
Abstract
Objectives:
Cognitive decline, depression, and anxiety are among the major concerns in patients undergoing coronary artery bypass grafting (CABG). Crocus sativus L. (saffron) seems to be a promising candidate for treatment of these conditions.
Design:
In this 12-week, randomized, double-blind, placebo-controlled clinical trial, men and women with on-pump CABG, who had Wechsler Memory Scale (WMS) score >70 and age <70 years, received either saffron capsules (15 mg/twice daily) or placebo. Patients were excluded if they had history of treatment with saffron or acetylcholinesterase inhibitors, comorbid neuropsychiatric disorders, serious medical conditions other than cardiovascular diseases, and hypersensitivity to herbal compounds. The primary outcome was defined as the difference in mean total score changes for WMS-Revised from the baseline to week 12 between the saffron and placebo groups. Secondary outcomes included difference in mean score changes from baseline to endpoint between the two treatment groups for Mini Mental Status Examination and subscales of Hospital Anxiety and Depression Scale (
Results:
No significant difference was detected in primary or secondary outcomes between the saffron and placebo groups. Also, no significant time × treatment interaction effect was found for any of the scales.
Conclusions:
The results of this trial do not support the hypothesis of potential benefits of saffron in treatment of CABG-related neuropsychiatric conditions.
Introduction
D
To date, different interventional methods have been used to alleviate depression and anxiety in patients with CABG. 10 –13 Nonpharmacologic interventions yielded controversial results in short term, 10,11 and among the few pharmacologic interventions only simvastatin had promising short-term effects. 12,13 Interestingly, Crocus sativus L. showed comparable effects to fluoxetine in patients with mild-to-moderate depression subsequent to percutaneous coronary intervention (PCI). 14 Crocus sativus (saffron) and its major constituent crocin have attracted attention in recent decades because of their therapeutic effects on a wide range of medical conditions, including neuropsychiatric disorders and cardiovascular diseases. 15 –17
Saffron promoted cognitive function, especially memory, 18 in Alzheimer's disease patients to an extent that was comparable to donepezil and memantine. 19 –21 Also, it reversed memory deficit, protected against neuronal injury, and improved recognition, learning behavior, and spatial memory in animal models. 22 –26 These effects are supposed to be due to inhibitory effects of saffron on β-amyloid fibrillization, 27 –30 acetylcholinesterase activity, 31,32 hippocampal long-term potentiation, 33 and extracellular glutamate levels, 34 –38 as well as regulatory effects on neuroinflammation and endoplasmic reticulum stress, which are the two mechanisms underlying inflammatory demyelination and neurodegeneration. 39 Similarly, recent systematic review and meta-analysis reported significant antidepressant activity for saffron in patients with depression. 40,41 These effects are suggested to be even comparable to some conventional antidepressant medications, including fluoxetine, 42,43 and imipramine, 44 and are supposed to be rooted in serotonergic, antioxidant, anti-inflammatory, neuroendocrine, and neuroprotective mechanisms of action. 40 Concerning application of saffron in anxiety, the results of few available studies seem promising. 15,45
Besides these neuropsychiatric effects, saffron attenuates atherosclerosis, 46 myocardial injuries, 47 cardiotoxcity, 48 and development of insulin resistance, 49 through antioxidant, radical scavenging, hypolipidemic, and hypotensive effects. 50 –54
To our knowledge, despite the efficacy and good safety profile of saffron in previous clinical studies, 15,55 there is no evidence concerning application of saffron in patients with cognitive impairment, depression, or anxiety who are subject to cardiovascular surgeries. Such studies are among recommended investigations by recent comprehensive reviews. 18,55 In this trial, the authors assessed the effects of saffron on cognition, anxiety, and depression in post-CABG patients through a randomized, double-blind, placebo-controlled trial. The primary outcome of interest was the mean difference in change of total score for Wechsler Memory Scale-Revised (WMS-R) from baseline to endpoint between the saffron and placebo groups.
