
Abstract
Objectives:
Thai yoga is a traditional Thai exercise used for improving health-related physical fitness. Many studies have evaluated these effects, but their results remain inconclusive. This meta-analysis aimed to examine the effectiveness of Thai yoga on physical fitness.
Design/Methods:
PubMed, EMBASE, CINAHL, Cochrane library, Thai Library Integrated System (ThaiLis), Physiotherapy Evidence Database (PEDro), National Rehabilitation Information Center (Rehabdata), Scopus, Web of Science, Thai University library databases/journals, and Thai Physical Therapy database up to March 2016 were searched for randomized controlled trials (RCTs) examining the effect of Thai yoga exercise compared with normal daily activities as controls, in any language. The weighted mean difference (WMD) and 95% confidence intervals (95% CI) were performed using the random-effects model.
Results:
Seven RCTs met the inclusion criteria. Thai yoga training significantly improved body flexibility by 3.9 cm after 4 weeks [95% CI = 3.9–4.0; p < 0.001: no heterogeneity χ2 = 0.66, d.f.2, p = 0.7; I2 0.00%] and 8.9 cm after 8 weeks [95% CI = 7.4–10.5; p < 0.001: no heterogeneity χ2 = 0.16, d.f.2, p = 0.9; I2 0.00%] compared to controls. It also significantly increased range of motion (ROM) of right shoulder extension by 1.5 degrees at week 8, compared to controls [95% CI = 0.12–2.81; p = 0.03; low heterogeneity χ2 = 1.61, d.f.1, p = 0.2; I2 37.9%]. Greater ROM for right shoulder abduction was observed after 12 weeks compared to controls [22.2 degrees (95% CI = 20–24; p < 0.001): no heterogeneity χ2 = 0.29, d.f.1, p = 0.6; I2 0.00%].
Conclusions:
Thai yoga exercises appeared useful, in particular, on body and right shoulder joint flexibility. Regular stretching exercise of Thai yoga and/or in combination with exercises could promote health-related physical fitness.
Introduction
T
Thai yoga, the so called Rusie Dutton, Thai Rishi's self-exercise, and Ascetic Yogi's or hermit's self-stretching are technical terms for mind–body exercise with therapeutic stretching exercise in traditional Thai medicine. 5,6 This exercise includes gentle dynamic stretching of body parts, deep breathing exercises, meditation, and self-acupressure during these movements. 6 Thai yoga has its root in Indian yoga. It is similar to or nearly identical to the Indian yoga system such as Hatha Yoga. 6 In the late 1700s, around 127 different Thai yoga poses and therapeutic exercises were written on stone tablets. 5,7 Therapeutic benefits of Thai yoga were mentioned, including relief of musculoskeletal pain, chest congestion, visceral discomfort, generalized muscle weakness, and joint stiffness. 6,8 Recent clinical research showed the benefits of Thai yoga practice such as improving extensibility of soft tissue, spine and joint flexibility, balance performance, 9 increasing respiration, and anaerobic exercise performance. 10,11
Principles of health related physical fitness include: flexibility, cardiovascular endurance, muscular strength/endurance, and body composition. 12,13 Much scientific evidence has accumulated about the actions of Thai yoga on physical fitness, but it remains inconclusive. The purpose of this study was to examine the effectiveness of Thai yoga on physical fitness using a meta-analysis.
Materials and Methods
Literature search strategy
This systematic review and meta-analysis defined PICOS as follows: healthy volunteers as participants; Thai yoga or Rusie Dutton as the intervention group; normal daily activities as the comparator group; physical fitness, including (1) flexibility, (2) cardiorespiratory fitness, (3) muscular strength/endurance, and (4) body composition, were used as outcomes; and randomized controlled trials (RCTs) as the study design.
