
Abstract
Objectives:
This pilot study compares the safety and efficacy of three treatments in reducing pain and improving fibromyalgia symptoms.
Design:
This study was an 8-week prospective, single center feasibility study.
Setting and Subjects:
Forty subjects were recruited from Solano, Sonoma, and Contra Costa counties of California in 2006–2009. Subjects were aged 18–65 and met the American College of Rheumatology (ACR) 1990 criteria for fibromyalgia.
Interventions:
This study had three treatment arms: gabapentin only (900 mg/day), osteopathic manipulative medicine (OMM) only, and combined treatment of gabapentin plus OMM. OMM treatment was administered by advanced medical students for 30 min, once a week. The trial lasted for 8 weeks, which included 6 weeks of treatment plus initial and final visits.
Outcome measures:
Key outcome measures included Wong-Baker FACES Pain Rating Scale (WBF), Clinical Global Impression of Health (CGI), Fibromyalgia Impact Questionnaire (FIQ), and number of tender points.
Results:
Twenty-nine subjects completed the trial; 8 subjects received gabapentin only, 11 patients received OMM only, and 10 patients received gabapentin plus OMM. Subjects receiving OMM alone and subjects receiving the combined treatment of OMM and gabapentin displayed clinical improvements based on WBF (p < 0.01 and p = 0.03, respectively), while the change among the gabapentin-only group was nonsignificant. The OMM only group was the only group to experience a significant decline in CGI scale (p < 0.01). No statistically significant changes were observed with the FIQ or number of tender points. No differences across groups were statistically significant. This is to be expected in a feasibility study with a small sample size.
Conclusions:
This pilot study suggests that OMM treatment and gabapentin are safe and clinically efficacious treatment of pain and other constitutional and somatic symptoms associated with fibromyalgia. A larger trial using the new ACR 2010 Fibromyalgia criteria is needed to confirm these findings.
Introduction
F
Treatment recommendations for fibromyalgia have been multidisciplinary and include pharmacologic tricyclic antidepressants, serotonin reuptake inhibitors, serotonin norepinephrine reuptake inhibitors, and pain modulating agents like Alpha 2 delta calcium channel ligands (gabapentinoids). 6 –8 Nonpharmacologic therapy for fibromyalgia has included cognitive behavioral therapy, graded exercise (swimming or walking), bio-feedback, physical therapy, occupational therapy, and sleep hygiene. 7 –10 In addition, some patients receive counseling on nutritional therapy, such as gluten free, paleo, and low-inflammatory dietary modifications, with the goal of achieving a healthy body mass index. 6,11,12
This study used the 1990 American College of Rheumatology (ACR) criteria for diagnosing fibromyalgia while enrolling patients from 2006–2009. 13,14 The ACR published revised criteria for the diagnosis of fibromyalgia in 2010. 10,15,16 The ACR 2010 fibromyalgia criteria recommend that tender points and Dolorimetry are no longer necessary for diagnosis. 10,15,16 The ACR 2010 criterion consists of two scales, the Widespread Pain Index (WPI) and the Symptom Severity (SS) Scale. 10,15,16 The ACR 2010 modified criteria by eliminating the physician estimate of the extent of somatic symptoms and substituted the sum of three self-reported symptoms. 10,15,16 They also created a 0–31 Fibromyalgia Symptom (FS) scale by adding the WPI to the modified SS scale. 10,15,16 This has made the diagnosis of fibromyalgia easier for clinicians and has allowed more patients to be considered for the diagnosis and treatment of this chronic pain disorder. 14 All participants in this study who met the 1990 criteria for fibromyalgia would also meet the criteria for diagnosis based on the 2010 guidelines. 14
Gabapentin is a common off-label treatment for fibromyalgia. 17 In preclinical pain models, gabapentin, a structural analog of the neurotransmitter gamma-aminobutyric acid (GABA), demonstrated analgesic and anti-allodynia effects in syndromes secondary to sensitization of pain responses. 18,19 The antinociceptive effects of gabapentin are hypothesized to be mediated by modulation of calcium channel ligand 2 binding, modulation of transmission of GABA, and potentially by additional unidentified mechanisms. 19,20
Osteopathic Manipulative Medicine (OMM) is a manual medicine treatment utilizing multiple modalities to restore proper structure and function to the musculoskeletal system. OMM has been used safely and effectively for a wide variety of conditions. 21 Risks of treatment include muscle soreness, headache, fatigue, and very rarely spinal cord injury or stroke with manipulation of the neck. OMM has been shown to be a safe effective treatment for fibromyalgia patients in preliminary research. 22,23
Materials and Methods
Setting and recruitment
The study was conducted at a primary care clinic in Vallejo, CA. Enrollment began in September 2006, and ended in April of 2009. Enrollment period was prolonged over 3 years because the investigators conducting the study were performing research on a part-time basis. Touro University's Institutional Review Board approved the protocol and consent process. Subjects were identified by physician referral, or responded to an advertisement for a fibromyalgia treatment trial. Subjects were recruited from Solano, Sonoma, and Contra Costa counties of California.
