
Abstract
Objective:
Despite the political commitment of national governments and collaborative efforts by the World Health Organization (WHO) toward the actualization of intercultural healthcare system over the past decades, sub-Saharan African countries feature medical cohabitation rather than a truly integrated medical system. This hospital-based cross-sectional study analyzed the capabilities of nurses for complementary and traditional medicine (CTM) integration in Africa.
Method:
Practicing nurses (n = 210) were recruited to respond to the CTM Health Belief Questionnaire (CHBQ) in December 2016. Normality of data was evaluated using Kolmogorov–Smirnov statistic with a Lilliefors significance correction. The authors assessed the relationship among nurses' knowledge, personal use, and clinical practice of CTM, using Spearman's Rank Order Correlation (rho). The differences and associations in continuous and categorical baseline variables were determined with Mann–Whitney U test/Kruskal–Wallis H test and Pearson's Chi-square test, respectively, at p < 0.05 as statistically significant.
Results:
The overall mean score of nurses' knowledge of CTM therapies was 38 (interquartile range [IQR] 16). This low CTM-related knowledge reflected in the poor mean performance score of 30 (IQR 17) and 22 (IQR 6) for personal use and clinical practice of CTM, respectively, among nurses. Nurses, therefore, lacked the confidence to recommend CTM therapies to patients. Yet, nurses exhibited a high positive attitude to CTM (72.7 ± 12.5). In addition to significant associations among CTM-related knowledge, education (p = 0.023), and religion (p < 0.001), the study found a positive and statistically significant correlation among CTM-related knowledge, personal use (r = 0.556, p < 0.001), and professional practice of CTM (r = 0.349, p < 0.001).
Conclusion:
Given their substantial role in the primary and public healthcare system, improving nurses' knowledge of CTM through evidence-based nursing education and training remains the surest way to achieve appropriate CTM integration in Africa as outlined in the WHO Traditional Medicine Strategy 2014–2023.
Introduction
A
In recent past, the global interest and uptake of CTM have significantly increased in advanced countries where sophisticated biomedical sciences have classically dominated the healthcare arena. 1 –4 The World Health Organization (WHO) reported that there are over 100 million users of CTM in European countries. 1 According to National Center for Complementary and Integrative Health (NCCIH), in the United States, ∼38% of adults (about 4 in 10) and ∼12% of children (about 1 in 9) are using some form of CTM. 5 Other high-income countries have shown high prevalence of CTM use, including Australia, 6 Korea, 7 Canada, 8 Singapore, 9 and Japan. 10 The development of CTM has become a constitutional mandate in Hong Kong. In developing world, an estimated 60% to 90% turn to CTM for their primary healthcare needs 1 with different practices and products due to cultural, historical significance, socioeconomic, and regulatory peculiarities. 11,12 In African Region, various independent national surveys found that ∼90% Ethiopians and Burundians, 85% South Africans, 75% Malians, 70% Rwandans, Beninese, and Ghanaians rely on CTM 13,14 in the wake of escalating healthcare costs and increased levels of chronic and other dreadful illnesses, including malaria, cancers, hypertension, diabetes, dementia, and HIV/AIDS.