The following bibliographic databases were searched since their inception dates till March 2016: PubMed, EMBASE, CINAHL, Cochrane library, Thai Library Integrated System (ThaiLis), Physiotherapy Evidence Database (PEDro), National Rehabilitation Information Center (Rehabdata), Scopus, Web of Science, Thai University library databases/journals (e.g., Chulalongkorn University, Mahidol University, Naresuan University), and the Thai Physical Therapy database. The search strategy was combined with key words specific to the topic: Rusiedutton, Rusiedutton, Ruesidadton, Rueseedudton, Rueseedudton, Ruesidudton, Ruesidudton, Thai Richi's self-massage, Hermit's body twist, Thai yoga, Ascetic exercise, Thai stretching, and the Thai key word of Rusie Dutton. The reference sections of the retrieved original research publications were searched to identify additional publications and/or authors were contacted for unpublished articles or relevant information.
RCTs which met the following inclusion criteria were included in this systematic review and meta-analysis: (1) RCTs investigating Thai yoga compared with control group (normal daily activities), (2) RCTs reporting sufficient information about physical fitness outcomes classified as (i) flexibility, (ii) cardiorespiratory fitness, (iii) muscular strength/endurance, and (iv) body composition, and (3) no language restrictions.
Data extraction and assessment of methodological quality
Data were extracted from each trial by independent reviewers using a standardized extraction form. The extracted data included study design, population, characteristics of subjects (i.e., gender, age, and number of participants), type of intervention (i.e., number of poses, protocol of training, and duration of training per week), comparator, and outcomes. Outcomes of physical fitness were represented as mean and standard deviation (±SD).
The methodological quality of each trial was assessed using 2 assessment tools: the PEDro scale 14,15 and Cochrane's risk of bias assessment. 16 The PEDro scale was developed by the PEDro, which is based on the Delphi list and is a commonly used quality assessment tool offering a comprehensive measure of methodological quality in physical therapy trials. 14 In brief, there are 11 items for quality assessment with a maximum score of 10. The quality of each study can be classified as a score of 9–10 (excellent quality design), 6–8 (good quality design), 4–5 (fair quality design), or 0–3 (poor quality design). Risk of bias as recommended in Cochrane handbook for RCTs was assessed using the seven-domain Cochrane Collaboration's tool which scores as “Yes,” “No,” or “Unclear” and then classified trials as a low risk of bias, high risk, or unclear risk (indicating lack of information or uncertainty over the potential for bias).
Data analysis
For each outcome of physical fitness, the weighted mean difference (WMD) between Thai yoga training and control groups and 95% confidence intervals (95% CI) after 4, 6, 8, and 12 weeks of training, that is, intergroup (between-group) comparisons, were performed using the random-effects model of the DerSimonian–Laird method. 17
A statistical heterogeneity was tested using the Cochran–Mantel–Haenszel method. 18 p < 0.05 was considered as evidence of heterogeneity. I2 - statistics was also performed to determine the degree of heterogeneity across studies. An I2 of 25%, 50%, and 75% indicates low, medium, and high heterogeneity, respectively. 16,18 Statistical analysis was performed using STATA software, version 14 SE. 19
Results
Search results
The initial search yielded 20,999 articles. After screening, 20,971 articles were excluded due to their not meeting eligibility criteria; and 6 articles were duplicate studies. Twenty-two studies were relevant to physical fitness. However, 15 studies were later excluded after detailed evaluation: pilot study (n = 1); not RCTs [observational (n = 1); quasi-experimental (n = 2); nonrandomized (n = 2); no control group (n = 3); and not original research (n = 5)] (Fig. 1). In total, seven studies that met the inclusion criteria were included.

A flowchart of the included studies. RCTs, randomized controlled trials.
Study and participant characteristics
The meta-analysis included 185 participants in the 7 studies
10,20
–25
(Table 1), and all seven were nonblinded RCTs and comprised female participants except one that had both sexes,
23
ages were 16–83 years, and had cohorts of 20–40 participants. Number of Thai yoga poses ranged from 15 to 30, training periods were 4–12 weeks, and exercised for 90–180 min/week. Poses of Thai Yoga used in individual study are shown in Supplementary data are available online at
Same population.