Male and female subjects were eligible for the study if they were 18–65 years of age and met the ACR 1990 criteria for fibromyalgia: pain must be present for 3 months or more at the time of enrollment in the study; subjects must have pain in 11 of the 18 tender point sites positive by Dolorimetry, where a 4 kg/cm2 pressure elicits pain. 13,14 The brand Dolorimeter used was the Chatillon manual dolorimeter that measured up to 10 kg/cm2 pressure applied using a rubber disc. Subjects' tender points were measured on week 1 and week 8. Subjects with other rheumatic or medical disorders that contributed to the symptoms of fibromyalgia were excluded.
Exclusion criteria consisted of the following: pain from traumatic injury or structural or regional rheumatic disease; rheumatoid arthritis, inflammatory arthritis, or autoimmune disease; unstable medical or psychiatric illness; lifetime history of schizophrenia, hypomania, mania, epilepsy, or dementia; substance abuse in the last 6 months; serious risk of suicide; pregnancy or breastfeeding; lack of contraceptive method in those of childbearing potential, and prior failed treatment with gabapentin, pregabalin, or OMM.
Sample size was determined by available recruitment of subjects, advertising, and the time period allotted by the IRB for funding. Sample size was also determined by the grant budget and the monies available in the grant to remunerate the subjects. A power study was not performed at the time of study design to determine the minimum number of subjects enrolled to give this study statistical significance. The sample size was determined by feasibility and recruitment resources. A more robust sample size of 63–120 participants would have allowed for more power, statistical significance, and the comparison of differences between groups.
Study design
Subjects were randomly assigned to one of the three treatment arms: (1) gabapentin only, (2) OMM only, and (3) combination treatment of OMM and gabapentin. Randomization was assigned as a computer generated number labeled on the laboratory values of the subjects as they returned from the Quest Diagnostics. Their study manager placed the computer generated numbers on the laboratory results and sealed them in an envelope for the research administrator to assign the treatment arm on the first day of the study. Participants and researchers were not blinded to the treatment intervention to which they were assigned. Enrollment and randomization took place at the week 1 visit, as well as a review of medical history, physical examination, laboratory tests, tender point assessment, and baseline assessment of FS using questionnaires described below. The only person blinded to the study arm assignments was the person administering the tender point examination using the Dolorimeter on the first day of the study during the history and physical before participants knew which treatment arm they would be assigned. Subjects had weekly visits during the 6-week treatment period, followed by a final visit during week 8. Subjects were monitored weekly at each visit with vital signs, number of self-reported treatment reactions, and health/medication changes. Self-reported treatment reactions included muscle and joint tenderness, dizziness, headache, sedation, back pain, constipation, upset stomach, fatigue, vomiting, nervousness, decreased function, difficulty sleeping, nausea, tremor, dry mouth, increased appetite, unstable gait, change in vision, runny nose, and slurred speech. Subjects could choose from a checklist to select side-effect symptoms or write them in on the survey. The final treatment course was given at the week 7 visit, and subjects were seen for a final visit at week 8 to complete posttreatment study questionnaires and tender point assessment.
