
Abstract
Objective:
Inadequate treatment of pain in patients undergoing surgery is associated with unsatisfactory perioperative outcomes. The aim of this study was to examine the role of reflexology in addition to standard analgesic treatment in postoperative pain management.
Design:
This was a prospective, unblinded pragmatic controlled trial.
Setting/Location:
Study participants included patients who were admitted to the general surgery department.
Interventions:
Patients in the intervention group received reflexology while standard analgesic care was administered similarly in both groups.
Outcome measures:
Pain intensity at rest and in motion was evaluated using visual analog scale (VAS [0–10]) at baseline, and 60–90 min after treatment.
Results:
Pain reduction was clinically and statistically significant in the reflexology group, both for pain at rest (from mean VAS of 4.4 to 3.1, N = 77, p < 0.0001) and for pain in motion (from 6.2 to 4.2, N = 77, p < 0.0001). In the control group, pain at rest was not reduced at follow-up (from 4.7 to 4.6, N = 87, p = 0.92), nor was pain in motion (from 5.8 to 5.7, N = 87, p = 0.65). Comparison of mean difference for pain showed significant improvement in the reflexology group compared to the standard of care group (p < 0.0001). The most significant pain reduction in the reflexology group was observed among patients who had moderate-severe baseline pain (VAS >4).
Conclusion:
Adding reflexology to standard analgesic care is effective in reducing postoperative pain at rest and in motion, especially for patients experiencing moderate to severe pain.
Introduction
P
Reflexology is a noninvasive and safe treatment method based on the principle that the feet represent a map of the entire body and that distant parts of the body can be treated by manipulation of the feet. 3 A number of studies examined the impact of reflexology on pain measures. A study comparing the effectiveness of reflexology to that of ibuprofen in treating menstrual pain found a significant preference for reflexology with respect to both pain duration and pain intensity (as measured by visual analog scale [VAS]). 4 Babajani et al. reported the effect of reflexology on pain upon chest drain removal following open heart surgery and demonstrated a reduction in pain following reflexology treatment. 5 However, a number of published clinical studies did not demonstrate reflexology to be any more effective than nonspecific massaging of the feet. 6 –8 Some evidence in the literature indicates that reflexology is beneficial in diminishing pain, but the literature is scanty both in terms of the number of articles and quality of research methodology. 6 Because reflexology is a practical and safe form of intervention that does not require many resources, it may serve as a potential treatment to manage postoperative pain control. In this study we examine the use of reflexology as a method for alleviating acute postoperative pain.
Methods
Before enrolling patients in this study, we attained approval from the Institutional Review Board (IRB No. 0041-09-BNZ) of the Bnai Zion Medical Center, Haifa, Israel. The study was registered before its inception at
Research type
This was a prospective pragmatic controlled and randomized trial.
Research setting and population
The study was conducted at Bnai Zion Medical Center in Israel, which is a tertiary academic medical center. Since 2010, a complementary medicine service is integrated in the surgery wards of the hospital. Patients are treated free of charge by various Complementary and Alternative Medicine modalities such as hypnosis, reflexology, acupuncture, and guided imagery with the aim of reducing common symptoms such as pain, nausea, and anxiety. 9 The study population comprised patients who were admitted between November 2011 and January 2015 to the surgical department of the Bnai Zion Medical Center in Haifa to undergo various surgical procedures. Most of the patients were admitted on an elective basis for nonurgent intervention. The intervention group received reflexology in addition to the standard analgesic treatment. The control group comprised patients who were treated with standard analgesics only. Patients were assigned to the groups according to the reflexologists' work days. On the days the reflexologist worked at the department patients received reflexology in addition to the standard treatment. On the days the reflexologists did not work, patients received the standard treatment only. Inclusion criteria were as follows: patients who consented to participate in the research, had been operated on during the past 48 h and reported pain in motion exceeding 2 on the VAS scale during the nurses' rounds. Exclusion criteria were as follows: unwillingness to sign the research participation form, limitations in comprehending informed consent in Hebrew, patients with foot ulcers, patients with borderline or unstable hemodynamic measures, such as tachycardia, bradycardia, and systolic blood pressure over 180 or under 100.
