
Abstract
Objectives:
Heavy menstrual bleeding (HMB) is one of the leading causes of low quality of life and iron deficiency anemia in women. This study aimed to determine the effect of hydroalcoholic extracts of Capsella bursa-pastoris on HMB.
Design:
This study is a triple-blinded, randomized clinical trial.
Setting:
The study was conducted in gynecology clinics affiliated to Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Subjects:
Our patients affected to a complaint of HMB. After obtaining a complete medical history of the women and filling out the demographic forms, the participants were assigned randomly into the experimental (n = 42) and control groups (n = 42).
Intervention:
The eligible participants were given a pictorial blood loss assessment chart (PBLAC) to confirm HMB during the menstrual cycle. The experimental group received two capsules of mefenamic acid (500 mg) every 8 h and two Capsella bursa-pastoris capsules every 12 h. The intervention started from the first day of menstruation to the end of this period up to 7 days for two consecutive cycles. In the control group, the patients received mefenamic acid and placebo instead of Capsella bursa-pastoris capsules.
Outcome measurements:
The PBLAC score and number of bleeding days, incidence of any possible problems, as well as participant satisfaction were measured. The data were analyzed using t-test, Chi-square, repeated-measures ANOVA, and ANCOVA tests in PASW Statistics ver. 18.
Results:
After the intervention, there was observed significant decrease in the amount of menstrual bleeding in both groups. However, the mean decrease in the amount of bleeding was significantly more in the Capsella bursa-pastoris group (p < 0/001).
Conclusion:
Compared with control group, hydroalcoholic extracts of Capsella bursa-pastoris capsule appeared to be effective in reducing menstrual bleeding in this study. Further research regarding the efficacy and safety of Capsella bursa-pastoris is required.
Introduction
A
This condition affects ∼10 million American women annually, the majority of whom are within the age of 40–50 years. In addition, by the age of 60, more than one-third of the American females have a hysterectomy, 50% of which is usually due to HMB. 5,6 Although HMB does not lead to death, this condition could cause some physical, mental, and social consequences, including iron deficiency anemia, decreased quality of life, and increased costs of medical services. 7 –9 Iron deficiency anemia is associated with such symptoms as weakness, fatigue, irritability, headache, pallor, and decreased exercise capacity. 10
Mefenamic acid is a nonsteroidal anti-inflammatory drug (NSAID) used as an inhibitor of cyclooxygenase enzyme. 11,12 Mefenamic acid could be effective in pain reduction of different problems such as dysmenorrhea, toothache, and menstruation, but it has various gastrointestinal side effects such as nausea, diarrhea, dyspepsia, and fatigue. 12 While in the traditional medicine of different nations, various methods have been used to treat HMB, including the use of medicinal herbs, acupuncture, and pressure therapy. 13,14 The application of herbal medicine has a long history, and they are widely acknowledged in many societies. 14,15 Capsella bursa-pastoris (known as shepherd's purse) has many compounds, including tannins, choline, acetylcholine, flavonoids, amino acids, fatty acids, sterols, thiamine, ascorbic acid, calcium, potassium, beta-carotene, vitamin K, niacin, and iron. 16,17 According to the literature, the shepherd's purse has oxytocic, antiulcer, and anti-inflammatory activities. 17,18
This herb has shown smooth-muscle stimulant effects; in other words, it can increase the uterine smooth muscle contractions and act as an astringent. In terms of application, this herb can be orally consumed to treat HMB or uterine bleeding between the periods. 16,17,19 Traditionally, this herb was used to treat chronic HMB. According to the European botanists, this herb can effectively treat bleeding caused by uterine fibroids. In the 20th century during the World War in Europe, this herb was used as ergot for the treatment of uterine bleeding and postpartum hemorrhage. 20 Given the lack of studies investigating the effect of shepherd's purse on HMB, this study was conducted to evaluate the effect of the hydroalcoholic extract of shepherd's purse (Capsella bursa-pastoris) on HMB among the females referring to the gynecology clinics affiliated to Shahid Beheshti University of Medical Sciences.
Materials and Methods
This triple-blinded, randomized clinical trial was conducted in 2013 on the effect of the hydroalcoholic extract of Capsella bursa-pastoris on HMB in women, who referred to gynecology clinics affiliated to Shahid Beheshti University of Medical Sciences, Tehran, Iran. The subjects were selected through purposive sampling method. The sample size was calculated to be 90 cases with α = 0.05, effect size = 0.61, and test power of 0.80. However, considering the possibility of 20% sample drop out, 100 subjects were selected.