Subjects administered gabapentin (in the gabapentin only group and the combination treatment group) began with a 300 mg dose, once per day at bedtime for the first 3 days, then increased to 600 mg at bedtime for the next 3 days, and then 900 mg at bedtime for the remainder of the study. If a subject could not tolerate 900 mg/day at bedtime, the dosage was administered thrice a day at 300 mg per dose. During the tapering phase, the dosage was decreased by 300 mg at bedtime every 3 days until discontinuation.
Subjects receiving OMM treatment (in the OMM only group and the combination treatment group) received one 30-min treatment per week for 6 consecutive weeks (weeks 2–7 of the study). OMM treatment was provided by third and fourth year osteopathic medical students at Touro University College of Osteopathic Medicine. The students were supervised by an osteopathic physician with 16 years of practice experience, including the OMM modalities used in this study. Every treatment began with a structural examination, which generated the treatment modalities that the subject received that week. Treatment modalities included myofascial, muscle energy, counter strain, facilitated positional release, articular ligamentous, high velocity/low amplitude, and cranial sacral OMM. 21,23 OMM treatment began with indirect treatments, progressing to direct treatments if tolerated by the study subject. Tolerance was determined by asking subjects if the treatment was comfortable and okay to proceed. If the subjects voiced the OMM treatment uncomfortable due to pain the treatment was stopped and a different modality selected and applied instead.
Outcome measures
Outcomes were evaluated using the following tools: The Wong-Baker FACES Pain Rating Scale (WBF), 24 the Clinical Global Impression of Health (CGI) 25 , the Fibromyalgia Impact Questionnaire (FIQ), 26 and the 1990 ACR criteria for the diagnosis of fibromyalgia to determine tender points. 13,14 The primary outcome of this study is pain, the secondary outcome is improved impression of health, and the tertiary outcome is improved functional status. The number of tender points was measured as an exploratory outcome.
The WBF assesses average pain severity during the past 24 h on a 0–10 scale, where 0 indicates no pain and 10 indicates pain as bad as you can imagine. 24 WBF was assessed weekly from weeks 1 through 8. Changes in the brief pain inventory WBF are shown over time in Figure 2.
The CGI 25 assesses changes in overall health using a 1–7 scale, where 1 represents normal, or not ill, and 7 indicates extremely ill participants. CGI was assessed at weeks 1 and 8.
The overall impact of fibromyalgia was measured using the FIQ, 26 a self-administered questionnaire that is used to measure components of health status that are affected by fibromyalgia over the previous week. The total score ranges from 0 to 80; a higher score indicates a more adverse impact on life function. FIQ was assessed at weeks 1 and 8.
The tender point assessment checked subjects for tenderness at the 18 tender point sites as defined by the 1990 ACR criteria for the diagnosis of fibromyalgia. 13,14 The tender point assessment was done at weeks 1 and 8.
The treatment reaction survey followed number of side-effects from treatment during the weeks 2 through 8. A survey listing side-effects from gabapentin and OMM was listed on a survey checklist plus subjects could write in any unlisted side-effects they sustained during the research period. The number of side-effects, type of reaction documented, and severity level of side-effects were tracked over time. Treatment reactions over time are shown in Figure 3.
Statistical analysis
Subjects' characteristics and outcome measures (WBF, CGI, FIQ, tender points) at baseline were compared across treatment groups using analysis of variance (ANOVA). Within-group changes from baseline through study end were assessed using paired t tests. The change in outcomes was compared across treatment groups using ANOVA.
Results
Of the 40 subjects who were enrolled, 29 completed the trial. Five participants were excluded for: exceeding the age limit (n = 2), previous gabapentin use (n = 1), inadequate number of tender points (n = 1), and pregnancy (n = 1). Of the 35 subjects who were randomized, 12 were assigned to the gabapentin arm, 13 assigned to the OMM only arm, and 10 assigned to OMM plus gabapentin arm. Six patients dropped out before the end of the study, due to inadequate transportation (n = 3), self-reported treatment reactions of depression and weight gain (n = 2), and pregnancy (n = 1). The study flow chart is shown in Figure 1.