NA, not applicable.
Quality assessment of the included studies
Based on the PEDro scale, one study was of good quality, and six studies were fair (Table 2). Based on Cochrane's risk of bias, all studies had adequate generation of the allocation sequence but most studies (n = 5) 10,20,23 –25 clearly did not conceal the allocation from researchers but did not report in other studies. Participants knew to which group they were allocated but what they were told about outcomes was not reported; all studies had high risk of performance bias. The researchers made their own measurements, so all studies had high risks of detection bias regardless of outcomes being objective or subjective. Four studies 20,21,23 –25 provided complete outcome data, while others had unclear risk of bias. The majority of studies (n = 6) 10,20,21,23 –25 were clear from reporting bias (Table 2).
Same population.
Y, yes; N, no; L, low; H, high; U, unclear; PED
Effect of Thai yoga on physical fitness
A total of 93 participants were assigned to Thai yoga training, while 92 participants in the control groups (normal daily activities). The meta-analyses of all outcomes are shown in Table 3.
Heterogeneity test at week 4.
Heterogeneity test at week 8.
Heterogeneity test at week 12.
NA, not applicable; ROM, range of motion; MIP, maximum inspiratory pressure; MEP, maximum expiratory pressure.
Effect of Thai yoga on flexibility
Five studies reported the effect of Thai yoga on body flexibility using the sit and reach test. Three studies 20,21,25 reported effects at week 4. The WMD of body flexibility increased by 3.94 cm. (95% CI, 3.89–4.00) over control (p < 0.001) with no heterogeneity across studies (χ20.66, d.f.2, p = 0.718; I2 0.00%) (Fig. 2). At 8 weeks of training in four studies, 20,21,24,25 WMD of body flexibility was 7.29 cm (95% CI, 4.27–10.31) but with high heterogeneity (χ212.63, d.f.3, p = 0.006; I2 76.2%) compared to controls (p < 0.001).
