
Abstract
Objectives:
This study aims to describe the Australian complementary medicine (CM) workforce, including practice and professional characteristics.
Design:
National cross-sectional survey.
Settings/Location:
Australia.
Subjects:
Any individual who self-identified as a practitioner qualified in any one of 14 CM professions and working in any state or territory of Australia was eligible to participate in the survey.
Interventions:
A 19-item online survey was developed following a review of existing CM workforce data and in alignment with other CM workforce survey projects in progress at the time. The survey items were presented under three main constructs: demographic characteristics, professional characteristics, and practice characteristics.
Statistical analysis:
Descriptive statistical analysis, including frequencies and percentages, of multiple choice survey items was used. Open response items were analyzed to determine the mean, standard deviation (SD), minimum, and maximum. The demographic data were evaluated for representativeness based on previously reported CM workforce figures.
Results:
The survey was completed by 1306 CM practitioners and was found to be nationally representative compared with the most recent registrant data from the Chinese Medicine Board of Australia. Participants primarily practiced in the most populous Australian states and worked in at least one urban clinical location. Most participants held an Advanced Diploma qualification or lower, obtained their qualification ten more years ago, and practiced in a clinical environment alongside at least one other practitioner from another health profession. Participants reported diverse clinical practice specialties and occupational roles. Per week, participants worked an average of 3.7 days and treated 23.6 clients.
Conclusions:
The results from this survey of practitioners from most complementary professions in Australia provide new insights into the national complementary medicine workforce. Further exploration of the CM workforce is warranted to inform all who provide patient care and develop health policy for better patient and public health outcomes.
Introduction
C
Diversity in occupational roles in the contemporary health workforce
The health workforce is a large and diverse group of occupations primarily trained to work within clinical settings. The roles of these health providers can vary considerably, not only across occupational groups but also within disciplines. 11 This diversity may be driven by a number of forces, including practitioner-related issues (e.g., need for greater job satisfaction and opportunity for career advancement), patient-related issues (e.g., unmet community healthcare needs), and institutional context (e.g., neoliberal management philosophies; greater emphasis on patient-led rather than practitioner-driven health services). 11 –14
Occupational role diversity can present a number of challenges for educational institutions, professional associations, regulatory bodies, and policy makers. These challenges include the need to provide appropriate undergraduate and postgraduate training to adequately prepared practitioners for the various roles they may perform 15 and to ensure that health professionals are acting appropriately within their intended scope of practice. This training is also paramount in ensuring that health providers operate efficiently and effectively within the context of the broader health system. 16,17
These challenges are potentially amplified in CM due to the lack of coherent professional leadership and variability often occurring in training within and across disciplines. 18 Although some CM professions in Australia (i.e., traditional Chinese medicine, chiropractic, and osteopathy) are under statutory registration, 19 these are exceptions, and the majority of CM professions are not formally registered by government. The unregistered CM professions exist largely beyond the gaze of those organizing healthcare provision and policy, reinforcing the view that CM operates as the “black market of healthcare”. 20 In the case of unregistered CM professions, stakeholders have attempted to develop other mechanisms to compensate for the absence of statutory registration such as the National Code of Conduct for Healthcare Workers 21 and the Health Training Package developed by the federal and state governments, 22 as well as practice standards and complaint mechanisms enacted through professional associations 23,24 and independent registration bodies. 25,26
Despite the mixed regulatory status of CM professions in Australia, the popularity of CM has not waned; in fact, the grassroots movement toward an integrative model of healthcare has seen many health consumers choosing to consult a CM practitioner in conjunction with conventional healthcare providers. 27,28
The importance of workforce data to support policy and practice
Government agencies responsible for providing accessible, affordable, efficient, and safe healthcare to those in need rely upon accurate health workforce data to inform policy development. 29 Equally, peak professional bodies charged with supporting the advancement, professionalization, and sustainability of a health profession benefit from detailed workforce data to assist them in their efforts. 30 Some attempts have been made to characterize the Australian CM workforce by analyzing existing data on the general CM workforce 31 or by focusing on specific unregistered professions, such as Western herbalists, 32 –34 massage therapists, 35 and naturopaths. 32,34 This body of work has provided some insights into the demographic profile 31,32 and attitudes of CM practitioners, 35 as well as the practice characteristics of specific CM disciplines. 32,33,35
Analyses of registrant data for the few CM professions that are registered in Australia, while representative of these professions, have largely been limited by focusing only on practitioner demographics and practice location 36 with the chiropractic 37 and osteopathic 38 professions as the few exceptions. Only one of these studies captures a sample representative of the Australian population 31 and while more accurate workforce data for registered professions can be found in government reports, 30 there are still large areas of uncertainty regarding the details of the workforce for unregistered professions.
