
Abstract
Objective:
Despite the recent re-emergence of the process of cupping by athletes, supporting evidence for its efficacy and safety remains scarce. This systematic review aims to summarize the evidence of clinical trials on cupping for athletes.
Methods:
SCOPUS, Cochrane Library, PubMed, AMED, and CNKI databases were searched from their inception to December 10, 2016. Randomized controlled trials on cupping therapy with no restriction regarding the technique, or cointerventions, were included, if they measured the effects of cupping compared with any other intervention on health and performance outcomes in professionals, semi-professionals, and leisure athletes. Data extraction and risk of bias assessment using the Cochrane Risk of Bias Tool were conducted independently by two pairs of reviewers.
Results:
Eleven trials with n = 498 participants from China, the United States, Greece, Iran, and the United Arab Emirates were included, reporting effects on different populations, including soccer, football, and handball players, swimmers, gymnasts, and track and field athletes of both amateur and professional nature. Cupping was applied between 1 and 20 times, in daily or weekly intervals, alone or in combination with, for example, acupuncture. Outcomes varied greatly from symptom intensity, recovery measures, functional measures, serum markers, and experimental outcomes. Cupping was reported as beneficial for perceptions of pain and disability, increased range of motion, and reductions in creatine kinase when compared to mostly untreated control groups. The majority of trials had an unclear or high risk of bias. None of the studies reported safety.
Conclusions:
No explicit recommendation for or against the use of cupping for athletes can be made. More studies are necessary for conclusive judgment on the efficacy and safety of cupping in athletes.
Introduction
I
Despite the long history and recent renewal of interest in the use of traditional medical techniques such as cupping, surprisingly little is still known about its efficacy and safety. Despite the lack of scientific evidence, recent studies suggest that cupping might benefit a variety of conditions that incorporate musculoskeletal pain, such as chronic neck pain 10 –13 or persistent nonspecific lower back pain. 14 –16 However, the scientific evidence on the use of cupping by athletic populations is limited, especially in regard to the potential benefits and purported mechanisms. Cupping, for example is thought to improve local microcirculation, thus improving transport of metabolic by-products such as lactate and therefore aid postexercise metabolic recovery. 17 Despite such speculation, there is a dearth of evidence as confirmed by experimental or clinical trials. Indeed paradoxically, recent experimental studies indicate that the acute effects of cupping might be related to an interruption of microcirculation in the tissues underneath the cupping glass, cutting off the oxygen supply during the cupping application. 18,19 In turn, such restriction of blood flow and the localized hypoxia induce subcutaneous increases in lactate concentrations. 18 Moderate acute local metabolic acidosis has been shown to result in local vasodilatation and improved microcirculation, 20 –22 and thus, the authors speculate that cupping might improve microcirculation on the longer term. 18 Of note, this theory is applicable to dry cupping only, and it should be noted that the bloodletting cupping does not incorporate the same mechanism. 5 In bloodletting cupping, incisions are made in the skin before the cupping vessels are applied, and blood that is thought to be stagnant, congested, 5 or containing toxins 23 is eliminated from the body and drawn into the cupping vessels.
This public display of cupping by prominent international athletes and the resultant media attention it garnered have been followed by a growing interest from the public and athletes alike as a method to enhance performance and recovery. 2,24,25 In consideration of the increased demand by athletes and sports people, and the lack of a systematic synthesis of clinical studies on cupping in athletes, this systematic review aims to summarize the evidence on the efficacy and safety of cupping for athletes and to inform the public, the athletes, and future research about the currently available evidence and its implications.
Materials and Methods
A protocol was developed using the Preferred Reporting Items for Systematic Review and Meta-analysis Protocols (PRISMA-P) 2015 Statement. 26
Search strategy
A database search was conducted on December 10, 2016, to identify original research investigating the effects of cupping in athletic populations, published with no date limits. The search included the following databases: SCOPUS, Cochrane Library, PubMed, AMED, and CNKI (China National Knowledge Infrastructure). The search terms employed were constructed around search terms for “cupping” and “athletes.” The following terms were excluded from the search: glaucoma and optic disc. Manual searching of Google Scholar, ProQuest, and reference lists of published articles on cupping was also conducted to ensure relevant known articles were included.