Notwithstanding the growing acceptance of CTM, there have been incessant calls for evidence-informed CTM with vested efficacy and safety, 15,16 especially in Africa, where a renewed form of CTM is needed most. In this regard, the WHO Traditional Medicine Strategy 2014–2023 was developed to support all Member States in harnessing the potential contribution of CTM to health, wellness, and people-centered healthcare and to promote the safe and effective use of CTM through the regulation of products, practices, and practitioners. 1 According to the WHO, this strategic plan aimed specifically at creating knowledge for framing national policies, affirming safety, quality, and effectiveness through regulation and promoting universal health coverage by integrating CTM services and self-healthcare into national health systems. 1
Studies show that the integrative process remains the surest way to attain a standard medical practice toward health promotion and disease prevention. 17,18 Although the past decades have witnessed certain levels of collaboration between CTM and mainstream national healthcare system, African countries feature medical cohabitation rather than a truly integrated medical approach. 18 Any policy in regard to medical integration critically needs to take account of individual level involvement and cultural acceptability of care provided by healthcare professionals, 18 with particular reference to nurses who are constantly in direct contacts with healthcare consumers. While the distribution of allopathic health force and resources are urban-biased, 19 –21 health systems in Ghana are poorly integrated to offer the benefits to the citizenry. 18
A vital driving force of the renewed focus on the safety and effectiveness of CTM in evidence-based practice is to eschew the marked skepticism of nurses and other healthcare professionals. 22 The practicality of evidence-informed CTM integration in the African context rests, in part, on the attitude, knowledge base, and professional practice among nurses. 23 While reports from previous studies show positive attitude toward CTM generally, 24 –28 nurses, to a larger extent have demonstrated overwhelmingly poor knowledge on the various modalities, benefits, and the potential side effects of CTM, 4,29 –31 and often defame the CTM practices and practitioners. 32,33 As long as nurses are the major port of call by patients at the healthcare facility-level relative to other healthcare providers, 34 nurses are expected to provide trusted and a more credible health information and medical assistance to clients. Nurses, in the first place, should be adequately and assertively informed, and have in-depth knowledge on CTM. This is subject to a professional training and specific educational paradigm on CTM for nurses 35 to make them more confident to advise their patients who use CTM.
After decades of failed attempts to procure a spot-on integration of CTM into the national healthcare systems in the respective African countries, there has been paucity of empirical studies on the capabilities of nurses for a successful CTM integration in Africa. The present study aimed at examining practicing nurses' knowledge of CTM, personal use, clinical practices, and attitude toward CTM as a conduit to integrative medicine discourse in Africa, taking evidence from Ghana.
Materials and Methods
Design and procedure
A hospital-based cross-sectional urban survey was conducted in the Metropolitan Kumasi from December 1 to December 30, 2016. Being one of the main cosmopolitan and populous districts in Ghana with diverse cultural and socioeconomic backgrounds, Kumasi was deemed appropriate for this study. With a two-stage sampling strategy, the study site was divided into two enumeration areas based on north–south delineation, selecting four hospitals in each area for the study. The study hospitals included a teaching hospital, a university-affiliated hospital, and six other community-based hospitals in the metropolis. Three of them had private health facilities. The facilities ranged from origin health or derivation centers to referral points, which provide healthcare needs for a wide range of health challenges and health promotional interventions to the citizenry. A convenience sample of 256 registered and practicing nurses (eligible for the study) were invited for a face-to-face interview. While 229 nurses agreed to partake in the study, 19 of them provided incomplete information, and therefore, excluded from the final sample. The total sample included in the analysis was 210, with a response rate of 82% (Table 1). Nurses responded to questionnaire on their knowledge of CTM, professional practice regarding the discussion and recommendation of CTM modalities to patients, their personal use of CTM strategies, and their attitude toward CTM.
Study protocol
The approval for this study was obtained from the Committee on Human Research Publication and Ethics (CHRPE), School of Medical Sciences at Kwame Nkrumah University of Science and Technology and Komfo Anokye Teaching Hospital, Kumasi, Ghana (Ref: CHRPE/AP/507/16). The authors again secured written informed consent from the heads of each hospital before contacts with the individual nurses in accordance with the Declaration of Helsinki. 36 Furthermore, oral informed consent was received from each participant ahead of the interview. Participants were assured of the strict confidentiality of the information they provided.
CTM-related knowledge and use of CTM
Knowledge, uptake, and recommendation of CTM to patients were evaluated via an adaptation of the CTM Needs Assessment tool, 37 which is a list of 18 CTM treatment modalities chosen from the most commonly used modalities included on a list of 40 therapies purposed to be integrated into the national healthcare system. The preliminary list of therapies was developed by a consensus of international researchers in the field of CTM, informed by a literature review, and then forwarded to a panel of medical and nursing experts at Kwame Nkrumah University of Science and Technology, Kumasi for approval. Respondents were asked about their knowledge of the various CTM methods and whether they had ever used or were currently using any of the treatments listed, and whether they would recommend or consider recommending these treatments to patients.