Methods
Trial design
In this double-blind, placebo-controlled, parallel-group, clinical trial, on-pump CABG candidates were randomized to receive either saffron or placebo for 12 weeks. The trial protocol was approved by the Institutional Review Board of the Tehran University of Medical Sciences in accordance with the World Medical Association (Declaration of Helsinki, as revised in Brazil 2013) code of ethics and was registered at the Iranian Registry of Clinical Trials (
Participants
Participants were selected from men and women referred for on-pump CABG surgery to the Tehran Heart Center, Tehran, Iran, from September 2014 to December 2015. These individuals were hospitalized at least 3 days before the surgery and remained hospitalized for at least 3 days after the surgery. Patients <70 years and who had a WMS-R score >70 were included. They were excluded if any of the following conditions existed: history of treatment with saffron, acetylcholinesterase inhibitors, antidepressants, or warfarin; comorbid psychiatric or neurodegenerative disorders based on the Diagnostic and Statistical Manual of Mental Disorders-IV-Text Revision; serious medical conditions other than cardiovascular diseases; and hypersensitivity to herbal compounds. Patients were also excluded from the study in case of inability to communicate. Written informed consent was obtained from all participants and their legally authorized representatives. The participants were informed that they were free to withdraw from the study at any time.
Intervention
Patients were randomized to receive either saffron capsules (IMPIRAN, Iran) or placebo in 15 mg doses twice per day from 2 days before the CABG surgery up to 12 weeks afterward. At each visit, besides counting the pills, patients and their caregivers were asked about the patients' compliance with the medications. It was required that the patients do not receive cognitive behavioral therapy during the course of the study and stop taking psychotropic medications or any sedatives at least 48 h before each evaluation visit.
Preparation of saffron capsules
Saffron capsules were prepared based on a precise protocol. Using a three-step percolation procedure, 120 g of dried and milled Crocus sativus L. stigma was processed with 1800 mL of ethanol (80%). Then, the ethanol extract was evaporated at 35°C–40°C to result in dried extract. Each capsule consisted of saffron extract (15 mg), lactose as filler, magnesium stearate as lubricant, and sodium starch glycolate as disintegrant. To standardize each capsule based on crocin content, drug samples were evaluated for major saffron constituents, crocin and safranal, through spectrophotometry with respective direct absorbance readings of 330 and 440 nm. The final capsules contained 1.65–1.75 mg of crocin.
Outcomes
The WMS-R 56 and Mini Mental Status Examination (MMSE) 57 were used for assessment of cognitive function in participants at the preoperative baseline visit, 1 week after surgery, 1 month after surgery, and at the endpoint visit. The WMS-R consists of 5 domains: verbal, visual, general, attention, and delay. Hospital Anxiety and Depression Scale (HADS) was used for assessment of anxiety and depression states. 58 All the WMS-R, MMSE, and HADS have been applied in previous clinical trials in the Iranian population. 19,21,59 –62
The primary single outcome of interest was the difference in WMS-R total score changes from baseline to endpoint at week 12 between the saffron and placebo groups. The secondary outcomes were defined as the difference in score changes from baseline to endpoint between the two treatment groups for MMSE, HADS anxiety subscale, and HADS depression subscale. Time × treatment interaction effect was evaluated for all the scales.
Safety
Participants and their caregivers were encouraged to immediately report any unexpected symptoms or changes in patients' status during the trial. Patients were visited on a daily basis by a psychiatrist to check for potential delirium status. In addition, a comprehensive symptom checklist was used at each visit followed by open-ended questioning for adverse events. Patients were thoroughly examined at baseline and each follow-up visit. Neuropsychiatric evaluation and assessment of adverse events were completed by independent raters. In case of any adverse events, a consulting neurologist was responsible to decide on whether the medication should be discontinued or not. Preoperative evaluations were performed at baseline, and postoperative cardiopulmonary workups were done according to the standard of care.