First, the researcher introduced herself, ensured patients of the confidentiality of their data, obtained their consent, and briefed them the objectives and methods of the study.
Data collection tools were information forms (including demographic and obstetric characteristics, evaluation of inclusion criteria, assessment of drug consumption method by patients, evaluation of participant satisfaction and acceptance of treatment, and assessment of medication side effects), scale, and tape measure. Content validity was used to evaluate the validity of the information forms and pictorial blood loss assessment chart (PBLAC). In addition, the Seca scale (made in Iran) and nonelastic metal meter (Leica, made in Italy) were employed to assess the validity of the scale and tape measure used in this study. Test-retest method was used to evaluate the reliability of the information forms. In addition, the reliability of the PBLAC was confirmed through the completion of 1 column of the form by 10 patients, followed by the filling of another chart 2 h later. The correlation coefficient between the obtained scores was estimated to be ≥0.8, which was acceptable. To confirm the reliability of the scale, a 2-pound control weight was used and then calibrated with the same standard weight after each weighing based on the manufacturer instruction.
The shepherd's purse was bought from an herbalist at Tabriz medicine market. After confirming the identity of the herb at the Laboratory of Botany, Faculty of Pharmacy, Shahid Beheshti University of Medical Sciences, the extraction was performed by soaking the herb in 96% alcohol. Subsequently, the extract was mixed with starch powder, which was filled in the size zero capsules. Each capsule contained 320 mg of the shepherd's purse extract (equal to 2.5 g of the herb). According to the literature, this plant is safe and harmless and has no side effects, especially in therapeutic doses. The shepherd's purse and placebo capsules were produced in completely similar shapes, sizes, and doses and delivered to the researcher in sealed packages coded with A and B. Before taking informed consent, the research team told participants that they would be randomly placed in one of the two groups.
At first, the researcher obtained a complete medical history of the females. Subsequently, the eligible participants were given a PBLAC to confirm HMB during the menstrual cycle. The participants were required to use medium-size wing-type sanitary napkins (made by Panberes Co., Iran). The PBLAC is a table, in which the horizontal row represents the numbers of menstruation days and the vertical row entails the diagrams depicting the lightly, moderately, and heavily soiled sanitary pads. For calculation of PBLAC score, the stained pads are given the scores of 1, 5, and 20 for mild, moderate, and heavy staining, respectively. For every pad change, the subjects were required to mark the appropriate box based on the pad saturation for the respective day. To calculate the final score at the end of the menstrual period, the numbers of the marked pads are multiplied by the corresponding ratio, and then the obtained numbers are added together. In this chart, obtaining a score of 100 or lower is considered normal bleeding and higher than 100 is defined as HMB. The participants completed the PBLAC during a menstrual cycle after receiving written and oral education and delivered them to the researcher. The subjects who obtained a score ≥100 were included in the study and completed the demographic and obstetric characteristics forms. Subsequently, the subjects were randomly divided into two experimental and control groups using the Excel software as described in Kim and Shin study. 21 Block randomization method was used for random allocation with each block consisting of four possible slots as shown below. Therefore, we used 25 different blocks from 6 possible sequences, including AABB, ABAB, ABBA, BAAB, BABA, and BBAA.
After randomization, written and verbal explanations were provided for subjects regarding medication consumption method and fulfillment of PBLAC. During the menstrual cycle, the participants completed the PBLAC and the medication consumption questionnaire, and then delivered them to the researcher in the clinic at the end of menstrual cycle. The research team asked the subjects to explain how to complete the PBLAC and about any possible problems. If they had filled out the forms incorrectly, they would be excluded from the study. In case of regular medication consumption and lack of any problems, the second cycle of treatment was repeated. In the next stage, the questionnaire of participant satisfaction and acceptance of the treatment, as well as the form of medication complication were filled out for the participants. The participant's satisfaction score was measured according to a Likert scale question. The satisfaction question was “are you satisfied with your treatment?” The responses were “Yes, completely satisfied,” “Yes, satisfied,” “I am not sure,” and “No, I am not satisfied.”
In a systematic review study, the sensitivity and specificity of PBLAC ranged from 58% to 98% and 7.5% to 97%, respectively. 22 However, the sensitivity and specificity were calculated as 86% and 88%, respectively, in the Wyatt study and PBLAC introduced as a valid and standard tool to distinguish HMB from normal menstrual bleeding. 23
The inclusion criteria include (1) regular menstrual cycles, (2) being diagnosed with HMB based on the pictorial blood loss assessment (PBLAC) chart, (3) age range of 18–45 years, (4) body mass index (BMI) of 18.5–29.9 kg/m2, (5) lack of known inflammatory pelvic disease, active vaginal infections, polycystic ovary syndrome, and functional ovarian cysts, (6) not being pregnant, (7) no IUD, (8) no pregnancy decision and breastfeeding during the next 3 months, (9) no ever abnormal Pap smear or ultrasound findings (10) no need for a specific medication, and (11) lack of allergy to medicinal herbs.