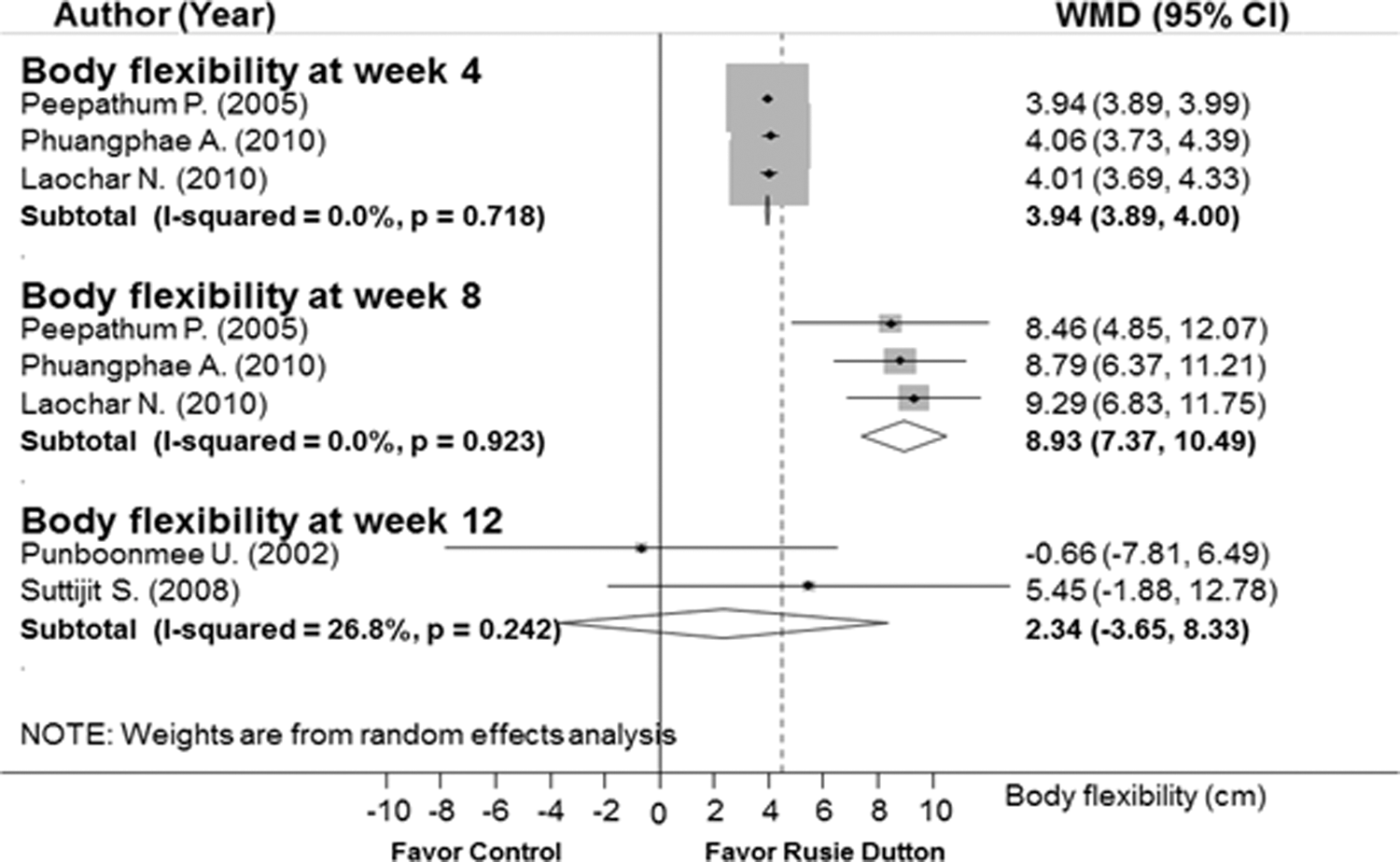
Effect of Thai yoga on body flexibility. WMD, weighted mean difference.
Subgroup analysis by age using only adults (17–83 year), 21,24,25 while excluding teenagers, increased body flexibility after 8 weeks of training; WMD was 8.93 cm (95% CI, 7.37–10.49; p < 0.001) without heterogeneity (χ2 0.16, d.f.2, p = 0.9; I2 0.00%) (Table 3, Fig. 2).
Three studies examined left and right shoulder flexibility each compared to controls using goniometers in three different directions (extension, flexion, and abduction) at 820,25 and 12 weeks training. 20,23 For flexibility of right shoulder extension at week 8, the pooled effect showed a significant increase of WMD range of motion (ROM) by 1.46 degrees (95% CI = 0.12–2.81; p = 0.033) with low heterogeneity (χ21.61, d.f.1, p = 0.2; I2 37.9%) as shown in Figure 3. Furthermore, ROM was higher for right shoulder abduction at week 12 of training than the control group [WMD = 22.2 degrees (95% CI = 20.24–24.19) without heterogeneity (χ20.29, d.f.1, p = 0.6; I2 0.00%)], see Figure 4. Likewise, shoulder flexibility in left extension, both left and right flexion, or left abduction at weeks 8 or 12 of training was likely to be better than the control group; however, these were based on high heterogeneity. The results of WMD ROM and heterogeneity tests are reported in Table 3.

Right shoulder extension at week 8 compared to controls. WMD, weighted mean difference.