This is the complete search strategy for PubMed:
Eligibility criteria
Randomized controlled trials on athletes (professionals, semi-professional, and leisure sports persons) were included irrespective of gender and age. Eligible studies were those that examined the therapeutic effect of cupping therapy irrespective of the form, the tradition, frequency, and application of cupping. Studies combining cupping with any other interventions were considered as eligible and included in the review. Studies were included if they compared cupping to no treatment, placebo, conventional medication, or any other intervention. Studies were also included if they assessed athletic performance-related outcomes, including perceptions of pain, discomfort, physical function (self-report and objective measures), physical or mental performance measures, recovery-related measures, physiologic measures of stress, inflammation, or injury (serum or urine markers etc.), or health outcomes. For the purpose of this review, articles published in English, Chinese, and any other language were included if they were identified and deemed to meet the inclusion criteria. Furthermore, due to the expected paucity of trials, gray literature was also included if resulting from Bachelor, Master, or PhD theses or articles published in other than peer-reviewed journals so long as the inclusion criteria were met.
Review of records
All articles were imported into EndNote (version X7.5) and analyzed based on title, abstract, and full text. One author (R.B.) conducted the search and downloaded the results into EndNote. Two reviewers (R.B., R.L.) independently screened abstracts of records, and full texts of potentially eligible articles were retrieved. Full texts were read by two pairs of authors (R.B. and R.L., P.K. and R.L.) and based on that, the final list of eligible studies was compiled. If discrepancies between the two reviewers occurred, those items were discussed with a third reviewer to achieve a consensus. No disagreements regarding the inclusion of studies arose.
Data extraction
A data extraction form was developed a priori by the authors, and the data extractors were familiarized and trained to ensure comparable standards. Two pairs of authors (R.B. and R.L., P.K. and R.L.) extracted data independently; they included information such as reference, country of origin, study type, sample data (sample size, age, gender, and inclusion criteria), intervention data (treatment and control group), outcome data (dependent variable, measurement time points), and results data. If a disagreement occurred between the two reviewers, a discussion took place and if required a third reviewer familiar with the process was sought to achieve a consensus. No disagreements regarding independent data extraction arose.
Data synthesis
Due to the paucity of data collated, and the clinical and methodological diversity between studies that met the criteria for inclusion, it was deemed inappropriate to undertake a meta-analysis by the authors.
Risk of bias
The Cochrane Risk of Bias Tool 27 was used for a critical appraisal analysis of the included randomized control trials (RCTs). This tool assesses risk of bias on seven domains: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other sources of bias. Within each of these domains, the risk of bias was assessed as low, unclear, or high risk of bias. Risk of bias was assessed separately by two pairs of reviewers (R.B. and R.L., P.K. and R.L.), and in case of disagreements they were settled through a discussion with a third reviewer until consensus was achieved.