The exclusion criteria were separated into two groups. Subjects were excluded from the first group at the time of screening if they had (1) any sign of allergy to medications, (2) had consumed any herbal or chemical medicine, (3) were diagnosed/affected with a certain disease (that affects the outcome of the study, or that a person has to take certain medications for that can affect the outcome of the study such as hyperthyroidism, stomach inflammation, and fibroma). Exclusion criteria for the second group began after study acceptance and active involvement in the study. These criteria were (4) lack of willingness to continue participation in the study, (5) obligation to take medication during the study, (6) failure to comply with the correct method of prescribed treatment, (5) affecting menstrual bleeding during the study, (7) pregnancy during the study, (8) need for surgery, and (9) occurrence of a specific event (such as traumatic events, need to surgery, and death of a relative).
This study was approved by the Ethics Committee of Shahid Beheshti University of Medical Sciences (code No.: 143) and registered at the clinic trial center with the code of 201410034529N13. The patients were informed that they would be randomly assigned into the experimental and control groups. It is noteworthy that the capsules had no scent. Moreover, for ethical consideration, the participants were given standard care. Two groups received the mefenamic acid, but the treatment group received shepherd's purse capsules.
Mefenamic acid capsules (250 mg), made in Darousazi Co., Iran, with the serial code of 066 and registration code of 1228102738, were provided for the patients as the standard care for HMB. 24 This was a triple-blind study; therefore, none of the patients, researcher, and statistical consultant were unaware of the nature of the prescribed capsules for the participants and assignment of each patient to study arms. For all the subjects, two capsules of mefenamic acid (500 mg) were prescribed every 8 h (six capsules a day) from the first day of the menstruation to the end of the period (up to 7 days) for two consecutive cycles. In addition to these capsules, the participants in the experimental group received two Capsella bursa-pastoris capsules every 12 h (four capsules a day, equal to 1280 mg of the Capsella bursa-pastoris extract and 10 g of the herb) from the first day of menstrual period to the end of it, up to 7 days. On the other hand, the control group received the placebo with the same Capsella bursa-pastoris capsule that contained starch powder. To prepare the placebo, dough is made with starch powder and converted to granules with a sieve. Then, placebo capsules were prepared in same shapes, sizes, and dose (320 mg) as Capsella bursa-pastoris capsules.
This study reviewed 120 potential candidates and selected 100 of them as study participants. After the first treatment cycle, some of the participants in the experimental group were excluded from the study, as follows: four individuals due to irregular use of drugs, two cases because of inaccurate filling of the forms, and one subject due to stomach irritation. On the other hand, three and two participants were excluded from the control group due to stomach irritation and irregular use of drugs, respectively. During the second treatment cycle, one and three cases were excluded from the experimental and control groups, respectively, due to irregular use of drugs. Therefore, in total, 84 patients (42 in each group) with HMB were assessed. The CONSORT form for assignment of eligible subjects is depicted in Figure 1.

CONSORT form of the participants through the study.
Data analysis was performed using the descriptive statistics, including frequency distribution tables and mean and standard deviation indicators, as well as independent sample t-test, Chi-square, repeated-measures ANOVA, and ANCOVA tests in PASW Statistics ver. 18 (IBM Co., Armonk, NY). Educational level and history of HMB were entered in ANCOVA model as covariates to adjust the confounding effect.
Results
After the end of study and data collection, information about drugs was provided by the pharmacologist and delivered to research team. Then, after adjusting with patient information, the type of prescribed capsule (Capsella bursa-pastoris/placebo) for patients was determined. Baseline measurement showed that there was no significant difference between the two study groups regarding the mean of age (27.54 ± 3.89 vs. 27.22 ± 4.89) (p = 0.722, t-test), mean of gravidity (0.2 ± 0.55 vs. 0.113 ± 0.79) (p = 0.692, Mann–Whitney test), mean of parity (0.31 ± 0.46 vs. 0.42 ± 0.64) (p = 0.338, Mann–Whitney test), and mean of HMB duration (3.58 ± 0.94 vs. 3.52 ± 1.13) (p = 0.239, t-test).
