remedies used among people from different Hispanic backgrounds. In addition to this, participants were given a meditation CD, which included the following mindfulness techniques: “awareness of breath,” “body scan,” and “loving-kindness meditation.” This CD was recorded in Spanish by the lead clinician, a native Spanish speaker, who was aware of the need to use Spanish words that were common to Hispanics from different origins.
The group visits were run by a Spanish-speaking provider and Spanish-speaking clinical assistants trained in mindfulness and CIM. There was an emphasis on allowing participants to discuss their thoughts on the practices. These discussions helped the provider rectify health misinformation, while giving participants control of the conversation. Participants were also encouraged to share their previous experiences with healthcare, what worked or had not worked for them, and what they were learning from the curriculum. Mid-term evaluations and focus groups where used to gather feedback to further adapt the curriculum.
Participants
Patients were enrolled at BMC, an academic teaching hospital, in the Family Medicine ambulatory clinic, and East Boston Neighborhood Health Center (EBNHC), a large community health center with a 70% Spanish-speaking patient population. The inclusion criteria included adults who speak Spanish as a first language and self-identify as “Hispanic” or “Latino(a)” with chronic musculoskeletal pain (with score of 4 or higher on a 1–10 scale for the past 12 weeks). The exclusion criteria included current pregnancy or plans to become pregnant in the next 3 months, given this intervention was not designed or tested for pregnant women. Other inclusion criteria were based on the safety of participants in the group or circumstances that could affect compliance with the intervention, including current psychosis or suicidal ideation, active substance abuse disorder, significant medical conditions that could affect participant's attendance (i.e., advanced cancer or surgery planned during the group visits), and previous IMGV participation.
Participants were recruited by being referred through their primary healthcare providers. After referral, research assistants called each participant and screened them for study criteria. If participants met study criteria, they were consented to the study using a Spanish consent form. Nineteen participants attended at least one session of the groups (11 to BMC and 8 to EBNHC). Participants on the study represent a diverse group of Hispanics, coming from seven different Spanish speaking countries (Table 2), and the majority were uninsured.
CIM, complementary and integrative medicine.
Data collection
Quantitative measures
To assess pain impact, depressive symptoms, anxiety, and perceived stress preintervention and postintervention, the following validated instruments were used: pain score during the last week (from the Brief Pain Inventory scale), PROMIS-29 (short version of pain interference, sleep disturbance, anxiety, and depression), PHQ-8, and PSS-10. All these have validated Spanish translations. 25,26
Qualitative measures
During the last week of the intervention, in each respective group, we conducted two focus groups to gather information on perceptions of the group visit, acceptability of the adaptation of the curriculum, how participants incorporated the techniques learned into their daily life, their overall experience with the intervention and group dynamics, as well as challenges to attending the sessions. We asked for recommendations from participants on making the curriculum culturally sensitive to Latinos from a wide variety of backgrounds. To avoid the possibility of bias, a native Spanish speaker, who had not attended any group visits and was not familiar with the participants, was the focus group moderator. All recordings of the focus group were transcribed by research assistants. These data are particularly important to our results for the purpose of determining the feasibility of this study in this population, given the otherwise small sample size.
Analysis
Quantitative analysis
Recruitment, retention, and survey data were analyzed using descriptive analysis: mean, median, and standard deviation for continuous variables, and frequencies for categorical variables. The primary analysis used “t”-test statistics with a level of significance (p value) <0.05. Differences in pain score using the PROMIS 29 questionnaire, as well as the PHQ-8 and PSS-10 were measured preintervention and postintervention. The analysis was performed using SAS software version 9.1. 27
Qualitative analysis
We used grounded thematic analysis, 28 where initial codes are developed and used to create higher order categories in a cumulative manner. Two members of the team coded the transcripts. The focus group was conducted in Spanish as were the transcription and coding of data. Any emerging themes were compared between coders and merged using an iterative process until agreement had been reached. Data from the focus groups were coded by two researchers independently, with a third member reviewing the coded data (triangulation) to ensure inter-rater reliability through a consensual discussion method.