Sample size
Based on previous trials, a difference of 1.8 on the WMS-R total score change, a standard deviation (SD) of 2, a two-sided significance of 5%, and a power of 80% were assumed for calculation of sample size considering a potential 50% dropout rate. The final calculated sample size was 76.
Randomization, allocation concealment, and blinding
Using computerized random number generation, an independent person randomized the patients to saffron or placebo groups in a 1:1 ratio. Allocation concealment was achieved using sequentially numbered, sealed, opaque envelopes. Rating and random allocation were done by separate independent entities. Identical containers were used to pack the medications with participants' code numbers on them. Medications were dispensed by an investigational drug pharmacist. Placebo capsules had identical coat, shape, size, odor, texture, and color to the saffron capsules. All the patients and their caregivers, the clinicians who referred the patients, and research team members, including the rater physicians, were blind to the treatment assignments.
Statistical methods
The IBM SPSS Statistics 20.0.0 (IBM Corporations) and SigmaPlot 12.2.0 (SYSTAT Software, Incorporated) were used for analysis and drawing plots, respectively. Number (%) and mean (±SD) formats were used to report respective categorical and continuous variables. Mean (95% confidence intervals [95%CIs]) format was used to report mean differences between groups. The Cohen's d (95% CI) was the choice measure of effect size. Independent samples t-test, chi-square test, and Fisher's exact test were applied to compare continuous and categorical data where appropriate. Whenever the assumption of equality of variances was violated based on Levene's test results, degrees of freedom and concordant p-values