Nurses were asked to indicate the level of their current CTM-related knowledge in any of 18 CTM strategies and to rate the intensity of their responses on a Likert-type scale of four options from “None” = 1 to “A lot” = 4. Scores on the knowledge assessment scale ranged from 18 to 72, where 18 to 36 was adjudged as poor, 37–54 = average, and 55–72 = good. Participants were asked to indicate, in the second section, the frequency of personal use of the CTM methods in the last 12 months preceding the survey. The responses utilized a 4-point Likert-type scale ranging from “never” = 1 to “3+ times” = 4 for a total possible score ranging from 18 to 72. Scores between 18 and 36 were considered poor, 37–54 = average, and 55–72 = good.
In the third section, the participants were asked to give a “no” = 1 or “yes” = 2 response to an 18-item question regarding the recommendation of various CTM methods during practice, for a total possible score ranging from 18 to 36. Scores ranging between 18 and 24 were adjudged as poor, 25–30 = average, and 31–36 = good. Scoring for varied sections of the questionnaire was determined by the researchers based on their cumulative experience with CTM methods analytics. The use of dichotomous response set—“yes” or “no”—regarding the professional use of CTM methods made responses quick and easy for respondents, while the use of a Likert-like scale yielded interval level data to enriched findings, especially for a variable latently assessing the willingness to recommend a CTM therapy.
Attitudes toward the use of CTM
The questionnaire examined nurses' attitude toward CTM via an adaptation of the CTM Health Belief Questionnaire (CHBQ). 37 The CHBQ asked nurses to score their agreement with 22 statements, for example, “CTM promotes a holistic approach to health,” “CTM can be integrated into current nursing practice,” “Health professionals/nurses should be knowledgeable about CTM and be able to advise their patients on commonly used CTM,” and so on. Scores ranged from “strongly disagree” = 1 to “strongly agree” = 5. Scores 1–2 reflected disagreement and 4–5 signified agreement with each statement. An overall score, ranging from 67 to 110 reflected a more positive attitude toward CTM, whereas a lower score ranging from 22 to 66 represented a negative attitude.
Validity and reliability of the questionnaire
The face and content validity of the questionnaire were established by both a comprehensive review of the literature and consultation with experts in the field of health service provision. The panel of experts assessed the questionnaire's validity, language clarity, the ease of use, its relevance, and the appropriateness of therapies listed for the purposes of the study. Internal reliability and consistency of the items were established with Cronbach's alphas (α), and the validity of the construct was reported. Using the Cronbach's α ≥0.7 criterion, the researchers found internal consistency and the reliability coefficients of knowledge, personal use, and professional practice constructs to be satisfactory (Table 2).
p < 0.05, *** p < 0.001.
Lilliefors Significance Correction.
Statistical analysis
Data were entered into and analyzed using SPSS v.21.0 (IBM, Armonk, NY). Data were summarized using frequencies and proportionate counts for the categorical sociodemographic variables and as means ± standard deviations for normally distributed continuous variables, or median with interquartile ranges (IQRs) for skewed continuous variables (overall knowledge, personal use, and professional practice of CTM therapy scores). The normality of continuous variables was tested using the Kolmogorov–Smirnov statistic, with a Lilliefors significance correction, which indicated violations of assumptions of normality (Table 4). Nonparametric Mann–Whitney U test and Kruskal–Wallis H test were applied to analyze differences in the continuous variables. Furthermore, bivariate correlation analyses were performed to investigate the strength of the relationship between nurses' knowledge and personal/professional use of CTM using Spearman's Rank Order Correlation (rho). Statistical significance was considered at a threshold of p < 0.05.
Results
Sociodemographic and clinical characteristics
Table 3 shows the demographic and clinical characteristics of the sample. The majority (81%) of respondents were females, about a third (30%) had completed an undergraduate degree or higher (the remaining 70% had a Diploma and Nursing Certificate), and ∼80% of participants were below the age of 40 years. The majority of participants had had speciality training in Maternity and Women's Health (26%) or Adult medical nursing (21%) and most (71%) reported having nursing clinical experience of up to 5 years. The median salary for the respondents was GH¢973 (IQR 675.55).
p < 0.05, *** p < 0.001.