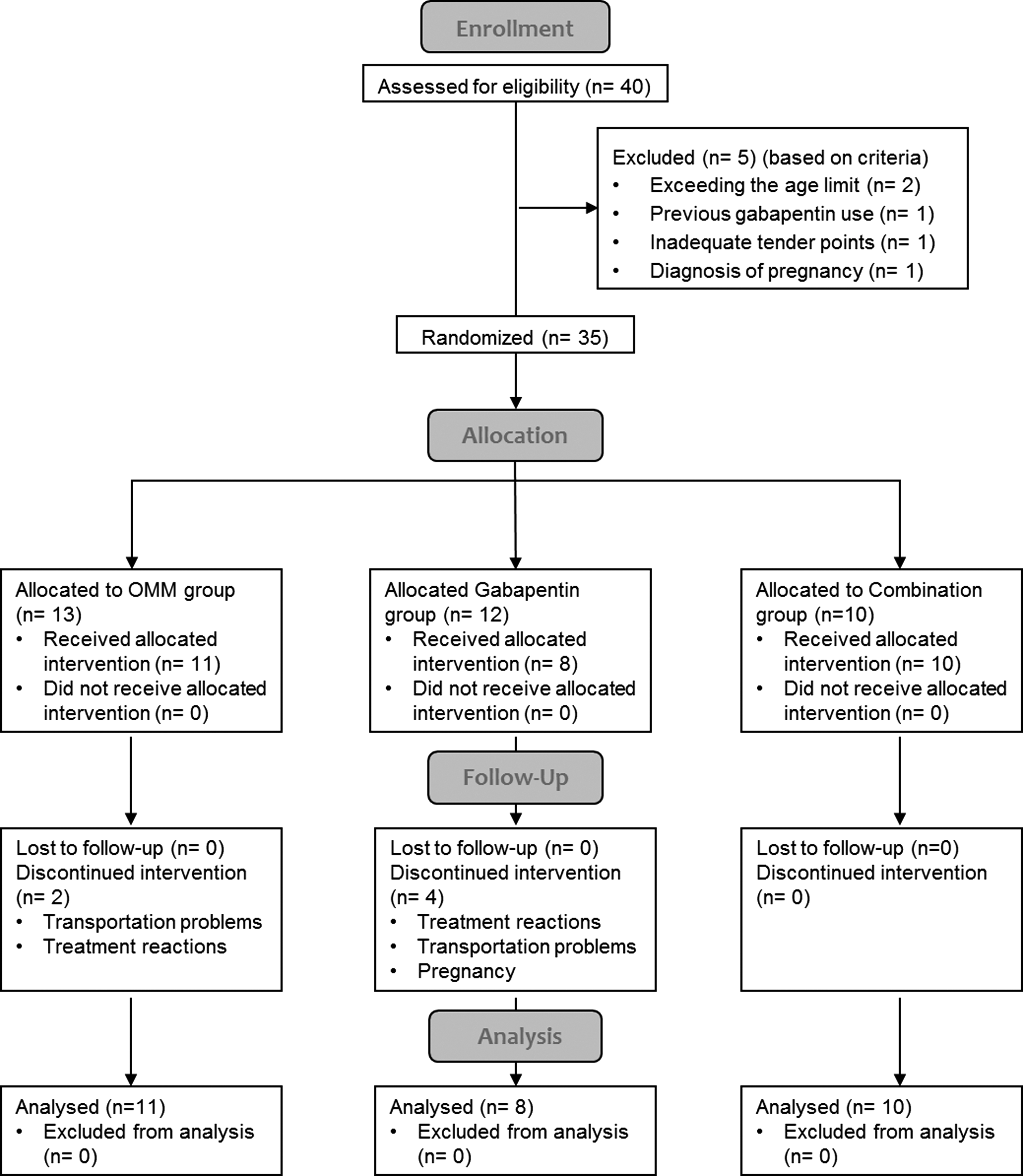
CONSORT flow diagram of study recruitment and participation. OMM, osteopathic manipulative medicine.