were corrected. Both complete case analysis and intention-to-treat analysis were applied. For intention-to-treat analysis, last observation carried forward procedure was used to impute the missing data before calculation of mean score changes. Also, as the most reliable and a widely applied method of intention-to-treat analysis in clinical trials with missing data, mixed linear regression models were used for estimation of time × treatment interactions considering time (three levels: baseline, week 4, week 12), treatment (two levels: saffron, placebo), and their interaction as fixed-effect covariates. A random intercept was included in final models after comparing model fits with and without random slopes. Autoregressive covariance matrix was considered after exploratory correlation analysis. p-Value <0.5 was considered significant in all analyses.
Results
Participants and baseline characteristics
A total number of 378 patients were screened out of whom 76 participants were randomized into the saffron and placebo groups equally (Fig. 1). Subsequently, 22 and 23 patients met the first postbaseline visit in saffron and placebo groups, respectively. Finally, 18 and 19 patients completed the study in the respective saffron and placebo groups.
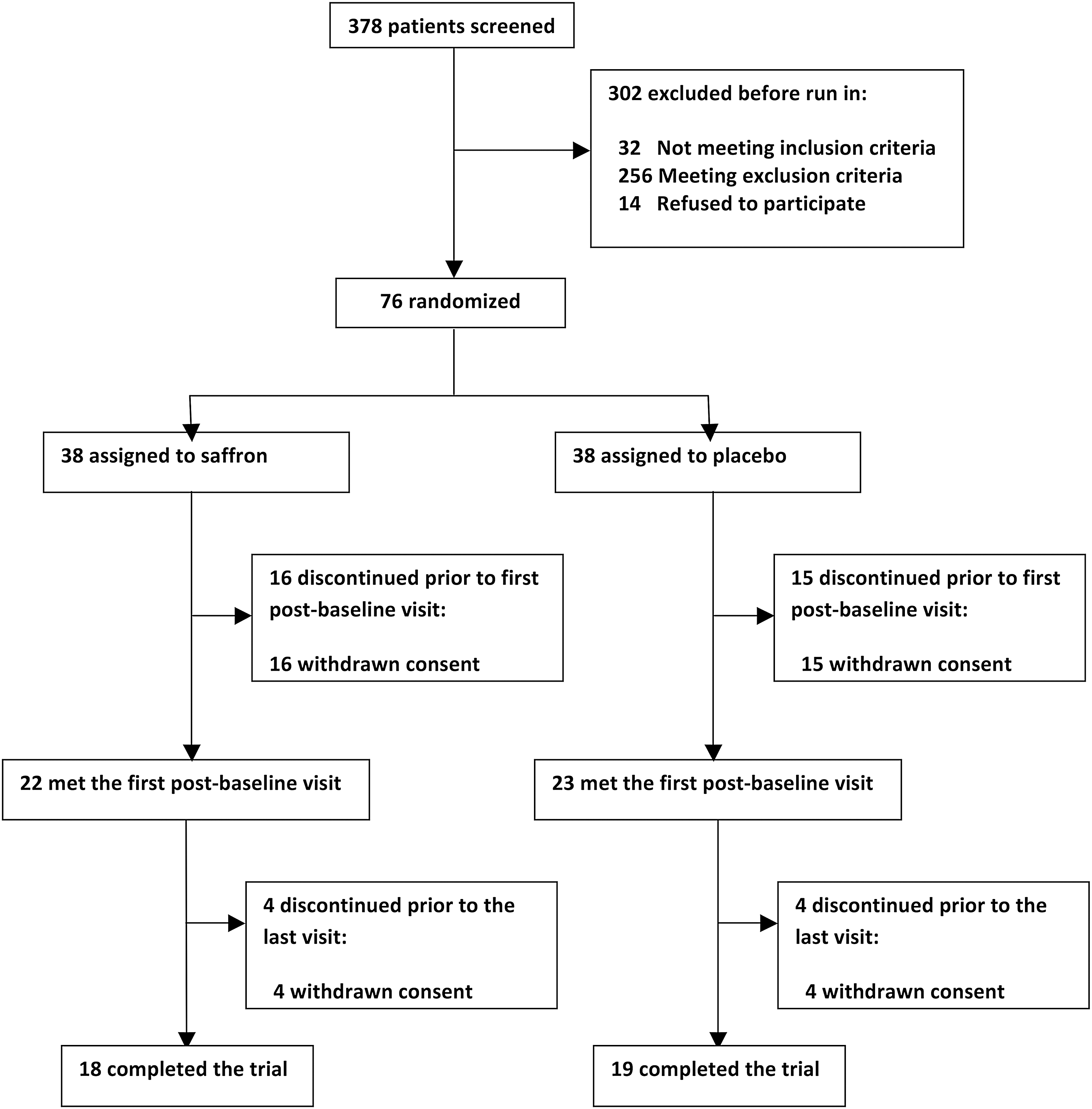
Flow diagram of patients undergoing coronary artery bypass grafting.
No significant difference was found between saffron and placebo groups regarding baseline sociodemographics (Table 1).
SD, standard deviation.
Outcomes
No significant difference was found in baseline scores, or score changes during the trial between the saffron and placebo groups for any of the scales (Table 2), including WMS-R, MMSE, HADS anxiety, or HADS depression (Fig. 2). Also, no significant time × treatment interaction was detected.