Results
Descriptive variables
The PRISMA flowchart of study inclusion is shown in Figure 1. Searches of the aforementioned databases and the other literature sources identified 88 possible citations, and following removal of duplicates, a pool of 79 citations remained. Sixty-six citations were deemed ineligible after title and abstract screening, and full-text articles were retrieved from 13 publications. Three of the publications reported the findings of 1 trial only, 28 –30 as such, 11 randomized controlled trials with n = 498 participants were then included in this review. 28 –40 Studies were published in English 30,36 –40 and Chinese 28 –35 ; and in a range of media outlets, including peer-reviewed journals, 30,38 –40 theses, 36,37 and other journals with unclear peer-reviewed processes. 28,29,31 –35
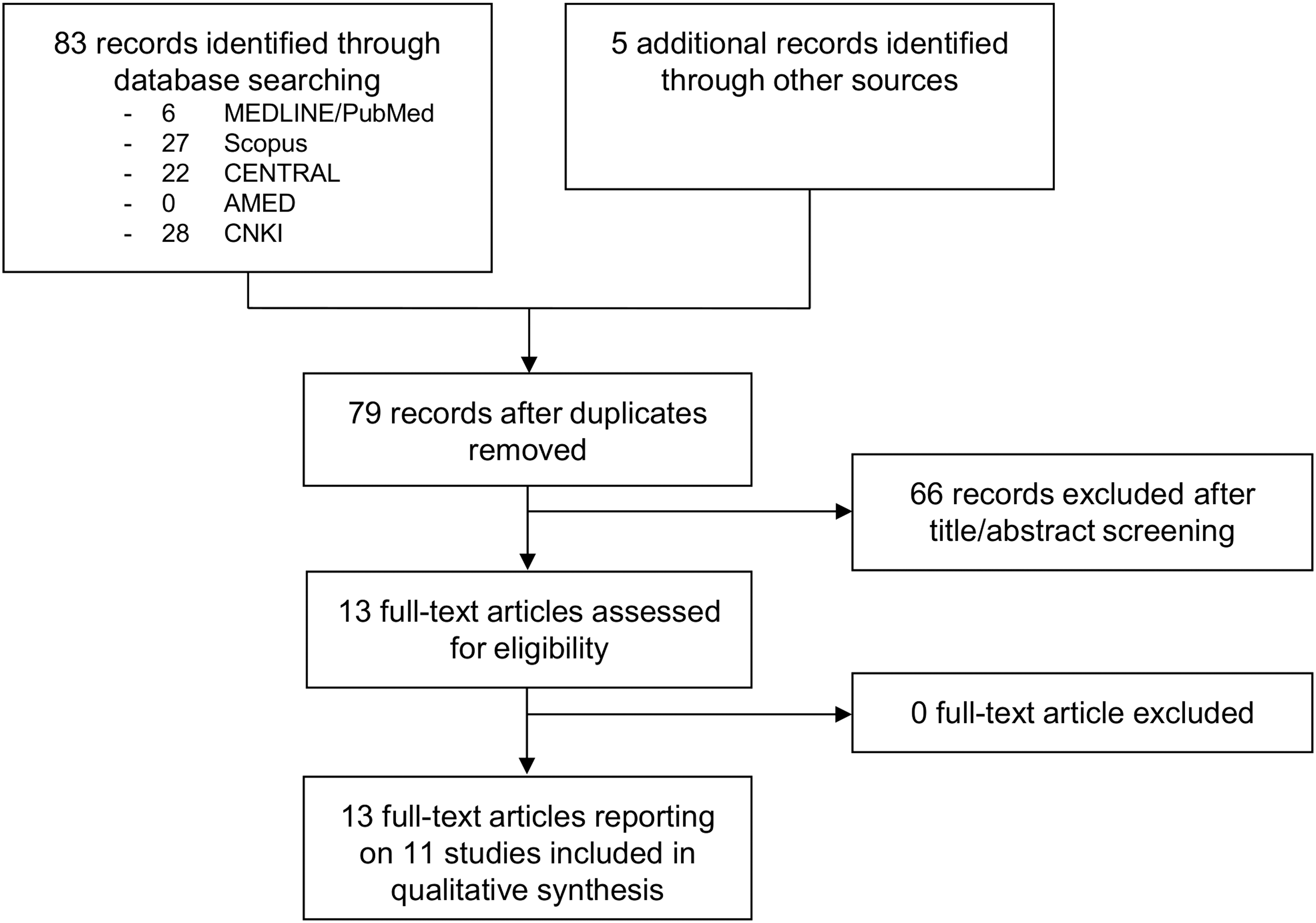
Preferred reporting items for systematic review and meta-analysis (PRISMA) flowchart of study selection.
Study characteristics are found in Table 1. One study each originated from Greece, 38 the United Arab Emirates, 40 and Iran, 39 two studies from the United States, 36,37 and six studies originated from China. 28 –35 While all studies were published between 1996 and 2016, the majority was published after 2010.
BUN, blood urea nitrogen; CK, creatine kinase; IE, isometric endurance; LD, lactate dehydrogenase; NA, not assessed; NR, not reported; PPT, pressure pain threshold; RMDQ, Roland Morris Disability Questionnaire; ROM, range of motion; ROM-ITB, Iliotibial Band Range of Motion; ROM-LWS, Lumbar Spine Range of Motion; RPE, Rated Perceived Exertion Scale; RT, reaction time; SCL-90, symptoms checklist; UR, urea; VAS, visual analog scale.