There were no significant differences between the treatment groups in demographic or clinical variables (Table 1). This is expected because the sample size is small. Table 1 shows that 18% of subjects in the OMM arm were the male subjects, with 0% in other arms. There were twice as many African Americans in the gabapentin arm compared to the OMM arm. The gabapentin arm was taking an average of 6.1 concurrent medications compared to the average 4.5 medication in the OMM arm. These could be considered as clinically significant differences. In this study, these patients were all taking a lot of concurrent medications. These drug–drug interaction effects between medications could be responsible for the treatment reactions in the treatment arms with gabapentin as treatment (Fig. 3). The majority of the patients were female and Caucasian, although African American and Latina patients also participated.
Testing for significant differences across treatment groups, using ANOVA.
Table 2 results represent the change in study outcomes from week 1 to week 8 of the trial. The WBF tool (range: 0–10) showed a significant decrease in self-reported pain in the OMM only group (mean difference, −2.4; p < 0.01) and in the combination group (mean difference, −2.9; p = 0.03). The gabapentin only group showed a slight but nonsignificant decline in WBF scores (mean difference, −0.6; p = 0.64). Figure 2 shows mean WBF score over time in weeks for each treatment group.

WBF average scores by treatment group over time. OMM, osteopathic manipulative medicine; WBF, Wong-Baker FACES Pain Rating Scale.
Testing for significant differences from week 2 to week 8 within treatment groups using paired t tests.
Indicates a statistically significant difference at α = 0.05.
Testing for significant differences in change of outcome across treatment groups (from week 2 to week 8) using ANOVA.
ANOVA, analysis of variance; CGI, the Clinical Global Impression of Health; CI, confidence interval; FIQ, Fibromyalgia Impact Questionnaire; OMM, osteopathic manipulative medicine; WBF, the Wong-Baker FACES Pain Rating Scale.
CGI scores (7-point scale) improved significantly in the OMM only group (mean difference, −1.3; p < 0.01), indicating that patients in this group felt better about their overall health and outlook on life at the week 8 endpoint. This change in CGI score represents a shift from feeling moderately ill at the inception of the study to feeling borderline ill at the end of the study. The combination group experienced a similar average change (mean difference, −1.3), which was not statistically significant (p = 0.12), while the gabapentin only group reported no significant changes in CGI scores (mean difference, 0.2; p = 0.73).
All treatment groups had lower average FIQ scores (range: 0–80) after 8 weeks of treatment, but the changes were not statistically significant in any group. Similarly, the mean number of tender points decreased in all groups, but none of the changes were statistically significant. No statistically significant differences were observed across study groups in the change in study outcomes (Table 2). The authors observed clinically significant improvement in the average FIQ score and the number of tender points over 8 weeks in all groups despite the lack of statistical significance.
Reported adverse reactions were mild-to-moderate in severity, and none required intervention (Fig. 3). The number of reported reactions decreased over time in all groups, with statistically significant decreases in the OMM only (mean difference, −5.7; p < 0.01) and combination groups (mean difference, −3.7; p = 0.03).

Average number of treatment reactions over time, by treatment group.
Discussion
This single center, randomized, parallel clinical pilot study of 29 patients compares the clinical effectiveness and safety of combined treatments of OMM and gabapentin, compared with each treatment alone, for reducing FS. After 8 weeks of treatment, the OMM only and combined treatment groups experienced significant improvements in the primary study outcome of pain (measured by WBF) and the OMM only group showed significant improvements in the secondary study outcome of overall perceived health (measured by CGI). Although all other changes in study outcomes were not statistically significant, Table 2 shows that all measures trend toward a clinical improvement, excluding the slight increase in average CGI for the gabapentin only group.
The between-group comparisons in Table 2, although not statistically significant, may be clinically significant by helping to distinguish the relative effects of the different treatments. For example, the combination group showed the largest improvement in average WBF and FIQ, while the OMM only group showed the largest reduction in average number of tender points.