Results
A total of 38 patients at BMC and 28 patients at EBNHC were referred by primary care physicians for participation in the LIMGV (Fig. 2). The first cohort took place at BMC. Once this cohort was completed, screening and recruitment of participants started at EBNHC. At BMC, 18 patients, and at EBNHC, 14 patients, were screened by phone. Eleven patients at BMC and eight patients at EBNHC were enrolled and attended first session. We gathered baseline data for all of these participants. Individuals who declined (n = 12) to participate cited scheduling difficulties as the most common reason. There was one patient who was ineligible due to a planned surgery. At BMC and EBNHC, 45.5% and 75% of patients, respectively, attended the ninth session and provided follow-up data.
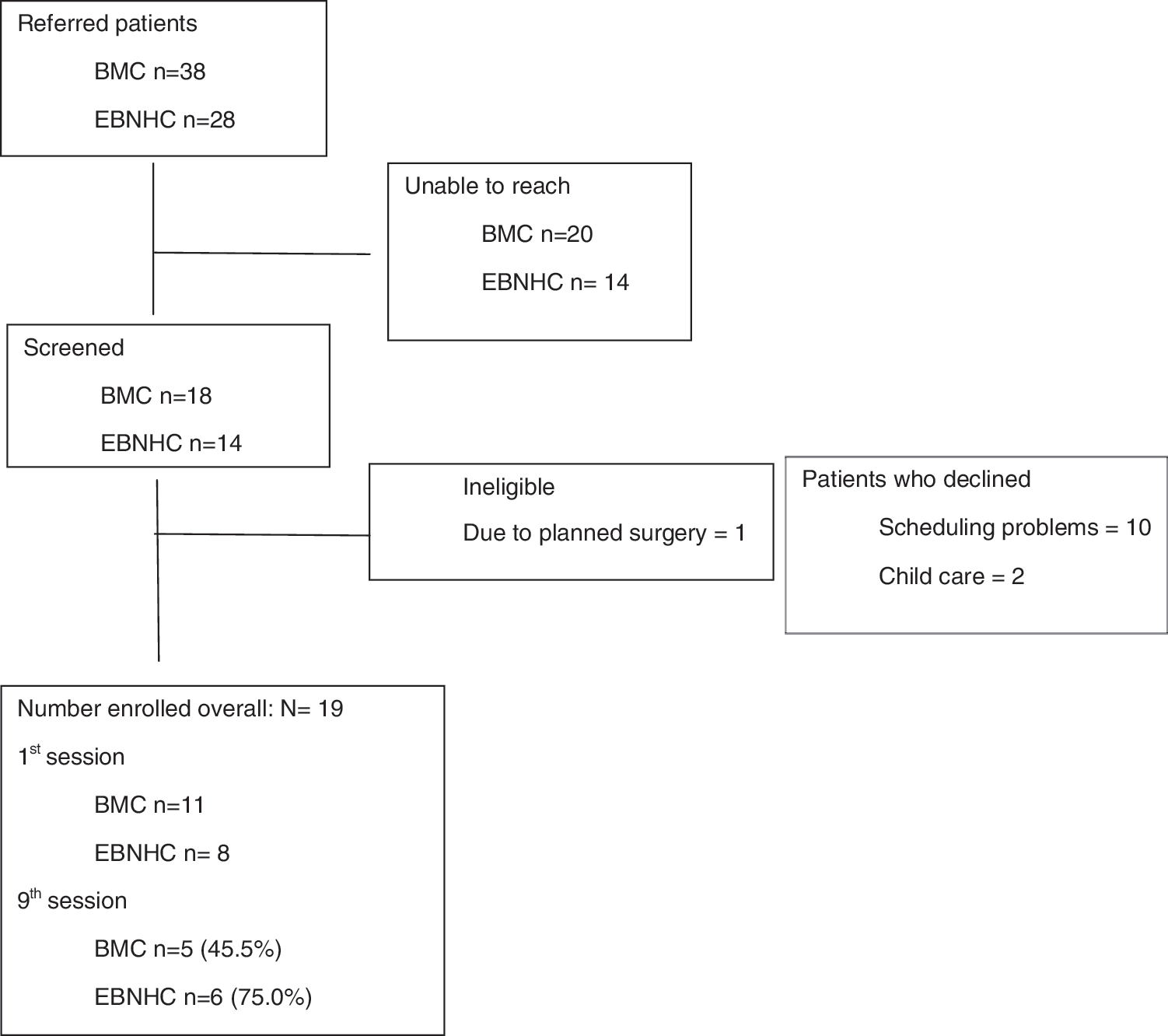
Recruitment flow for study. EBNHC, East Boston Neighborhood Health Center.