Although investigations into the CM workforce have improved their understanding of this population, there are still many aspects that are yet to be examined (i.e., practice location, occupational roles, practice hours, patient load, and so on) 39,40 ; the absence of such data limits the ability of policy makers to develop and implement responsive, appropriate, and evidence-informed policies that impact the entirety of the health system. 29,41
The study reported here draws from national CM workforce survey data to address some of the knowledge gaps surrounding the Australian CM workforce; in doing so, the study aims to present a more comprehensive profile of the CM workforce to better inform future health workforce and health service planning.
Materials and Methods
Design
National cross-sectional survey of Australian CM practitioners.
Aims and objectives
This study aims to describe the Australian CM workforce, including practice and professional characteristics.
Sample
Any individual who self-identified as a practitioner qualified in any one of 14 CM professions (Fig. 1) and working in any state or territory of Australia was eligible to participate in the survey. Participants were required to have access to the Internet as the survey was administered online. Chiropractors and osteopaths were excluded as other workforce surveys were known to be under development for both professions. 42,43 The sample was recruited as part of the initiation of the Practitioner Research and Collaboration Initiative (PRACI); more information about the sample methodology has been described in detail previously. 44 The minimum target sample size for statistical significance was determined to be 639 based on the most recent known number of CM practitioners (n = 16 136) 31 with a confidence level of 99% and a confidence interval of 5.
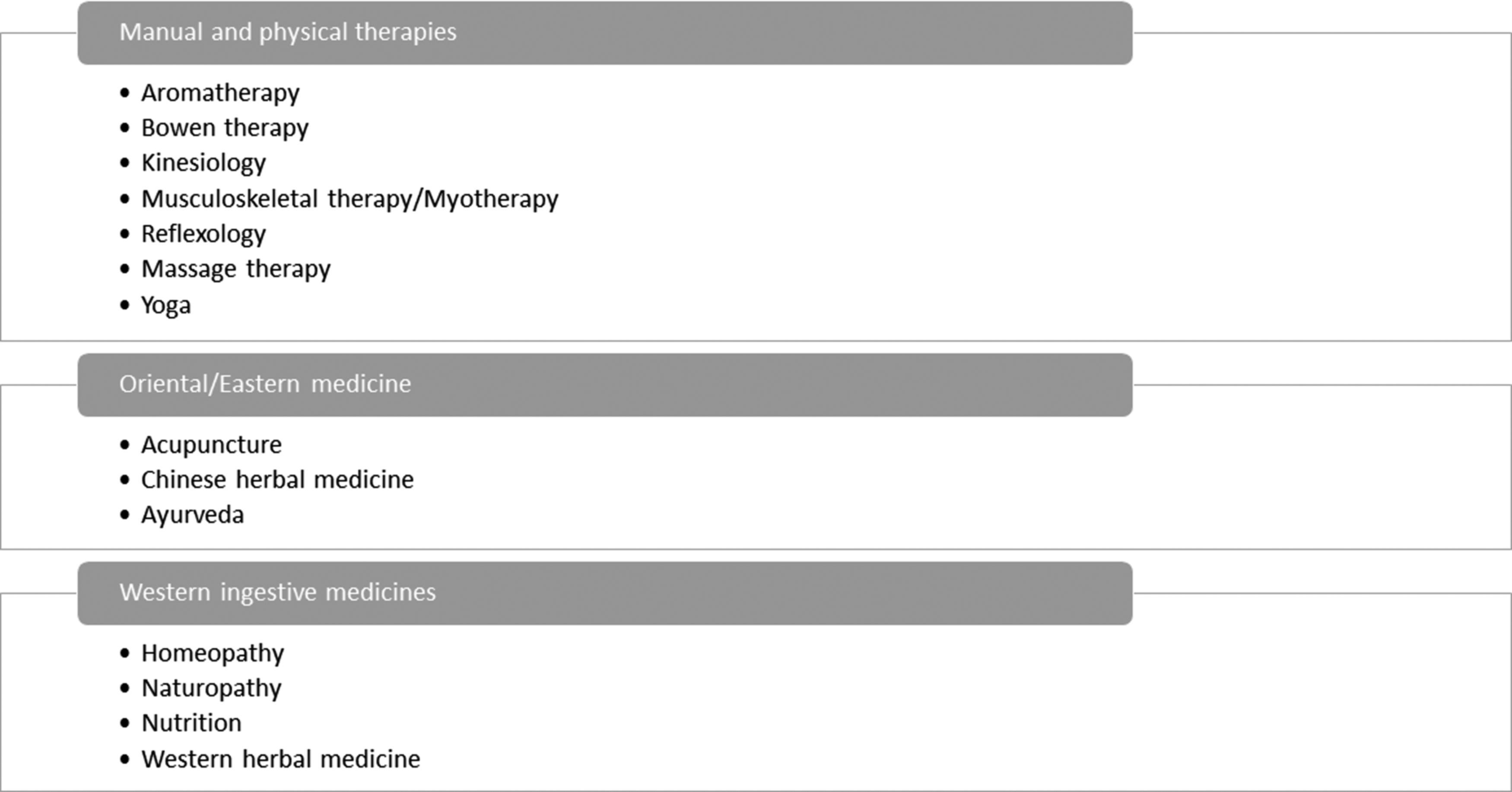
CM professions included in the target sample population for the PRACI Workforce Survey. CM, complementary medicine; PRACI, Practitioner Research and Collaboration Initiative.