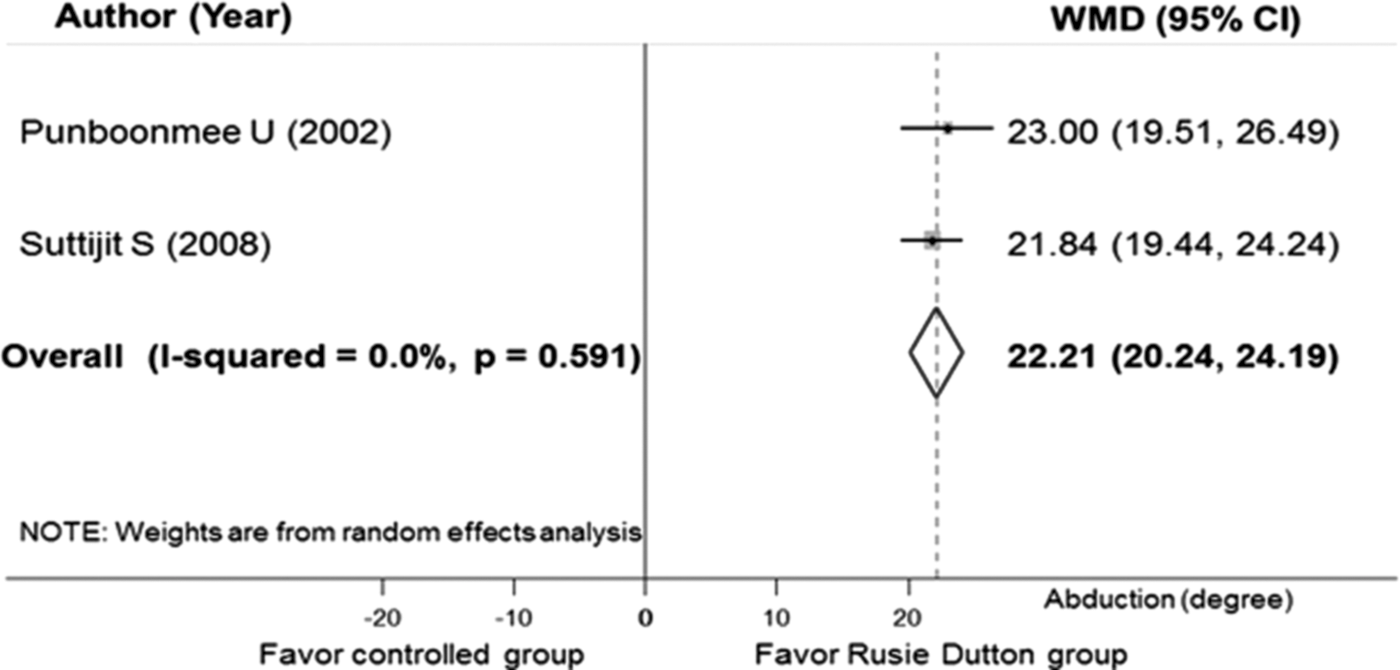
Right shoulder abduction at week 12 compared to controls. WMD, weighted mean difference.
Two studies 23,25 examined hip joint flexibility using goniometer. One study on elderly participants 23 showed a significant difference of active flexion and extension of hip joint flexibility (p < 0.05) at week 6 and 12 after training compared with the control group. Another study focused on working women aged 25–50 years 25 showed increases in ROM of active right and left of hip joint for both flexion (week 4, 8) and extension (week 8) compared to controls (p < 0.05).
One study 20 which published the comparative effects of training on ankle joint flexibility in 30 healthy female teenagers (aged 16–17 years) using a goniometer showed a significant increase of left ankle joint flexibility at week 12 compared to control group (p < 0.001).
Effect of Thai yoga on cardiorespiratory fitness
One study by Punboonmee 20 in healthy female teenagers found differences between trained and control groups in resting systolic and diastolic blood pressure and lung vital capacity at week 12 (p < 0.001) (Table 3).
Another study evaluated anaerobic fitness in young healthy sedentary females. 10 Peak anaerobic power (PP) and anaerobic capacity (AC), anaerobic indicators, were measured using Wingate method on a bicycling ergometer where the trained group at 4 weeks showed a higher PP and AC than in the control group (p < 0.001) (Table 3). The study 22 also examined training on respiratory muscle strength indicated by maximum inspiratory pressure (MIP) and maximum expiratory pressure (MEP). After 4 weeks training MIP and MEP were both increased compared to controls (p < 0.001) (Table 3).