Demographics
The majority of the participants in the study were female (89%), and the mean age was 51.6 years (Fig. 2). Among the countries of origin, most of the participants were from the Dominican Republic, Colombia, and El Salvador. The educational level of the participants varied, with the majority having an elementary school education (35%) and the next largest group having some post-high school education (29%).
The “pain level during the past week” from the Brief Pain Inventory developed by Cleeland and Ryan (1994) was used to assess pain level scores at baseline. The mean pain score at the first week of the intervention was 6.9. The patients who had a previous experience with CIM therapy (n = 18), most commonly used acupuncture (44%), massage (28%), and chiropractic (22%) therapies (Table 2).
Quantitative results
Our results showed statistically significant reduction in pain (p = 0.01), fatigue (p = 0.01), and depression (p = 0.01) in PROMIS T-scores. The PHQ-8 pre–postdepression score was also fairly close to a statistically significant reduction (0.05). Our results also showed a statistically significant reduction in pain over the course of the study (p = 0.03) (Table 3).
Significant pre–postmeasures at α = 0.05.
PHQ-8, Personal Health Questionnaire; PROMIS-29, Patient-Reported Outcomes Measurement Information System; PSS-10, Perceived Stress Scale.
Qualitative results
During the focus group sessions (10 participants) and the in-depth interview (one participant), the information provided centered on the following themes: positive feedback about their experience; improved nutrition habits; group sessions are preferred over individual appointments; decreased pain; group solving effect; and a preference for medical care in Spanish.
Positive feedback about their experience
Participants expressed their gratitude and felt motivated to make health behavior changes by participating in the LIMGV.
Before the group, I did not used to go out, now I talk to others, … now, I go out, and when I wake up I pray to God, and thank God…and go out, and I feel different, because I feel this has helped me, it has helped me spiritually and in my health…it has helped me a lot”
Group “problem” solving
Patients noted the importance of sharing problems as a group. The “group solving effect” is well described in the literature, and was one of the main themes emerging from participants of the LIMGV. 17
[When] you are in the group and hear what others are going through is much worse than your own problems, and you ask yourself, how can I be complaining if this other person is still alive …and smiling? I am dying just being anxious, when this other person has much worse problems than me
Preference of group visit to individual visit
Preference of the group visit versus the traditional doctor–patient encounter focused on two main aspects: perception of having more time with your doctor and the collaborative relationship among participants to learn new skills or knowledge about different health topics.
Well, it is very different, the visits with your doctor are about fifteen minutes, you do not have much time to explain where you hurt, however, in the group it's very different because you have two hours and you have time to explain to the doctor or you could explain to him individually what your problem is, in detail, and look for a solution other than pills, alternative medicine instead…it is very important
Decreased pain experience/improved pain coping
Some participants mentioned that they were taking less pain medications after attending the group, and even though they recognized the pain was still there, they argued their pain was better controlled.
I take my time and relax, I am taking less medicines and the chronic pain I used to have for long time has improved a lot. The pain has not gone away, I still have it, and with today's weather, cold…there are some days you wake up with back pain, pain in the joints, but what used to have improved a lot with the medicines the doctor prescribed. I used to have a lot of pain in my hips and knees, and that has improved…thank God
Better nutrition
Another common theme was food related, including the difference nutrition can have on their bodies, and how it affects pain.