Survey
The survey was drafted following a review of existing CM workforce data and in alignment with other CM workforce survey projects in progress at the time. 42 The draft survey was then piloted for face validity with six CM practitioners known to the research team from different professions and practice environments to ensure relevance to the diverse professional categories represented in the target sample. The survey comprised 19 items, which were presented under three main constructs as follows: demographic characteristics (e.g., age, gender), professional characteristics (e.g., CM qualifications, years since first qualification, association membership, and occupational roles), and practice characteristics (e.g., number of clients seen per week, practice location, number of clinics, other practitioners in primary clinical location, average rate charged per hour, and clinical specialties [i.e. areas of special clinical interest or focus]). The survey items were primarily closed questions with multiple choice response options. Open questions were used for some questions targeting practice characteristics where the answer was expected to be a numeric value (e.g., average days worked per week, average clients seen per month, and years in practice). The estimated completion time of the survey was 15 min.
Data collection
Eligible CM practitioners were identified using membership lists of professional CM associations (i.e., Australian Naturopathic Practitioners Association [ANPA], Naturopaths and Herbalists Association of Australia [NHAA], Massage and Myotherapy Australia [MMA], Australian Integrative Medicine Association [AIMA], Complementary Medicines Australia [CMA], Complementary Medicine Association [CMA], Australian Acupuncture and Chinese Medicine Association [AACMA], Australasian Association of Ayurveda [AAA], Australian Homoeopathic Association [AHA], Yoga Australia [YA], Reflexology Association of Australia [RAA], Association of Massage Therapists [AMT]) and customer lists of companies with CM practitioners as the customer base (i.e., Health World Ltd, Bioconcepts Ltd, FIT-BioCeuticals Ltd, Naturopathic Product Online Database, and Natural Therapy Pages). Two large professional associations did not choose to disseminate the survey invitation (Australian Natural Therapists Association [ANTA] and Australian Traditional Medicine Society [ATMS]). However, through the client distribution lists of organizations such as the web-based service advertising site Natural Therapy Pages, as well as practitioner-based supplement companies, the authors are confident that the invitation had a broad reach. Each organization was supplied with recruitment material and requested to communicate information about the study to CM practitioners on their database using whichever communication channel deemed appropriate to each organization's management team. CM practitioners were also informed of the study using social media (e.g., Facebook, Twitter) and through practitioner meetings such as professional conferences. All recruitment materials provided initial information about the project and a link to the survey. Upon accessing the survey link prospective participants were presented with the participant information sheet, which included an informed consent agreement and information about ethical clearance. The survey was administered online using the SurveyGizmo platform.