According to Table 1, the two groups were homogeneous in terms of educational level (p = 0.562), housing status (p = 0.349), marital status (p = 0.489), history of HMB (p = 0.311), family history of HMB (p = 0.821), and type of delivery (p = 0.802). Nevertheless, the results of t-test showed that the participants were not homogenous in mean of BMI, and a significant difference was found between the two groups in this regard (p = 0.008). Moreover, the BMI category was statistically different between the two groups (p = 0.005). In other words, mean BMI was significantly higher in the control group, compared to that in the experimental group. To evaluate the possible impact of BMI on the treatment effect as a confounder, this variable was entered in the model as a covariate. However, the results of the repeated-measures ANOVA and ANCOVA revealed no significant impact in this regard (p > 0.05). It means that this variable had no significant role in the effect of shepherd's purse extract and mefenamic acid capsules on HMB.
BMI, body mass index; HMB, heavy menstrual bleeding.
The amount of menstrual bleeding was evaluated in both groups before and after the intervention using the PBLAC scores and then compared within each group. The results of the intragroup comparison by analysis of variance for repeated measurements demonstrated a significant reduction in the amount of menstrual bleeding in both groups after the intervention (p < 0.001). The PBLAC score decreased from 139.42 ± 27.56 received in the first month to 88.01 ± 18.61and 70.30 ± 15.03 in the second and third month, respectively, in the treatment group. Moreover, the trend of decrease in PBLAC score in the control group was from 137.21 ± 19.45 in the first month to 92.25 ± 13.12 and 75.87 ± 8.85 in the second and third month. The t-test showed that there was no significant difference between the experimental and control group regarding to PBLAC score in first (p = 0.678) and second month (p = 0.242). Nevertheless, the PBLAC score in the experimental group was lower in comparison to the control group (p = 0.047). However, this reduction was higher in the treatment group, compared to that in the control group in the second course of treatment (Fig. 2).
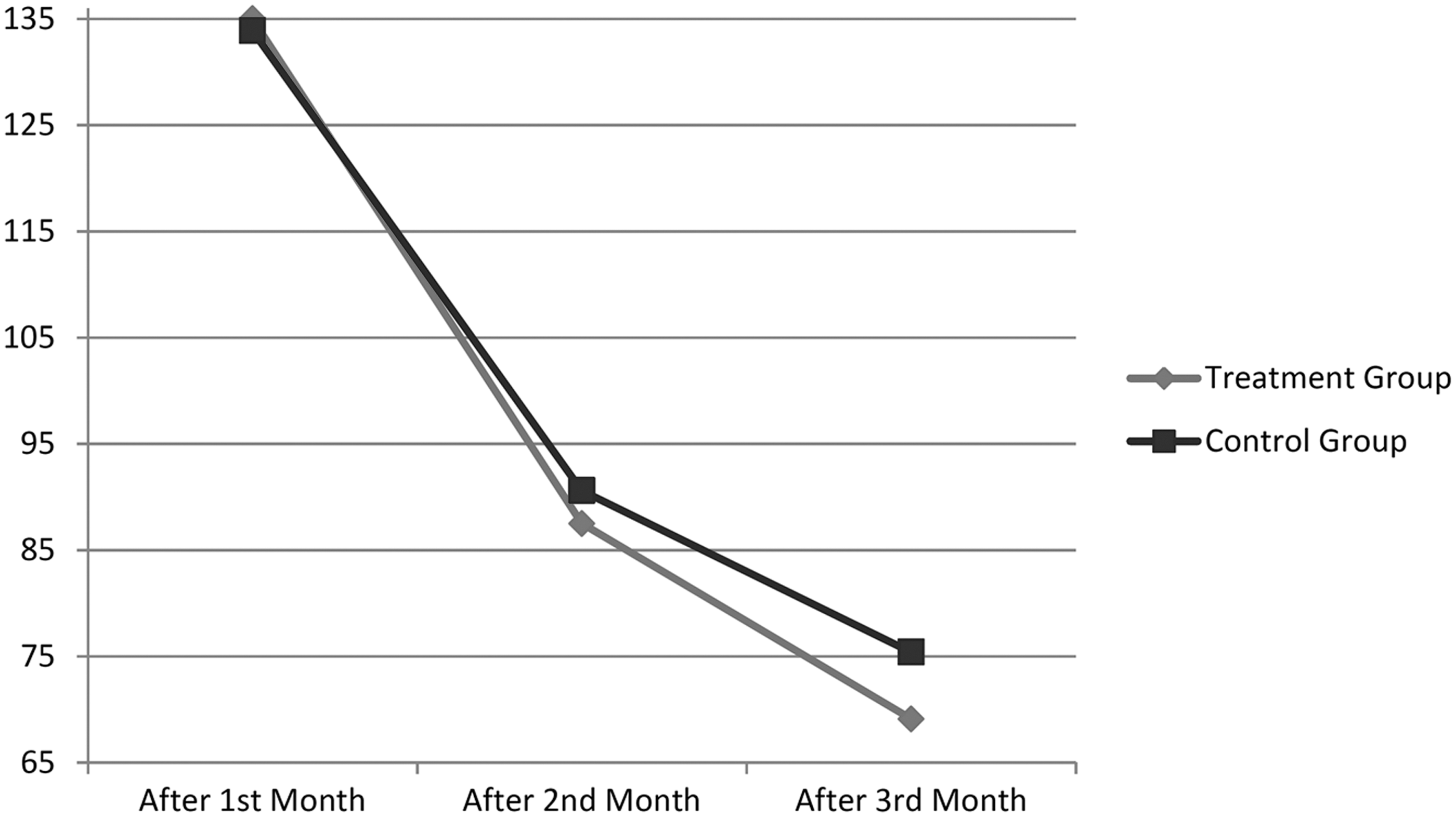
Comparison of PBLAC score of menstrual bleeding between the experimental and control groups before the treatment and in the first and second courses of the treatment. PBLAC, pictorial blood loss assessment chart.
Moreover, the mean duration of menstrual bleeding (Table 2) was reduced in both the groups, following the intervention based on repeated measurement test (p < 0.001). Nevertheless, no significant difference was observed between the two groups at the end of treatment courses. Although the reduction rate in the treatment group was higher than the control group (p = 0.032).
Participant satisfaction
According to the results, a significant difference was observed between the study groups in terms of participant satisfaction with the treatment (p < 0.001). Accordingly, the level of participant satisfaction with the treatment was significantly higher in the experimental group, compared to that in the control group (in the experimental group, 40% and 51.1% of the patients were completely satisfied and satisfied, respectively, whereas in the control group, 2.2% and 60% of the participants were completely satisfied and satisfied, respectively).