Figure 1 is the CONSORT flow diagram, which shows the follow-up on all enrolled participants. Please note in this Figure 1 the disproportionate dropout rate in the gabapentin only group. Four out of the total six dropouts occurred in this group. In this study, those 4 of n = 12 equate to a 33% dropout rate compared to the 0% in the combination group. The authors postulate that the high dropout rate in the gabapentin arm is due to the higher side-effect profile of gabapentin and any drug–drug interactions in this group of participants (Fig. 3). This implies that gabapentin may not be as safe as OMM due to the higher side-effect profile and the potential drug–drug interactions.
Figure 2 shows that all three groups basically look the same from a statistical standpoint at 8 weeks, but from a clinical standpoint certain treatment arms might be more effective and safe. Subjective outcome measures of WBF, CGI, and FIQ did show some clinical improvement over time compared to the objective outcomes of number of tender points on examination.
There were larger improvements in the subjective outcome measures (WBF, CGI, FIQ, and general symptoms) than in the objective exploratory outcome measure (number of tender points). In a disease that is so fraught with somatic, affective, constitutional, and cognitive symptoms, an improvement in the patient's perception of their disease is considered an important improvement.
Several limitations of this study should be considered. There was no sample size or power calculation performed at the initiation of the study. The treatment groups were small, thus producing only hypothesis-generating data. This is problematic, because this pilot study is likely underpowered. Post hoc analysis found that a sample size of 21 participants per group would be needed to detect large effect size (Cohen's f = 0.4) at an α level of 0.05 and with 80% power. Larger adequately powered studies should continue to evaluate the impact of these treatments.
The results may not generalize to longer treatment periods due to the 8-week trial duration. The long-term efficacy of treatments should be explored in future clinical trials. OMM treatments were administered by osteopathic medical students who demonstrated special interest and skill in manipulation, supervised by trained and certified osteopathic physicians; it is possible that more experienced practitioners would be more effective in treating fibromyalgia. A generalized treatment protocol was used for all subjects, but each practitioner used clinical judgment to determine which treatments were most effective for individual subjects. Results may be difficult to reproduce among different practitioners. Furthermore, the gabapentin only group saw the clinician for a brief visit of 5 to 10 min, whereas those patients getting the OMM only or OMM plus gabapentin treatment spent 30 min face-to-face with their clinician. This difference in attention and physical contact impedes their ability to distinguish the impact of OMM from the effects of general personal contact or human interaction. Future research could include sham OMM or placebo to better isolate the impact of OMM therapy.
There were no adjustments for baseline covariates in this study. As such, this is really a feasibility study and pilot for the use of OMM, gabapentin, and combination therapy in the treatment of fibromyalgia.
The future larger trial would include a power analysis to determine appropriate sample sizes, the use of the new ACR 2010 Fibromyalgia diagnostic criteria, 10,15,16 and adjustment for potential confounding variables. After post hoc analysis, the authors propose that the future study be performed on 63–126 participants, to improve power size. The future study of the treatment of fibromyalgia with OMM, gabapentin, and combined treatment arms would use the following inclusion criteria: the WPI plus the FS severity score to equal the FS Scale as positive for the diagnosis of fibromyalgia. Primary outcomes would follow the WPI, the SS Scale, and Somatic Symptoms over time. Secondary outcomes would compare the treatment reaction profile over time. Exploratory outcomes could compare the PHQ-9 (depression/anxiety questionnaire) before and after the study. The authors hypothesize with larger treatment arms that there will be larger differences between groups that are statistically significant. The authors hypothesize that a future study designed as described above would show OMM to be more efficacious and safe compared to gabapentin.
Conclusions
This is the first study to evaluate the use of the combined treatments of gabapentin and OMM in the treatment of fibromyalgia. This pilot study suggests that OMM treatment and gabapentin may be a safe and effective treatment of pain and other constitutional and somatic symptoms associated with fibromyalgia. Additional research is needed to further support these findings and to help refine effective treatments for fibromyalgia to reduce the burden of this chronic pain condition.
Footnotes
Acknowledgments
This study was funded through an internal intramural grant submitted and approved by Touro University-CA, College of Osteopathic Medicine 2006–2009. Trial Registration: Fibromyalgia Treatment Trial with Gabapentin and Osteopathic Manipulative Medicine has been reviewed and is published on the
Author Disclosure Statement
No competing financial interests exist.