Sample sizes varied from 20 to 86 athletes with a median of 32 participants. Studies also varied regarding the athletes' demographics, ranging from amateur to professional athletes, from football, handball, and soccer players to gymnasts, swimmers, and field and track athletes, with healthy athletes or athletes specifically suffering from a variety of conditions, including back pain, 40 exercise-induced fatigue, 32 muscle strains, 34 sunstroke, 33 and heel pain. 31 Participants were of mixed gender in the majority of studies, 28 –31,33 –35,37 predominantly or exclusively male in other studies, 36,38,39 and two studies did not report participant gender. 32,40
Interventions
The treatment groups received a diverse range of cupping interventions, from cupping with 39,40 or without bleeding, 40 cupping massage, 35 and cupping was often applied in conjunction with other treatments. 28 –34,38 For example, one RCT used cupping in one group and cupping combined with stretching in another group, 36 three trials combined cupping with acupuncture, 31,33,34 one with moxibustion, 28 –30 and one trial combined cupping with instrument-assisted soft tissue techniques. 37 Cupping was applied between one and at least 20 times, over time periods ranging from 1 day 37,39 to 6 weeks. 36 As a note of observation, the majority of studies lacked a detailed description of the cupping procedures or the control group procedures. The number of applied control groups again varied in the trials, from one 33,37,39 up to five 38 control groups. Again, control group interventions included no treatment, 28 –30,32,35,38,40 instrument-assisted soft tissue techniques, 38 stretching, 36 massage, 32 massage combined with herbal crèmes, 31 exercise, 39 ischemic pressure, 38 electroacupuncture, acupressure, or moxibustion, 32 acupuncture combined with hot compresses, 34 and herbal medicine. 33
Outcome measures
A large variety of outcome measures were used, including self-reported measures of perceived pain, 34,38 disability, 40 exertion or fatigue, 28 –30,32 and other symptoms. 28 –30,34 Furthermore, measures used included pressure pain thresholds, 38 lumbar, 40 iliotibial band, 36 shoulder range of motion, 37 local skeletal muscle isometric endurance, 40 or reaction time. 32 More clinical-oriented systemic measures of inflammation, stress, and damage included serum creatine kinase, 28 –30,35,39 lactate dehydrogenase, 39 blood urea nitrogen, 28 –30 urea and urine parameters, 28 –30 and participant- and/or assessor-based judgment of recovery status and time to recovery. 31,33,34 Except for very few instruments, such as the Roland Morris Disability Questionnaire (back pain disability) or the SCL-90 (physical and psychologic symptoms), most studies did not provide detailed information about the application, validity, or reliability of the assessment processes for outcome measures. Finally, not one of the included studies assessed or reported safety of the cupping intervention.
Summary of findings
Cupping was found to be superior for perceived lower back and hip pain in soccer players when compared to no intervention, 38 while another trial found that more participants had recovered from heel pain after 2 weeks of acupuncture and cupping compared to a massage combined with a herbal cream. 31 In contrast, another study reported acupuncture and cupping less beneficial than acupuncture and hot herbal compresses for hamstring muscle strains. 34 Cupping was further found to be superior to no intervention in soccer players for perceived injury-induced disability due to lower back pain, 40 and similarly, studies found a significantly larger range of motion outcomes following cupping 36,37,40 when compared to no intervention controls. 37,40 However, when the above studies were compared to other objective interventions, particularly involving movement, that is, stretching, no differences in outcome measures were evident. 36 Cupping was also superior in those trials in terms of lumbar isometric endurance 40 or torque at shoulder rotation 37 when compared to no intervention. Finally, perceived exertion after training was investigated in two trials, 28 –30,32 with significant lower training-induced exertion following cupping compared to no intervention controls. 28 –30,32
From a clinical perspective, studies measuring creatine kinase after training reported reduced values 16 h after cupping 28 –30,35 compared to no intervention. Of interest, cupping alone was found to increase creatine kinase concentrations comparably to moderate-intensity exercise itself. 39 However, a predominance of other studies found no differences regarding other markers of stress or inflammation as based on blood urea or nitrogen concentrations or other “routine urine parameters.” 28 –30
One study that investigated swimmers with sunstrokes found that acupuncture and cupping were superior to herbal medicine for light to severe sunstroke, when viewed from the perspective of recovery rate within 24 h and time to recovery based on physical symptoms. 33
No study assessed safety, that is, no study measured or reported adverse events or side-effects. As for risk of bias assessment, none of the trials reported adequate random sequence generation or allocation concealment. No study reported blinding of participants or personnel, and only one study 38 reported blinding of outcome assessor. This study, however, included self-report data as well, and thus, blinding for self-report outcomes could not be considered low risk in any study. Attrition rates were only reported by three studies that reported a small number of dropouts only 36,37,40 ; all other studies had to be judged as unclear. Insufficient reporting, potential lack of ethical approval, and potential conflict of interest resulted in high risk of bias in all RCTs. Full results of the risk of bias assessment can be seen in Figure 2.