Statistical analysis
Data were exported from the SurveyGizmo platform into Stata 14® software for statistical analysis. Binary variables were created for items such as practice location and locality, professional qualifications, highest level of qualification held, and practice special interests, to account for practitioners with multiple qualifications, practices, and/or special interests. Descriptive analyses for all respondents, including frequencies and percentages, were calculated for variables of interest. Comparisons across professions were not possible, due to participants having qualifications across more than one profession. Chi-square analyses were used to evaluate the representativeness of the sample against demographic data for the Australian CM profession as published by Leach. 31 An additional analysis comparing respondents from the Traditional Chinese medicine (TCM) professions (i.e., acupuncturists and Chinese herbalists) with national registration data 30 was also undertaken, due to the limitations of Leach's CM workforce data. 31
Results
Demographic characteristics
The survey was completed by 1306 CM practitioners, the majority of whom were female (n = 1004; 76.9%) and aged between 40–59 years (n = 775; 59.4%). These figures were higher than those previously reported for the Australian CM workforce (p < 0.001), but for TCM practitioners, were not significantly different to 2015 Chinese Medicine Board of Australia registrant data (Table 1).
As reported from the 2006 Australian population census by Leach. 31
As reported in the December 2015 CMBA report.
CM, complementary medicine.
Practice characteristics
The practice characteristics of respondents are presented in Table 2. Practitioners primarily practiced in the more populous Australian States of Victoria (n = 454; 34.8%), Queensland (n = 317; 24.3%), and New South Wales (n = 268; 20.5%) and notably less practiced in the smaller states and territories. A small percentage of respondents also identified as having a “virtual” clinical practice. While the majority of practitioners worked in a single clinical location (n = 848; 64.9%), more than one-third had two or more clinical practices. These clinics were predominantly located in an urban location (n = 1067; 81.7%), although at least one in four practitioners (n = 325; 28.5%) had a clinic in a rural setting. Most respondents (n = 1291; 98.8%) held at least one membership with a CM professional association.
There was wide variation in the number of years since participants had received their first CM-specific qualification, with most (n = 868; 66.5%) obtaining their qualification ten or more years ago (Table 2). There was also diversity in the composition of clinical teams, with 23.5% (n = 304) working only in solo practice, 26.6% (n = 345) working only in a shared clinical practice environment, and 49.9% (n = 646) working across shared and solo practice settings. Chiropractors (n = 109; 8.4%), counselors (n = 102; 7.8%), physiotherapists (n = 92; 7.0%), and osteopaths (n = 90, 6.9%) were the professions that CM practitioners were most likely to share a clinical space with. CM practitioners were least likely to share a clinical space with midwives (n = 14; 1.1%), social workers (n = 23; 1.7%), specialist doctors (n = 26; 2.0%), and community nurses (n = 31; 2.4%). Approximately 4.5% of respondents (n = 59) were colocated with a general practitioner.
CM practitioners reported twenty different clinical practice specialties (Table 2). The most frequently reported specialties were general health and well-being (n = 949; 72.7%), musculoskeletal conditions (n = 921; 70.5%), and pain management (n = 778; 59.6%). Practice specialties reported the least were pediatrics (n = 393; 30.1), renal health (n = 342; 26.2%), and gerontology (n = 252; 19.3%).
The outcomes of the analysis regarding clinical consultation economics are reported in Table 3. The respondents worked an average of 3.7 days per week as a CM practitioner, with naturopaths working the least number of days per week (mean: 3.2 days) and myotherapists working the greatest number of days per week (mean: 4.3 days). These differences did not directly translate to the number of client hours worked per week, with the lowest number of hours worked reported by reflexologists (mean: 13.9 h/week) and the highest number reported by Chinese herbalists (mean: 25.5 h); the average for all respondents was 17.8 h per week.
CM, complementary medicine.
The mean number of clients consulted per week was also greatest for Chinese herbalists (28.4 clients), but the lowest number was reported by Ayurvedic practitioners (9.7 clients). The average number of new clients seen per month for all CM professions was 23.6 clients. Chinese herbal medicine practitioners and acupuncturists reported a similar and equally high number of new clients per month (mean: 43.2 clients), compared to reflexologists who reported seeing the least (mean: 14.7 clients). The average rate charged per hour as a CM practitioner was $83.58, although this varied across professional categories, with homeopaths reporting the highest hourly rate (mean: $106.57) and reflexologists reporting the lowest hourly rate (mean: $71.78).
Professional characteristics
The majority of respondents identified as being in clinical practice as a CM practitioner (n = 1184; 90.7%) and spending on average 80% (SD 28.4) of their work time in this role (Table 4). Participants had worked a mean 5.9 (SD 7.8) years full time and 5.7 (SD 6.6) years part-time as a CM practitioner. In addition to CM clinical practice, 19.7% (n = 251) also worked in a non-CM clinical role for approximately 52.1% (SD 32.1) of their work time. A similar number of respondents reported other occupational roles such as lecturer (18.5%; n = 156), group educator (9.4%, n = 123), and retail employee (9.3%, n = 71). For those with a nonclinical occupational role, the average percentage of time committed to this role ranged between 19.4% (group educator, SD 21.6) and 42.0% (retail employee, SD 26.8).