… it was around the importance of food,…, one may think ‘let's eat’ but now one thinks let's eat not automatically, instead one has to eat nutritious food that doesn't worsen the pain we have. So, this is what you learn, to eat mindfully, to learn to chew. I myself did not use to chew the food, just swallowed it, fast, so many things I have learned in such a short time, and that now will stick in my mind for all my life, because that will not be forgotten
Having the group visit and materials be in Spanish
When asked about their thoughts on the intervention being delivered completely in Spanish, everyone expressed their gratitude for being able to communicate and interact with physicians and peers in their native language.
When he, the doctor, told me that it was in Spanish, I asked him: is that in Spanish? … and he said ‘yes, everything will be in Spanish’, I felt so happy, because sometimes, because of the language you feel isolated and say no, I won't be able to participate, how I am going to express myself?, but thank God, expressing yourself in your own language is very nice
Suggestions for improvement
Participants also mentioned that adding a “dancing” piece into the program could be beneficial for decreasing stress.
Well, I think that if the next group would agree, they should have a dance session. I would have liked us to have dancing as part of the program, because I think that helps you a lot with the stress.
Discussion
The results from this study indicate that it is feasible to adapt and implement an IMGV model for low-income Spanish-speaking patients with chronic pain in an outpatient medical setting. Our pre–postresults showed statistically significant reduction in pain, fatigue, and depression based on the PROMIS scales. These findings are consistent with reports from previous literature. 22,29,30
The “decreased pain” theme was also noted in the qualitative data analysis. Participants recognized that they still had pain, but they were able to cope better with their chronic pain, had more control of it, and also mentioned reduced use of pain medications. Further study is needed to determine if these results would be clinically meaningful. The fact that participants were naive to the concept of group medical visits and found the different components of this intervention helpful indicates its feasibility among this Spanish-speaking population. In considering the cultural acceptability of the IMGV intervention, our qualitative data included patients' gratitude on having the intervention in Spanish. Patients mentioned the fact that expressing themselves in their native language helped them connect to others and not feel “isolated.” This is particularly important when trying to improve access to healthcare for those in an unfamiliar culture, who struggle with a lack of social support and language barriers. This study suggests that the LIMGV intervention for Spanish-speaking patients with chronic pain was considered both acceptable and appropriate by the participants.
One recommendation from the participants was to consider a more active “movement/dance” component into the curriculum. The current LIMGV program has one session where participants learn and practice mindful movement. Taking into account the importance of dancing within the Latino culture, a session of “Zumba” may be considered for future programs. This curriculum can also be tested with a more heterogeneous Latino population to ensure broad cultural acceptability.
This study has limitations, such as having only the “intervention group” without a control cohort. The results presented in this paper are from a small sample of low-income Spanish speakers living in inner city Boston, and may not be generalizable to other Latino population in the United States. Recruitment and retention rates in this study are comparable to group visit studies in English speakers. 22 This study was not funded; so limited time devoted by “volunteer” research assistants could have contributed to low retention rates.
In our qualitative data, there were negative feedbacks from participants, related to the fact that some people only attended the first session or two. Participants also wanted better organization of the curriculum. The mostly positive feedback from our focus groups could suggest that patients who attended were positively biased toward our intervention and our findings may not be generalizable to other Latino populations. Finally, the curriculum adaptation was made by a team representing three Spanish-speaking countries. Participants came from seven different Latin American countries, meaning the curriculum may not account for all Latin American cultural differences. We tried to offset this limitation by having open discussions within the study team and in the group visits for clarification of the material, as well as having a mechanism for feedback from the participants about the curriculum.
Conclusion
The LIMGV is an innovative intervention that could address the emotional, psychological, and physical burden of chronic pain among vulnerable Latinos. Given the preliminary results of this study, future studies should assess this model of care using a larger sample and implementing this model of care in primary care settings, serving a large Hispanic population. Successful implementation studies could potentially aid in reducing disparities in the access of chronic pain among vulnerable populations.
Footnotes
Author Disclosure Statement
No competing financial interests exist.