Knowledge scores of nurses about CTM.
Mann–Whitney U test.
Kruskal–Wallis H test.
CTM, complementary and traditional medicine; IQR, interquartile range.
Personal use and professional practice of CTM therapies
The normality scores for personal use and professional practice of CTM therapies (p < 0.001), assessed with the Kolmogorov–Smirnov test revealed significant results which indicated skewness of the scales. A mean performance score of 30 (IQR 17), reflecting an overall poor use of CTM methods for personal purposes by the nurses, was recorded as the performance score falls within the poor score zone of 18–36. Respondents had a mean performance score of 22 (IQR 6) (which is within the zone of 18–24), also reflecting an overall poor use of CTM therapies in clinical practice as in (Table 2).
Knowledge of CTM
The overall mean score of nurses' knowledge about CTM therapies was 38 (IQR 16). This indicates less than the average score for the sample. Kolmogorov–Smirnov normality test conducted a priori, showed non-normal distributions for CTM knowledge (p < 0.05). Analyzing the association among knowledge about CTM, sociodemographic, and clinical experience variables using Mann–Whitney U test and Kruskal–Wallis H test found no significant associations between CTM-related knowledge and sex, age, salary, marital status, clinical experience, ethnicity, and the clinical speciality of nurse (p > 0.05) (Table 3). Howbeit, significant associations were found among education (p = 0.023), religious affiliation (p < 0.001), and CTM knowledge—an indication of nurses with at least an undergraduate degree having more knowledge about CTM therapies than their diploma-/certificate-certified counterparts. Also, Christian nurses were less informed about the CTM therapies than nurses with other religious affiliation.