CM, complementary medicine.
In terms of practitioner qualifications, the majority of participants across most professions held an Advanced Diploma qualification or lower, with the only exceptions being acupuncture and Chinese herbal medicine (Table 5). Most acupuncturists held a Bachelor degree qualification (n = 112; 64.7%), with almost one in four (n = 32; 18.5%) possessing a postgraduate qualification. More than half (n = 45; 52.9%) of Chinese herbalists had a Bachelor degree qualification, with almost one-third (n = 24; 28.2%) holding a postgraduate qualification. Although two-thirds (n = 193; 66.8%) of naturopaths had an Advanced Diploma qualification or less, there was still a sizeable proportion that held a Bachelor degree qualification (n = 123; 42.6%); however, very few (n = 7; 2.4%) had a postgraduate qualification. By contrast, while a similar proportion of clinical nutritionists also held an Advanced Diploma qualification or less (n = 113; 68.1%), a relatively greater proportion of this group had a postgraduate qualification (n = 18; 10.8%). Of all professions, aromatherapists (98.2%) and reflexologists (97.5%) had the largest proportion of respondents with an Advanced Diploma qualification or lower.
Discussion
This study highlights the diversity of the CM workforce in Australia and offers an update to existing workforce data, as well as offering new insights into the nonclinical roles undertaken by CM practitioners. The study makes a number of important observations; first, although most Australian CM practitioners work as clinicians, a sizeable proportion of this workforce is also engaging in other nonclinical roles. While previous research has identified diversity in the types of treatments and therapies used in the CM clinical setting, 32 this research underlines the variety of settings and roles outside of clinic that comprises a CM practitioner's occupational life. Whether this mixture of roles is influenced by transitions in the CM practitioner's career 11 (i.e., transitioning from study to practice; establishing a new practice; and responding to patient-led demand for health services or unmet community health need) 11 –13 is not yet clear.
Some CM practitioners report working as retail employees, most likely in pharmacy or health food store settings. 45 This occupational role may be driven by consumer demand as previous research indicates that 58% of pharmacy customers endorse the employment of a CM practitioner in pharmacies that stock CMs. 46 Public safety concerns also have been raised by researchers, as untrained health food store assistants have been found to provide unsafe healthcare advice to customers. 47 Alternatively, or perhaps in addition to the possible market demand for CM-qualified retail staff, practitioners may be choosing to integrate retail duties into their occupation to address insufficiencies in their income from clinical practice. 32 While there is emerging evidence regarding the nature of health advice provided to customers of health food stores 48 and pharmacies, 49 there has been little exploration of the role and contribution of qualified CM practitioners within those retail environments, pointing to a need for additional research in this area.
The number of CM practitioners working as group educators lends weight to the argument that some CM professions practice in accordance with, or are philosophically aligned with, the principles of public health and health promotion. 50,51 While existing research suggests that CM practitioners emphasize patient education within the clinical consultation 9,10 and may focus on wellness and disease prevention, 52 this is the first known study to reveal that these professions also provide group education to the community. However, the content of these CM-practitioner led group education sessions is not yet known and warrants closer examination before the role of CM practitioners as providers of community health promotion and public health services can be assumed. Overall, this study offers new insights into the roles that CM practitioners play within the health system, but urges caution in reaching any firm conclusions until a more comprehensive exploration of these roles has been undertaken.
The findings of this study also suggest that Australian CM practitioners have diverse practice specialties. While the most common practice specialty reported by respondents in this study was “general health and well-being”, other more specific disease-oriented interest areas were also common. The relationship between CM and wellness is well established both at a theoretical and philosophical level, 53 as well as in the real world; 54 it is also a key reason why individuals report using CM. However, although CM is known to be used for specific conditions such as cancer, 7,55 depression, 6 and arthritis, 4 the specific role and contribution of CM practitioners in the management of these and other health conditions are largely unknown. 39,40 In fact, the degree to which CM practitioners value-add clinical care has received sporadic interest from researchers at best. 52,56 This study therefore provides a useful direction for future researchers seeking to explore this topic more carefully.