Phuangphae (2010) 24 assessed cardiorespiratory fitness by the Astrand-Ryhming method using bicycle ergometers in healthy female students where training improved fitness after 8 weeks (p < 0.001) (Table 3).
Effect of Thai yoga on muscular strength/endurance
Phuangphae 24 also measured upper body and abdominal muscular strength and endurance by 30-sec abdominal sit-ups and 60-sec modified knee push-ups, and training showed significant increases at 4 and 8 weeks compared to controls (p < 0.001).
Laochar (2010) 25 investigated quadriceps muscle strength as leg extension using the Biodex™ Isokinetic system in sedentary working women. The trained group demonstrated significantly increased strength (by 21 ft-lb) at 8 weeks compared to controls (p < 0.001).
Effect of Thai yoga training on body composition
Phuangphae (2010) 24 used Lange skinfold calipers on skin overlying the biceps, triceps, subscapular, and suprailiac areas to estimate total body fat of their 30 healthy students. There was a significant decrease in fat after 4 and 8 weeks training compared with controls (p < 0.001).
Discussion
Thai yoga is an ancient Thai mind–body exercise dating back to more than 250 years, 5,6,26 which has incorporated slow stretching movement, control of breathing and meditation, and taught at the Chetawan Temple (Wat Pho) Thai Traditional Massage School in Bangkok, Thailand. This study is the first systematic review and meta-analysis to confirm the effect of Thai yoga exercise on improved physical fitness, in particular body and shoulder flexibility.
Thai yoga training increased body flexibility by 3.94 (week 4) and 8.93 cm (week 8) over and above normal daily activities. Indian Hatha yoga also increased body flexibility (by 4.1 cm at 8 weeks) in healthy younger adult volunteers (18–27 years) 27 and increased spine flexibility (by 5.6 cm at 12 weeks) in healthy older women (50–70 years old). 28 This suggests that Thai yoga exercises are at least as effective as Hatha Yoga. However, a head-to-head clinical trial comparing these methods on body flexibility could confirm this. In their study, participant age was identified as a factor influencing body flexibility. Based on exercise physiology, sit and reach test is usually used to assess flexibility of the lower back, hip, and upper thigh, and this method showed the unique pattern of age associations related, in part, to growth of the trunk and lower extremities during adolescence. 29 Adolescents during the growth spurt of long bones and poor hamstring length are less flexible than young adults. 30,31 Subgroup analysis of Thai yoga on body flexibility by age seems to reflect this finding. Sex, number of poses, or pose characteristics in the series of Thai yoga exercise may also attribute to differences in findings.
Thai yoga also improved shoulder flexibility in several directions. In particular, it increased the right shoulder ROM in extension (1.5 degree) and abduction (22 degrees) compared with the normal daily activities. These effects are similar to 8 weeks of yoga training. 27,32 Shoulder ROM is important in physical and daily activities. Joint motility components were quantified, and the joint capsule and ligament were cited as important factors for flexibility. 33 Dominant sidedness and posture could influence joint ROM. The dominant arm displayed a greater joint ROM than the nondominant side. 34,35 Most participants in their included studies were likely to be right handed reflecting the improved right shoulder ROM after Thai yoga training compared to the left shoulder. Although the improvement of shoulder flexibility appeared to be multidirectional, extension and abduction were clearly evident. This is probably because their included studies for meta-analysis were composed of Thai yoga poses in shoulder extension and abduction directions. Other factors affecting ROM may be sex, age, muscular strength, elasticity of the surrounding tissue, and pain. 34,35 Although shoulder flexibility in flexion showed increased flexibility, it was based on high heterogeneities. Clearer evidence is needed to prove an effect of Thai yoga on shoulder flexibility in flexion directions.