Research procedure
Patients with VAS scores of pain in motion equal or above 2 received analgesics and were offered to participate in the study according to eligibility criteria. Patients assigned to standard care (on days of absence of reflexologist) were re-evaluated by research assistants for VAS within 30 min of the referring nurse's evaluation. On days that the reflexologist was present, VAS was re-evaluated similar to the control group followed by reflexology treatment. A follow-up VAS evaluation was conducted in both groups about 90 min after the previous VAS assessment (Fig. 1). Each patient received a single reflexology treatment the day after surgery.
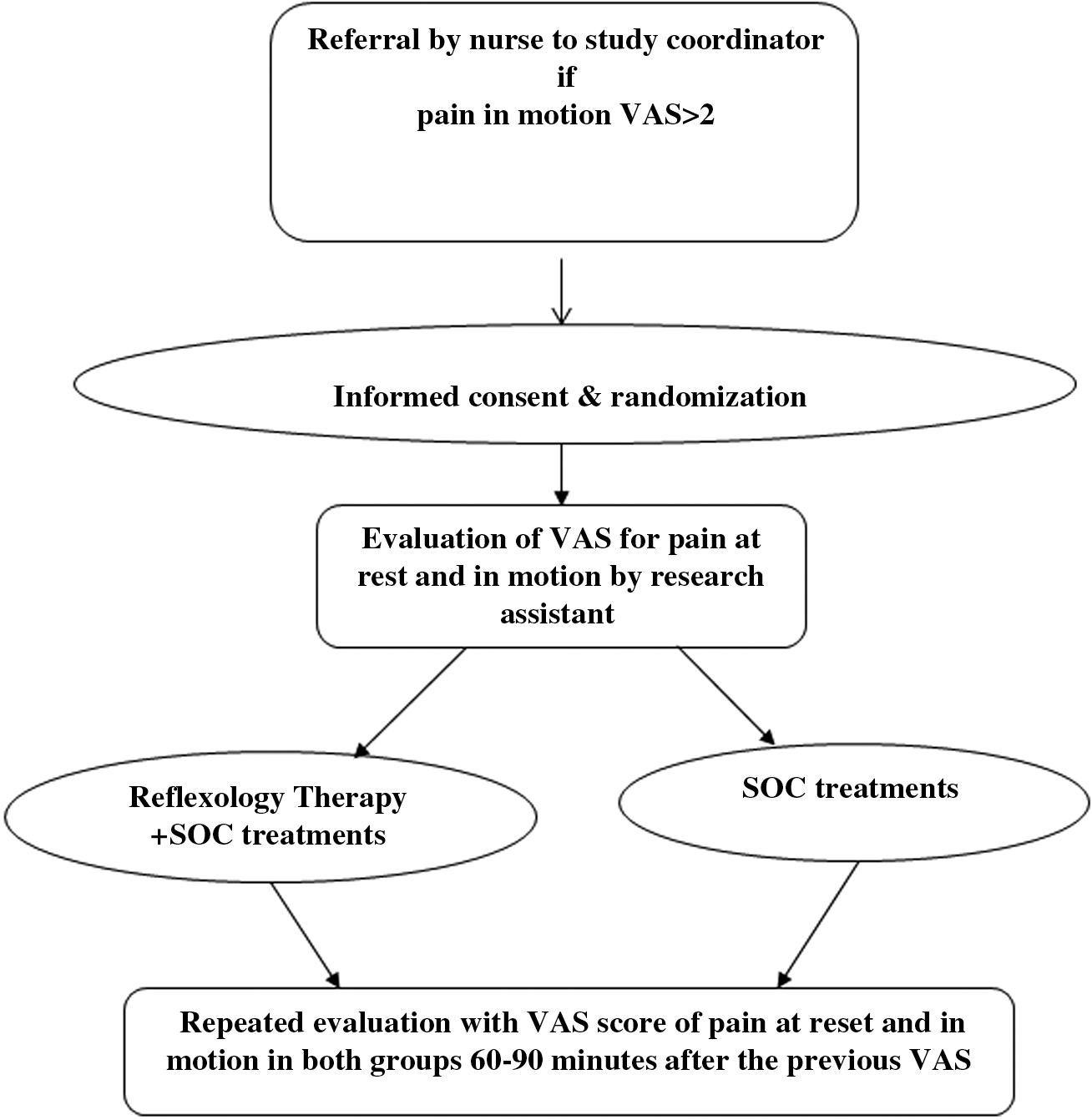
Research procedure in the surgery department. SOC, standard of care; VAS, visual analog scale.