Another observation of this study is the considerable variation in the level of training of Australian CM practitioners. This variation most likely reflects the availability of university training for CM in Australia. 57 Notwithstanding, it is unlikely that access to professional education is the only contributing factor, as almost half of naturopaths reported having an Advanced Diploma qualification or less, despite a Bachelor degree qualification for naturopathy being available in Australia for over 20 years. 18 Statutory regulation also may have an influential effect on the level of practitioner training within specific disciplines, with the two statutory regulated professions in this study (i.e., Acupuncture and Chinese herbal medicine) both reporting the highest proportion of Bachelor degree or postgraduate qualified practitioners. 36,58
Many of the metrics associated with economic viability of CM clinical practice (i.e., days worked per week, number of clients seen per week, and number of new clients per month) were above average for most CM professions in this study that are characterized by “practitioner-administered” treatments such as acupuncture and massage therapy. 16 Many of the CM professions that deliver “practitioner-administered treatments” may also be benefiting from high rates of referral from other health professionals. 59 By contrast, the professions that primarily provided patient-administered treatments, 10 such as naturopathy and homeopathy, charged above average hourly rates. Given that the factors driving the economics of health service delivery are reasonably complex, the reasons for these differences are not entirely clear. It may be that those CM professions in this study with a higher average hourly rate are driven by a need to maintain practice viability in response to decreasing patient numbers. 60 It is also possible that practitioners in professions characterized by prescription of patient-administered treatments may be responding to increased market demand due to the relative size of their workforce. 61
Contrary to reports from previous studies that Australian CM practitioners work alone and are isolated from healthcare teams, 32 the findings of this study indicate that three out of every four Australian CM practitioners provide consultations in a shared clinical environment of some kind. This difference may be due to the evolving professionalization and mainstreaming of CM in the years since this previous research was conducted. However, this pattern of shared clinical location was less likely to be inclusive of medical doctors such as GPs or specialist doctors, suggesting that CM practitioners are still practicing at structural and geographical distances from the core of mainstream healthcare delivery in Australia. Furthermore, it is not clear whether this finding reflects interprofessional collaboration or just co-location. There are diverse models of care reported in the literature within the broad scope of integrative or CM, 27 with several studies exploring the interprofessional communication between CM practitioners and other health professions reporting varying success. 32,62,63 And as such suggest that, along with the level of isolation of CM within the broader health system, the practice environments for CM practitioners may be adapting to the changing role of CM in contemporary healthcare. It is interesting to note that the health professionals most commonly sharing a clinical space with CM practitioners in this study provided either manual therapies or psychologic support. As a possible explanation of this trend, the importance of mind–body medicine is acknowledged within CM as a core component of holistic philosophy 8 and may compel CM practitioners to provide patient referrals to health professionals that are able to provide more advanced and specialized support for their patients' emotional and physical health complaints. Closer researcher attention to the structural, spatial, and interpersonal interface between CM and other health professionals is needed before any of these possible interpretations can be verified.
Limitations
While contributing to their understanding of the Australian CM workforce, there are limitations to this study that require consideration. First, the representativeness of the data is not clear. Based on comparisons with Australian Census data, 31 their sample appeared to be older and more female dominant than the national average; however, it is possible that the exclusion of chiropractors and osteopaths in their sample (both male-dominant professions) 31 and the age of the census data (i.e., more than 10 years old) may have contributed to the differences between data sets. According to more recent data (i.e., CMBA registrant data), 58 our sample of TCM practitioners does appear to be nationally representative. As such, while our analysis does suggest that our sample may be nationally representative, no firm conclusions on this issue can be drawn. Our study is also limited by factors inherent in the study design, such as the risk of response bias, as all answers were self-reported.
Conclusions
CM use, including consultations with CM practitioners, is widespread, and the CM workforce provides substantial levels of clinical care in many important areas of health. The characteristics of CM practice are diverse and reflect clear differences in practice dynamics and economics between the various CM professions. CM practitioners are also fulfilling a more diverse range of occupational roles than has been previously considered. The implications of this apparent diversity in CM practice within and across CM professions warrant further exploration to help inform all stakeholders involved in providing patient care and developing health policy for better patient and public health outcomes.
Footnotes
Acknowledgments
The PRACI project is funded by Endeavour College of Natural Health and supported by Key Support Partners, including Massage and Myotherapy Australia, Complementary Medicines Australia, Australian Homoeopathic Association, Health World Ltd, and FIT-BioCeuticals Ltd.
Author Disclosure Statement
The authors have no conflicts of interest to disclose.