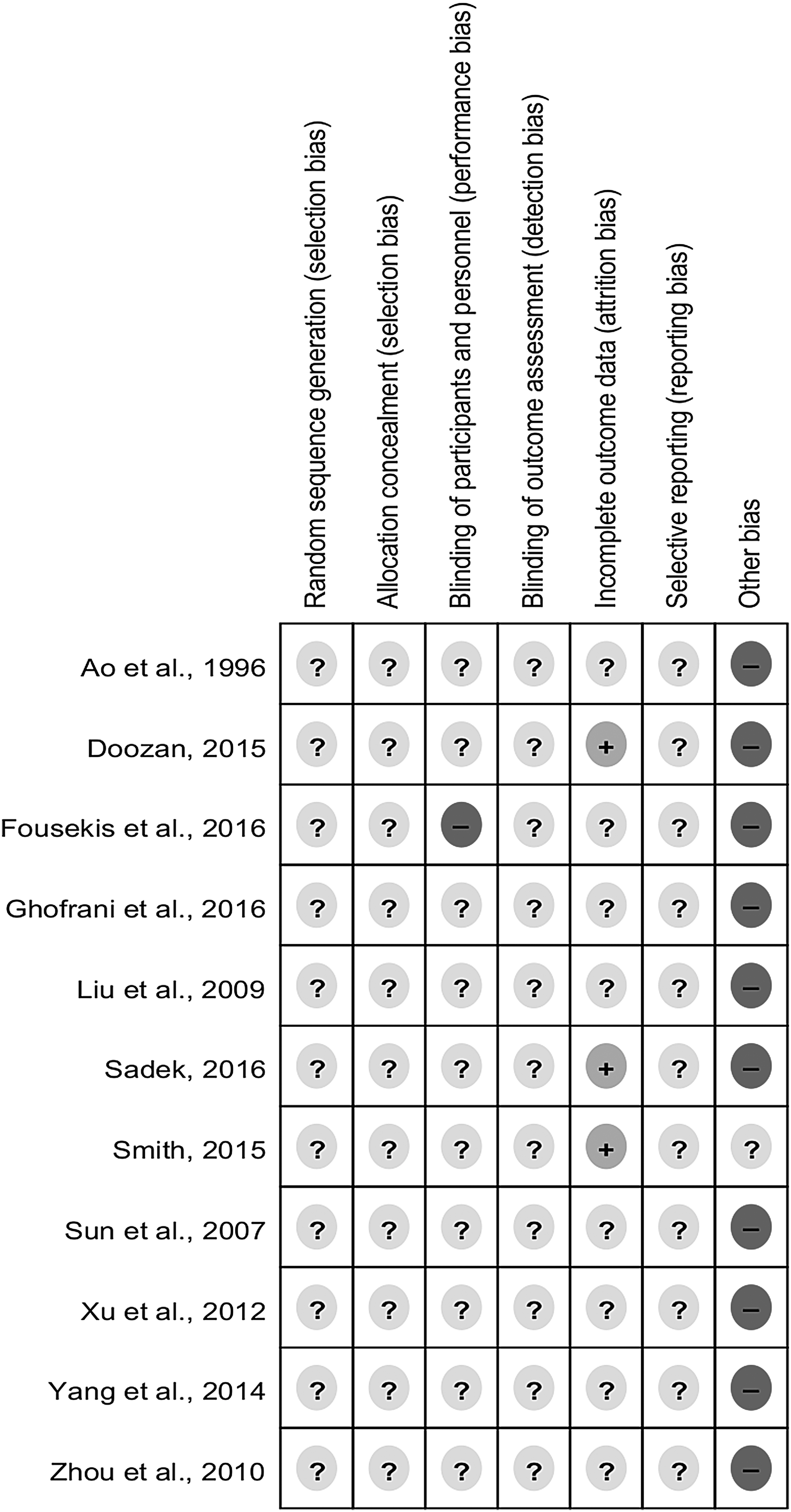
Risk of bias of included trials. “+” indicates low risk of bias, “−” indicates high risk of bias, and “?” indicates unclear risk of bias.