The mechanism of Thai yoga exercise on improved flexibility is not precisely known, but possibly related to stretching effect. Possible mechanisms for this may involve: increased muscle-tendon unit length by the long-term adaptation of connective tissue, sarcomere and/or reflex response; decreased evoked H-wave reflex latency as a neuromuscular sensitivity indicator; inhibited muscular antagonist mediated by the Golgi tendon organ-1b afferent axons; and reduced musculoskeletal stiffness. 1,29 Many studies have confirmed that stretching exercise helps to enhance physical fitness and performance by improving their range of movement, reduce passive stiffness, and reduce risks of exercise related injuries 1,36 and is recommended for athletes, older adults, and rehabilitating patients. Thai yoga, which is fundamentally a stretching exercise, could apply to any sporting activity especially during warm-up or for treatments of orthopedic conditions or injuries. 37
The effect of Thai yoga on other flexibility outcomes (hip flexibility, ankle flexibility, back flexibility) and on other physical fitness outcomes (cardiorespiratory fitness, muscular strength/endurance, body composition) remains inconclusive because of insufficient studies on these physical fitness outcomes. In addition, most included trials recruited only female participants, used normal daily lifestyle as control, and applied 15 different poses of Thai yoga. Further research should investigate the effect of Thai yoga on these remaining unanswered physical fitness outcomes, in male participants, compared with other stretching exercise or in people with physical health condition (e.g., musculoskeletal disorder).
Methodological quality of all included RCTs in this systematic review and meta-analysis was fair to good in quality using PEDro scale. Generally, low risk of bias was identified in the domains of random sequence generation and selective reporting, while high risk of bias was detected in the domains of blinding participants, personnel and outcome assessment, and allocation concealment using Cochrane' risk of bias. Although inadequate allocation concealment and lack of blinding of outcome measurements for almost all of the included studies were observed, it may not be possible for this type of intervention trial to blind/conceal the participants whether they received Thai yoga stretching exercise. However, strong blinding of researchers should be mandatory.
Their study used a wide range of well-accepted international bibliographic databases plus a database devoted to physical therapy (PEDro; and Rehabdata) in identifying relevant studies and quantified relevant outcomes using a meta-analytic approach. Thai medical databases were also included to maximize the likelihood of identification of all relevant clinical trials on Thai yoga conducted in tropical areas. The authors considered it appropriate to quantitatively pool the results in the following ways by: (i) applying the random-effect model of DerSimonian–Laird method for pooling results which account for the between-study variance, which is recognized to have contributed to higher heterogeneity of the results compared to the fixed effect model; and (ii) only significant outcomes with no or low I2 were used in formulating the conclusions about the effect of Thai yoga. In addition, this systematic review and meta-analysis applied a standard tool (Cochrane risk of bias) and the specific tool for trials in physical therapy (PEDro scale) in assessing quality of clinical trials. Overall, the methodological quality of the included trials displayed a low risk of bias assessed by Cochrane risk of bias and fair to good quality of trials assessed by the PEDro scale. This contributed to the robustness of the evidence for effects of Thai yoga. Their study adhered to standard methodologies of systematic reviews and meta-analyses as indicated by the PRISMA statement. 38
However, some limitations should be considered in this systematic review and meta-analysis. A rather small number of RCTs was included; the results might be influenced by the “small study effect.” In addition, the results relied on rather small sample size (20–40 participants). Further studies with larger sample size are needed to confirm the effect of Thai yoga on physical fitness. Furthermore, the results were derived mostly from female participants as males tend to participate in sports and strength-dependent activities, while females prefer aerobics, dance, and yoga. 39,40 Thus, the results may not apply to male subjects.
Conclusions
Thai yoga exercise provided positive effects, in particular, on body flexibility and right shoulder joint flexibility. Promoting regular stretching exercise of Thai yoga or in combination with other type of exercise should enhance health-related physical fitness.
Footnotes
Acknowledgments
The authors gratefully acknowledge the support of C. Norman Scholfield in proofreading this article. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.