Relationship among nurses' knowledge, personal use, and professional practices of CTM
Using Spearman's rho correlation coefficient (Figs. 1 and 2), the authors found a moderate positive and statistically significant correlation between CTM knowledge and personal use of CTM (r = 0.556, p < 0.001). Despite a weak relationship, CTM-related knowledge was found to be positively associated with the professional use of CTM (r = 0.349, p < 0.01). Further analysis revealed statistically significant increases in scores of domains of CTM use (personal and professional) with increasing scores of knowledge of corresponding CTM domains. All eight CTM domain variables' associations had correlation coefficients between 0.20 and 0.50. Spearman correlation matrices are depicted in Table 4.
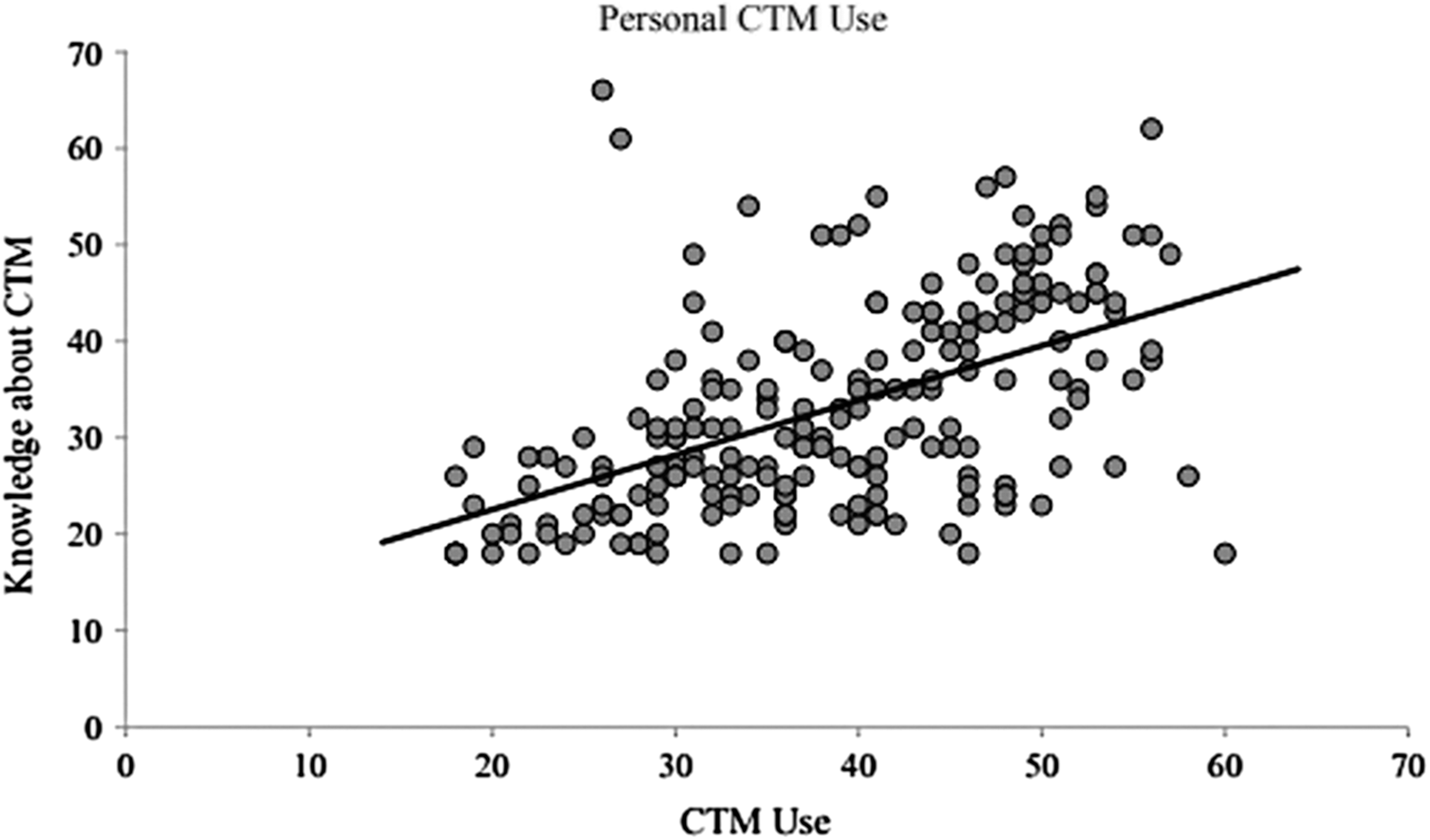
Correlation between nurses' knowledge and personal use of CTM. CTM, complementary and traditional medicine.
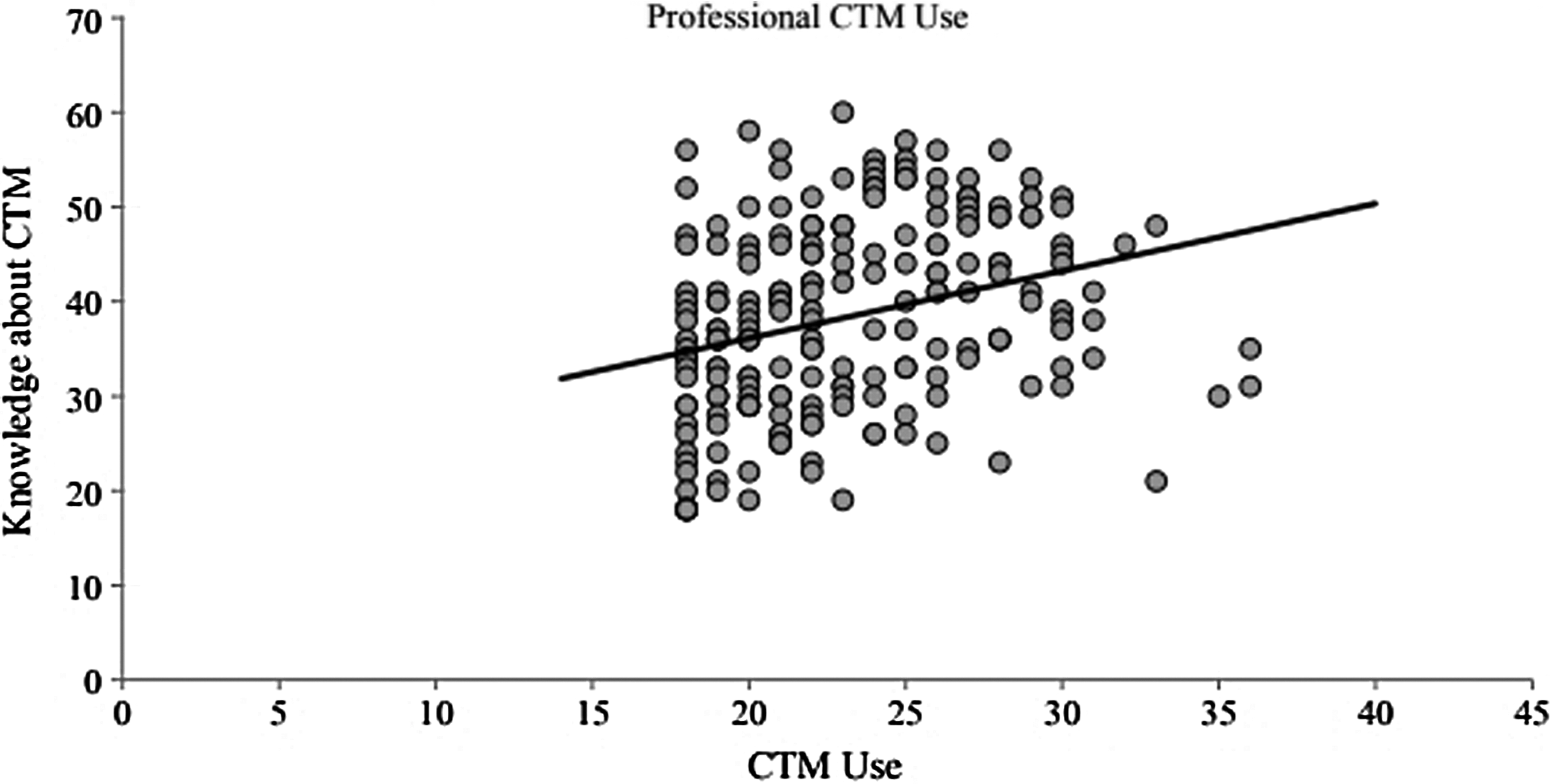
Correlation between nurses' knowledge and professional use of CTM.
**p < 0.01, ***p < 0.001.
Attitude toward CTM
The study revealed a mean total CHBQ score of nurses' attitude toward CTM use to be 72.7 ± 12.5 (range, 41–97; possible range, 22–110). Furthermore, an overall majority of nurses had a positive attitude toward CTM use (n = 144, 69%) (Table 5). Correspondingly, a large number of nurses expressed agreement with most of the attitudinal statements offered.
Discussion