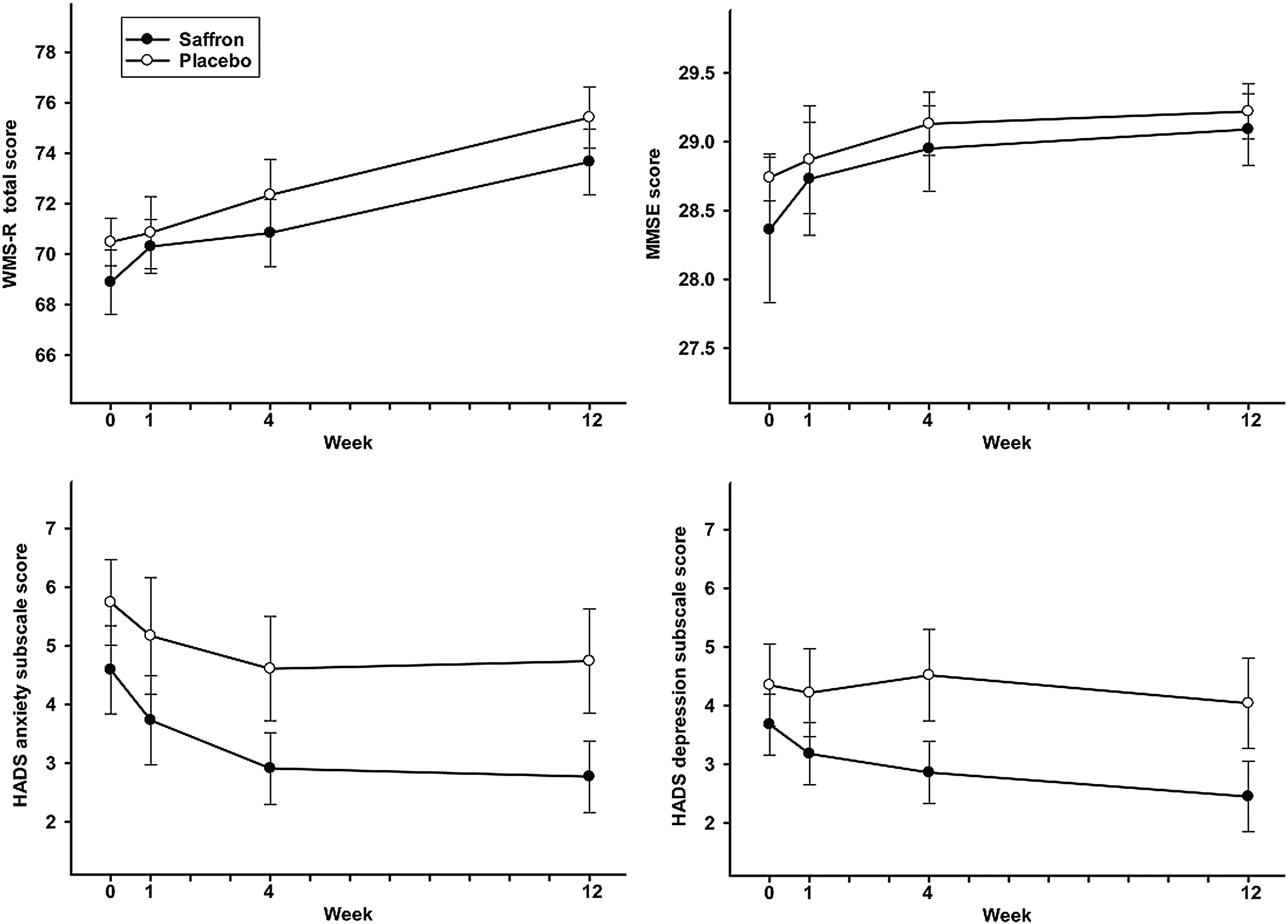
Comparison of WMS-R total score, MMSE score, and subscale scores of HADS between saffron and placebo arms in patients undergoing coronary artery bypass grafting. Values are represented as mean ± standard error of the mean at each time point. Independent-samples t-test was used to compare the score change from baseline to each time point between the two groups. HADS, Hospital Anxiety and Depression Scale; MMSE, Mini Mental Status Examination; WMS-R, Wechsler Memory Scale-Revised.
CI, confidence interval; HADS, Hospital Anxiety and Depression Scale; ITT, intention to treat; MMSE, Mini Mental Status Examination; SD, standard deviation; WMS-R, Wechsler Memory Scale-Revised.
Adverse events
Other than post-CABG surgery symptoms, which were comparable in both treatment arms, no adverse event was reported that could be associated with saffron or placebo.