Discussion
This is the first systematic review to provide a comprehensive overview of randomized controlled trials to examine benefits and risks of cupping in athletes and sports people, and identify gaps in the scientific evaluation of cupping in the past. Given the lack of published empirical research, only a limited number of studies could be included. Of those included studies, several did not examine the effects of cupping exclusively, but rather the effects of cupping combined with other interventions such as acupuncture or moxibustion. While many studies reported benefits of cupping for most outcomes, including pain and symptoms, range of motion, and physiologic markers of systemic damage or stress, in most cases these studies had no control group intervention. Accordingly, the risk of bias assessment revealed insufficient reporting for all domains, and as such, potential study biases cannot be ruled out. Regardless, given the growing popularity of cupping for athletes, as yet no systematic review exists to date and the results of this review cannot be compared with previous reviews. Results of this review, however, can be compared with other scientific work in relation to cupping therapy.
With regard to pain, this review found benefits of cupping for lower back and hip pain in soccer players, and heel pain in a variety of athletes, when compared to no intervention. Previous research has found benefits of cupping for musculoskeletal pain conditions, including lower back and neck pain, 10 –12,14,15,41 and osteoarthritis. 42 Those reviews, however, did not include athletic populations; as such, results are hardly comparable. With several methodological limitations evident, nonspecific effects can further not be ruled out as being an artifact of the research design. In fact, a recent trial found that cupping displayed similar effectiveness to a sham/or minimal cupping in patients with fibromyalgia. 43 Given the cultural status of cupping in China as part of the Traditional Chinese Medicine system, 4,5 and in Arabic societies as part of the Medicine of the Prophet, 8 patients in those countries are likely to have very high expectation in the effectiveness of cupping. Prior research has demonstrated that patient expectations correlate to both within-group changes and between-group disparities, 44 as such, it cannot be ruled out that benefits of cupping regarding pain may be unspecific in nature.
Trials reported in this systematic review also found that range of motion improved after cupping. 36,37,40 Such a finding has been demonstrated before, through which cupping increased straight leg raise and also lumbar flexion range of movement. 16 At the current time, the relationship between cupping and range of motion remains unclear, and the increased range of motion might be related to a cupping-induced muscle relaxation or myofascial release. 36 Given that the effects have only been found in trials comparing cupping to a nontreated control, and that no blinding was used in the majority of trials, unspecific effects must be considered as potential causal contributors to the effect. Since it is still unclear whether an improved range of motion might benefit athletic performance, 45 further studies are warranted for more conclusive outcomes.