Despite the wrestle and skepticism over the integration of CTM within policy making, health profession, and the public arena, various modalities of CTM continue to provide primary and public healthcare needs in Africa, with its use, rapidly increasing globally. The WHO Traditional Medicine Strategic Plan 2002–2005 and the revised version 2014–2023 emerged to address issues of policy and safety and also quality dimensions of CTM. 1 The integration of CTM into the national healthcare system, which remains the cornerstone for the rational use of CTM and ensures the safety of the public, 18,38 has not seen full actualization in the African countries. The knowledge, personal and clinical use, as well as the attitude of the healthcare professionals and nurses, particularly toward the CTM, are critical in the medical integration journey. The current study provides a comprehensive analysis of the capabilities of nurses for CTM integration in the African context.
The burgeoning use of CTM in African countries should, in part, manifest in the evidence-based clinical recommendation for CTM therapies. Best practices of integrative healthcare in the hospital setting largely hinges on the support of nurses, reinforced by their excellent knowledge about CTM. Nevertheless, this study shows that Ghanaian nurses, in general, do not perceive themselves to have sufficient knowledge about CTM. This has a strong connotation with an overall poor use of CTM methods by the nurses for personal purposes and clinical practices. The general CTM-related poor knowledge of nurses demonstrates a weak inclusion of theoretical and practical modules of CTM therapies in nursing education and training programs in Africa. These findings are not different from the observations of other studies globally, 30,39 –41 despite the view that nursing practice is ingrained in the integrative medical paradigm of care, healing, and holism.