Discussion
Post-CABG cognitive decline is a major concern, 1,2 and depression and anxiety symptoms are frequently experienced by patients undergoing CABG both before and after surgery, which is thought to affect the CABG outcome. 3 –5 The available body of evidence denotes the potential association between cognitive state, depression, and anxiety. 6 –9 While the effects of different interventional methods on these conditions have been a matter of controversial research for years, saffron appears as a therapeutic candidate due to its documented effects on cognition, 18 –21 depression, 40,41 and cardiovascular system. 46 –49
In this trial, the authors found no prominent difference between the saffron and placebo groups for mean score changes from baseline to endpoint neither for the WMS-R score as the measure of primary outcome nor for the MMSE and HADS depression/anxiety subscale scores. Also, they found no significant time × treatment interaction effect for any of the scales.
To our knowledge, this was the first trial of saffron in CABG patients concerning cognition, depression, or anxiety, and was among the few trials of pharmacologic interventions in these patients. These findings were inconsistent with the results of previous clinical trials of saffron showing cognition promoting effects in Alzheimer's disease 18 –21 and antidepressant effects in depression. 40,41 Also, these findings were inconsistent with the results of the most similar clinical trial in which the authors compared antidepressant effects of saffron to fluoxetine in patients with established mild-to-moderate depression who had gone under PCI in the last 6 months before the trial. 14 As a potential explanation for these inconsistencies, we can point out the differences in the pathophysiology of neuropsychiatric changes between perioperative conditions and chronic established states of cognitive decline (e.g., Alzheimer's disease) or depressive disorders (e.g., major depression). While intraoperative factors (e.g., disruption of cerebral perfusion) and preoperative patient-related factors (e.g., preexisting vascular disease) are discussed as risk factors for postoperative cognitive decline, 2,63 the pathophysiology behind the operation-related changes in cognition, depression, and anxiety remains unclear. 2 –4,63 In other words, it is plausible that the effects of saffron on these operation-related conditions cannot be simply compared with the effects of saffron on established conditions, including Alzheimer's disease and major depression. The fact that the effects of other interventional methods on CABG-related cognition decline and depression have been controversial so far is also another evidence supporting this explanation. 2,10,11,63
This trial was subject to some limitations. First, the sample size was relatively small with high rates of dropout in both arms. Meanwhile, it is noteworthy that all the dropouts in both groups were due to consent withdrawal rather than appearance of side-effects. In fact, patients who undergo CABG are hard to follow up in trials of adjunctive therapy as they tend to move between treatment settings, and many of them may not comply with the trial treatments as they receive several other medications. It is also common that patients mistakenly relate their postsurgery complications/adverse events to the trial treatments, and consequently withdraw from the study. Second, CABG patients are subject to different medical treatments, including anesthetics, analgesics, and benzodiazepines, which may conceal the net effects of saffron. Third, the authors used HADS for assessment of depressive and anxiety symptoms rather than other more comprehensive scales; however, the HADS has been used as a valid and reliable scale in previous clinical trials in patients with CABG. 64,65 Among the strengths of this study are the follow-up period of 12 weeks and measurement of cognition, depression, and anxiety simultaneously in CABG patients.
Conclusion
Overall, this trial did not support the hypothesis of saffron therapeutic effects in post-CABG cognitive decline or perioperative depression and anxiety; however, this was the first trial of saffron in patients with CABG. Further studies targeting the same population are not suggested unless a plausible rationale and a comprehensive design are proposed with a strict control for confounders. Future potential clinical trials will also benefit from bigger sample sizes to account for high rates of dropout in this population, but relatively the same 3-month period of follow-up as the major portion of fluctuations in mood and cognition in patients undergoing CABG happens within this period.
Footnotes
Acknowledgment
This study was supported by a grant from the Tehran University of Medical Sciences (Grant No. 23285).
Author Disclosure Statement
The authors declare that no competing financial interests exist. Tehran University of Medical Sciences had no role in the design, conduct, data collection, analysis, data interpretation, article preparation, review, final approval, or decision to submit this article for publication.