Cupping was also found to improve pressure pain sensitivity in one study, 38 and similar results have been found in previous studies using cupping for alleviation of symptoms of chronic neck pain. 10,11 It was assumed that cupping might improve local microcirculation and as such improve muscle function at the affected areas, resulting in a reduction of hypersensitive trigger points. 10 However, the relationship between pain and pressure pain sensitivity is quite complex, and at least for chronic neck pain no such associations have been found when multiple trials on cupping were collated and reanalyzed. 46
Several studies have also included laboratory measures to examine the benefits of cupping on indirect markers of muscle damage, such as creatine kinase. 28 –30,35,39 Two studies found decreased creatine kinase concentrations 16 h post-treatment when compared to no treatment controls. 28 –30,35 In athletes, creatine kinase is used to assess training-induced muscle damage, and thus infers the potential state of recovery and readiness to train. 47 –49 Consequently, decreased creatine kinase values following therapeutic interventions are assumed to represent improved muscle regeneration and ensuing readiness to perform. To date, further placebo-controlled studies are warranted to better understand the relationship between cupping and creatine kinase in athletes. Together with other studies, 18 those findings might provide insights into the mechanisms of cupping therapy. This aforementioned study 18 examined the effects of cupping on cellular pyruvate, lactate, glucose, glycerine, and adenosine 18 and found that the lactate concentration after cupping increased significantly, being indicative of cupping-induced hypoxia in the subcutaneous tissue. Moderate acute local metabolic acidosis has been shown to result in local vasodilatation and improved microcirculation, 20 –22 and as such, the authors speculate that cupping might improve microcirculation in the long run. 18 Given the potential biased results in the studies of this review, more studies are warranted to determine, for example, metabolic changes due to cupping therapy to improve understanding of its potential mode of action. Investigators should, however, be cautious to select valid and reliable outcome measures for their respective research questions.
One major drawback of this review is the lack of sufficient reporting of information pertaining to participants' safety, as none of the trials assessed or reported adverse events or side-effects. This seems to be a common finding for complementary medicine trials such as acupuncture, 50 yoga, 51 or manual therapies. 52 Given that cupping may be associated with a number of severe side-effects as reported in case reports, 53 –58 especially when used by practitioners with lack of formal qualification, future trials need to assess and report safety sufficiently.
An important consideration of the results reported above is the overall risk of bias in included studies was unclear or high, and this is not uncommon for trials in Traditional Chinese Medicine. 59 However, even those trials conducted in Europe 38 or the United States 36,37 lacked standard reporting items such as randomization and allocation concealment as observed in this review. Authors of prospective research are urged to improve the reporting of trials on cupping therapy and adhere to standard reporting guidelines such as CONSORT. 26 Further RCTs must ensure rigorous methodology and apply adequate methods of randomization, allocation concealment, intention-to-treat analysis, and blinding of at least outcome assessors to provide valid data for conclusive judgment of the effects of cupping therapy in athletes. While the use of placebo controls to examine specific effects is considered gold standard in conventional research, it has been controversially discussed in complementary medicine. 60 As such, future studies should also examine the effectiveness of an intervention in its usual clinical environment.
Overall, while the trials reported in this systematic review found beneficial effects of cupping in athletes when compared to no intervention, there are several limitations in the reporting of these outcomes that preclude definitive statements on the efficacy. For example, the most important limitation is related to the paucity of studies available with several of available studies published in journals with no or unclear peer review as well. Although the search was not limited to trials published in English, it is questionable whether the inclusion of Chinese trials increased the validity of findings, mainly because trials originating in China have been shown to produce mainly positive findings. 61 The heterogeneity of trials regarding participants' characteristics, the cupping techniques, and the combination of cupping with other techniques such as acupuncture not only limits the validity of results but also renders a quantitative synthesis impossible. Trials did not include suitable placebo controls, or other adequate standard control groups, and as such, the specific effects of cupping could not be determined. Finally, the potentially limited validity of outcome measures applied in the trials, and the generally unclear risk of bias in the included studies, does not allow for conclusive judgment of the validity of results. Further investigation and studies are required to enhance the understanding and scientific evidence of the efficacy, safety, and mechanisms of cupping in athletes.
Conclusion
From this review, no recommendation for or against cupping can be made at the current time due to the paucity of data and methodological flaws of the included studies. Additional studies are necessary for conclusive judgment on the efficacy, safety, and mechanisms of cupping in athletes, to provide up-to-date evidence to athletes, sports associations, and healthcare practitioners.
Footnotes
Acknowledgment
The authors thank Dwan Vilcins for her feedback on the first draft of the article.
Author Disclosure Statement
No competing financial interests exist.