Intriguingly, the present study found positive significant association among CTM knowledge, personal, and professional use of CTM. This relationship further increased in scores of domains of CTM use with increasing scores of knowledge of the corresponding CTM domains. In addition, nurses with higher nursing educational training, correspondingly, exhibited higher CTM-related knowledge. These lend credence to suggest that nursing training on CTM remains critical to improving nurses' knowledge about CTM. Studies have shown that incorrect delivery and dispensing of therapies and the attendant medical error due to insufficient knowledge and/or lack of competence may present a devastating consequence to patients. 24,42 –45 Hence, the need for culturally acceptable approaches to improve the knowledge and confidence of nurses in practicing CTM. Nursing education programs and curricula in Africa, therefore, need a rigorous review to embrace detailed CTM content and/or modules. This may serve as a critical link in a chain of interventions needed for ensuring safe and effective use of common CTM strategies within the ambit of integrative medicine outlined by the WHO Traditional Medicine Strategy 2014–2023. 1 Adaptation of this framing by the Ministries of Health and the associated Health Services of the respective African countries may provide fertile grounds to empowering nurses in clinical practice of CTM toward the well-being of the unsuspecting patients.
In spite of the different agreement levels reported, nurses overwhelmingly portrayed a positive attitude toward CTM use and its integration into the allopathic healthcare system. While this finding is consistent with previous studies, 46,47 the high CHBQ score (mean = 72.7 ± 12.5) in this study is higher than those found in some advanced-country studies. 48,49 Nurses thought of CTM as a preventative measure that could offer a holistic primary care in the healthcare system. The majority of nurses strongly welcome any needful incorporation of CTM into accepted allopathic medical practice. This move is key to standardization processes of CTM, including the development of clinical practice guidelines. 42
This is the first known study, of which the authors are aware, to tease out the potentials of registered nurses to CTM integration in Africa with Ghanaian example, taking into consideration nurses' knowledge, practices, and attitude toward CTM. Although the current study is a useful contribution to the intercultural healthcare discourse in Africa, the results are tainted with some limitations. The retrospective cross-sectional survey does not only disallow causal relationship and/or inferences to be made, it is also potentially prone to recall biases which could compromise accuracy. Again, the CTM strategies considered in this study excluded some culturally specific traditional practices, including consultation with traditional healers. Although the study was conducted in urban Ghana, the findings mirror evidence from sub-Saharan Africa and other countries with a similar sociocultural setting.
Conclusion
This study presents findings of a representative study of the association between nurses' knowledge and use of CTM vis-à-vis their attitude toward CTM remedies. Nurses' positive attitude toward the use of CTM provides some evidence to suggest that nurses could be agents for integration of clinically approved CTM modalities into nursing primary care. Despite the view that CTM-related knowledge of nurses correlates positively with their personal use and professional practice of CTM in the in-hospital context, nurses generally showed poor and insufficient knowledge about CTM therapies, which resulted in their overall poor use of CTM personally and clinically. Being the keystone of healthcare and primary care system, there is an exigency to improve nurses' knowledge of CTM through nursing education and training in the curriculum alignments toward the fulfillments of the WHO Traditional Medicine Strategic Plan for appropriate CTM integration in Africa. In this way, a high healing impact for newly emerging illnesses, particularly the chronic noncommunicable conditions, could be procured, and proffer a renewed strength for disease prevention, health promotion, and health preservation in Africa.
Footnotes
Acknowledgments
The authors wish to thank the nurses who generously participated in this study in the various hospitals. They further acknowledge the stellar support offered by Mr. Godfred Amankwaa, their research assistant during the data collection stage. The Editor-In-Chief, Prof. John Weeks and the two anonymous reviewers of this journal deserve no mean an appreciation for offering gracious and irreplaceable comments and invaluable insights, which helped to improve upon the earlier versions of this article.
Author Disclosure Statement
No competing financial interests exist.