Research tools
Before reflexology treatment, pain was assessed using the VAS. This questionnaire is based on the validated Edmonton Symptom Assessment questionnaire 10 assessing pain during motion and pain at rest on a scale ranging from 0 to 10, where 0 indicates a lack of symptoms and 10 expresses the maximum intensity of the symptom. Note that the patients were asked specifically about pain in the area of the operation. If they reported pain in some other area, for example a headache, this was considered a new complaint to be assessed separately and was not included in this research. A result of VAS >4 represents moderate to severe pain. 11
Therapeutic tools
Therapeutic approach using reflexology
Five experienced reflexologists formulated the therapeutic reflexology protocol. All therapists studied reflexology for 2 years, had at least 5 years of experience as reflexologists in ambulatory settings, and 2 years in treating in-patients. Three of the five reflexologists administered the treatments in this study. The therapeutic protocol included a preparatory period consisting of several minutes of gentle and nonspecific foot massage, followed by a shift to the reflex points regarded according to reflexology as representing the spinal column, sinuses, and the solar plexus for relaxation purposes. 11 After that, the treatment focused on the pain by massaging the reflex point associated with the target organ and reflex points associated with the affected system according to reflexology maps (e.g., esophagus, stomach, and intestine reflex points after intestinal surgery). In addition, reflex points of the areas that innervate the target organ were also massaged. The treatment lasted around 20 min. Treatment safety was assessed by the reflexologist following treatment. Patients were asked if there was any discomfort regarding treatment.
Analgesic drug treatment
The drug treatment was administered to the patients in accordance to standard clinical directives for alleviating pain. While the department uses standard therapeutic approaches to pain alleviation, there is no uniform protocol defining the drugs given to each patient (according to type of surgery or level of pain). The most common drugs used are paracetamol, dipyrone, nonsteroidal anti-inflammatory drugs, and opioids.
Outcome measures
The primary outcome measure is short-term pain reduction following referral to study. Reflexology treatment was defined as the independent variable and pain symptoms at rest and in motion as the dependent variable. Three reflexologists carried out the intervention according to the study protocol. To reduce the potential for data deviation stemming from more than one therapist, we standardized the therapeutic approach by writing an official protocol. The protocol was implemented through several meetings dedicated to this purpose and by adding assessment of the actual treatment.
Materials and auxiliary aids
The study coordinators used an iPad equipped with software for assessing VAS (Statuscope TM) that included patient details, personal and demographic data, place of treatment, and the VAS pain assessment questionnaire. The reflexology treatment involved the use of a reflexology cream comprising the following components: coconut oil, sweet almond oil, shea butter, cera alba, isopropyl myristate, lanolin, propyl parabenmethyl paraben, phenoxy ethanol, butylated hydroxytoluene, and peppermint oil.
Statistical methods
Sample size was calculated using GPower software in accordance with customary research standards of 95% confidence level and 80% power. A minimal sample size of 55 patients in each group was required to show an average difference of 15 mm in VAS units, with a standard deviation of 28 mm. This difference might be considered as a “medium” effect. 12 The differences in quantitative measures between the intervention group and the control group (e.g., age) were examined by Mann–Whitney test or t-test, in accordance to distribution of the quantitative measure. Repeated measures analyses were conducted to examine the relation between level of pain (at rest and in motion) at the two measurement points according to intervention or control group, standardized for age and gender. Note that the median value was also chosen as a measure for comparison because the data are not normally distributed. Significance was reached at p < 0.05.
Results
The research participants comprised 164 patients hospitalized in the surgery department, 77 in the intervention group and 87 in the control group, a total of 164 treatments. Around 11% of the patients we approached to participate in the study refused to participate. The reasons for their refusal were not documented. The average age in each group was ∼47 (Table 1), with no statistical difference (p = 0.98) between the intervention and control groups. The research group consisted of 87% women, compared to 60% in the control group (p < 0.0001). The research participants underwent diverse surgical procedures that were divided into six categories according to surgical approach and surgical location. The frequency of laparoscopic and breast surgery differed statistically between the two research groups (p = 0.02 and p = 0.006, respectively). For all the other categories there was no statistical difference between the two groups (Table 1).
SC, standard care; SD, standard deviation.
Time of data collection
The median time that elapsed between the two assessments was 1 h and 25 min (minimum 00.25.00–maximum 02.55.09) for all the participants in the research. In addition to the assessment of pain, ranging from 0 to 10 VAS units at rest and in motion, the results were also analyzed according to pain rated moderate and above, that is VAS exceeding 4 (4–10) at rest and in motion. The average initial level of pain at rest and in motion was similar for the two groups, without statistical significance (Table 2). From 50% to 76% of the research population reported moderate to severe pain at rest and in motion, respectively (Table 2).
SC, standard care; SD, standard deviation; VAS, visual analog scale.
Assessment of pain at rest (VAS 0–10)
In the treatment group, pain intensity at rest decreased from 4.40 ± 2.75 to 3.13 ± 2.37 (p < 0.0001) while no significant change was observed in controls (from 4.74 ± 2.73 in baseline to 4.66 ± 2.9, p = 0.92; Fig. 2; Table 3).

Change in mean pain level (at rest and in motion)—standard care versus reflexology. VAS, visual analog scale.
SC, standard care; SD, standard deviation.
Assessment of pain in motion (VAS 0–10)
In the treatment group, pain intensity in movement decreased from 6.25 ± 3.08 to 1.18 ± 2.54 (p < 0.0001) while no significant change was observed in controls (from 5.84 ± 3.16 in baseline to 5.72 ± 3.09, p = 0.65; Fig. 2; Table 3).
Assessment of moderate to severe pain at rest (VAS >4)
In the treatment group, pain intensity at rest (moderate to severe) decreased from 6.66 ± 1.78 to 4.18 ± 2.30 (p < 0.0001) while no significant change was observed in controls (from 6.41 ± 1.55 in baseline to 5.99 ± 2.39, p = 0.23; Fig. 3; Table 3).

Change in mean pain level for moderate to severe pain (VAS >4) (at rest and in motion)—standard care versus reflexology. VAS, visual analog scale.
Assessment of moderate to severe pain in motion (VAS >4)
In the treatment group, pain intensity in movement (moderate to severe) decreased from 7.70 ± 1.76 to 4.86 ± 2.38 (p < 0.0001) while no significant change was observed in controls (from 7.67 ± 1.84 in baseline to 7.15 ± 2.45, p = 0.12; Fig. 3; Table 3).
Safety
During the research period, no significant side effects of the reflexology treatments were observed. One patient indicated that he was unable to fall asleep during the night after treatment, felt restless, and was overwhelmed with emotions, attributing these feelings to the reflexology treatment. Side effects of the drug treatment were not documented for either of the two groups.
Discussion
Our research assessed the hypothesis that reflexology can contribute to the challenge of postoperative pain management. The research results point to a large improvement in level of pain at rest and in motion after reflexology in addition to standard analgesic treatment compared to standard drug treatment only. This observation has significant ramifications in the current reality where postoperative pain remains a significant problem and constitutes a barrier to patient satisfaction, despite available treatment options. The reflexology group included more women and this difference was statistically significant. This difference may have potentially occurred randomly. Despite the gender difference, the initial level of pain at rest and in motion was similar in the two research groups. This is in accordance with the findings in the literature that contrary to prevailing assumptions, patient gender is not a predictor of pain or of consumption of analgesics. 13 The distribution of laparoscopic and breast surgery differed statistically between the two research groups. For all the other categories—open abdominal surgery (laparotomy), perianal surgery, thyroid, and other—there was no statistical difference in distribution between the two groups. When considering type of surgical procedure as the main predictor of postoperative pain and pain intensity, the initial pain intensity, which is similar in the two groups as discussed below, is provided to indicate that there is no statistical significance to the distribution of type of surgery between the two groups. Of the 164 patients included in the research, 60% reported their initial pain at rest as moderate to severe (VAS ≥4) and 70% assessed their initial pain in motion as moderate to severe (96 and 116 out of 164 patients, respectively). This finding indicates that pain management is not optimal, similar to that described in the literature 14 and underscores the medical challenge presented by postoperative pain. The initial pain intensity in both groups was measured under the influence of standard analgesic treatment in the department, and did not differ statistically. This implies that analgesic approach was quite constant, although suboptimal. A comparison between the mean or median changes in assessments of pain at rest and pain in motion reveals a greater decrease for pain in motion. Reducing pain in motion, is an important outcome since it may allow early patient mobilization. However, this needs to be assessed specifically. This points to the importance of two assessments of postoperative pain—one for pain at rest and one for pain in motion. The reliability of VAS as a research tool for assessing pain has been the subject of much discussion. One question that has arisen refers to the degree of change in VAS that has clinical significance and reflects an improvement in pain level as experienced by the patient. A study of 96 patients in an emergency room setting determined that a change of 13 mm in VAS represents the minimal measured change in pain intensity experienced by patients as “a little less pain” or “a little more pain.” 15 The average improvement in assessed pain at rest and in motion among patients with VAS >4 was 1.98 for pain at rest and 2.96 for pain in motion. This change is more than two times greater than the minimal measured change in pain intensity reflecting clinical improvement, as determined by Gallagher et al. 15 Some research studies show a correlation between expectations and results in complementary medicine, while others show the opposite. 16,17 This issue was not examined in the current study. It would be advisable to clarify whether the component of therapeutic belief or expectation plays a role in enhancing the therapeutic effect. Other effects, such as ritual, attention, empathy, and therapist–patient relations, may likely also be influential factors.
Limitations
Although the results of this research indicate that reflexology leads to a decrease in the intensity of postoperative pain, the results may not be suitable for all surgical patients. The literature describes controversies regarding the precise location of the different reflex points. 18 Hence, future research should use a Delphi procedure to formulate the reflexology protocol, as is often done in studies involving acupuncture. 19 Around 11% of the patients we asked to participate in the research refused. We have no sociodemographic or medical characteristics for this population, nor do we know about their position regarding complementary medicine. In view of this, we cannot evaluate the impact of this population on the research results. Another limitation is the lack of a sham reflexology group, that is, a group that undergoes nonspecific foot massage. It can be assumed that a heightened placebo effect would emerge in individual treatments merely from the human contact. With respect to the drug treatment, neither dosage nor timing of analgesic drug treatment in the research group was documented, and pain treatment in accordance with documented VAS was not standardized. Drug treatment was administered as customary in the department, and the pain assessments in the control group were not at set times in accordance with the drug treatment but rather were random. It is possible that some of the effect of reflexology on pain scores could be residual pain management from pain medications. However, this is exactly the point of integrative care. Ultimately, we are less interested in whether integrative care can, or should, replace other forms of pain management but rather can it be used as safely and effectively as current pain management approaches. 20 Another potential limitation is the random assignment to groups according to the reflexologists' days of work. This type of assignment is described in the literature as suboptimal randomization. The gender difference between the groups and the difference in the distribution of types of surgery did not corroborate this assumption. On the other hand, the similarities between the groups (age and level of basic symptoms) support our assumption. We also did not gather data regarding patient belief and expectation from reflexology since there was no valid questionnaire to that end. It is strongly suggested that future studies assess these domains. Of note, a questionnaire was recently developed and validated by our group to evaluate belief, expectations, and attitude toward reflexology in hospitalized patients. 21 Finally, we did not assess patient postoperative mobilization and length of stay. These outcomes are important in terms of early recovery, and economic burden, and should be specifically evaluated in future trials.
Conclusion
Our research indicates that the conjunction of reflexology with standard drug treatment has a positive impact on reducing postoperative pain. Particularly apparent is the clinically significant decrease in pain for moderate to severe pain (VAS ≥4) at rest and in motion. These results place reflexology as a potential intervention in the multidisciplinary treatments of the challenging phenomenon of postoperative pain. Reflexology treatment takes place at the patient's bedside, has no major side effects, and is not dependent on the patient's linguistic knowledge or cognitive level, thus making it suitable for a broad population group. Future research should include a sham reflexology group and assessment of the differential contribution of analgesics.
Footnotes
Acknowledgments
We thank Ronit Leiba for statistical processing, and Ilana Merhav and Tanya Kligerman, librarians at the Bnai-Zion Medical Center, for their assistance in the literature search. We also would like to thank Sarah Ben Shlosh and Shlomit Grimberg for evaluation of symptoms in patients for the research.
Author Disclosure Statement
No competing financial interests exist.