Adverse effects
In this study, the obtained results revealed that the most common post-treatment complication was gastrointestinal disturbances (46.7% and 55.6% cases in the experimental and control groups, respectively), which was due to the consumption of mefenamic acid in both the groups. Given the use of mefenamic acid in both the groups and lack of increased complications in the experimental group, it could be concluded that shepherd's purse resulted in no significant complication.
According to the results, no significant difference was observed between the experimental and control groups in terms of gastrointestinal disturbances (p = 0.832) and other complications, including headache and dizziness (p = 0.999). In addition, there was no report of allergies to the medications used in this study.
Discussion
The extract of the shepherd's purse herb has several active substances, including tannins, choline, acetylcholine, sterols, and flavonoids. 17,19 Each of these substances has a role in the management of HMB due to their antioxidant and anti-inflammatory features by creating uterine contractions and hormonal effects. The anti-inflammatory and contractile activities of the shepherd's purse herb have been demonstrated in the literature. 17 According to the finding, the volume of menstrual bleeding was significantly decreased by the hydroalcoholic extract of shepherd's purse herb and this plant could be effective in the treatment of HMB. Our finding revealed that, the side effects of hydroalcoholic extracts of Capsella bursa-pastoris were low and participant satisfaction was acceptable. Given the lack of studies on the effect of this plant extract on HMB, this study discusses similar studies on medication or plants with similar active compounds, and mechanisms or diseases with similar pathologies.
In another study conducted in Iran, it was indicated that the amount of menstrual bleeding was decreased by the hydroalcoholic extract of nettle and mefenamic acid, as well as quince extract, and this reduction was more significant in the nettle group, compared to the control group. 11,25 Similar to nettle, shepherd's purse also has anti-inflammatory features, 26 and it seems that this herb could have a positive impact on the treatment of menorrhagia through similar mechanisms. In this study, there was a significant reduction in the amount of menstrual bleeding in both the groups. Meanwhile, this decrease was higher in the experimental group, compared to that in the control group.
The results obtained by systematic reviews revealed that the amount of bleeding was reduced in the subjects administered with nonsteroidal anti-inflammatory medications, compared to those who consumed placebo during the study. In this study, the amount of menstrual bleeding decreased in the control group that used mefenamic acid and placebo. 27,28
Capsella bursa-pastoris can cause contractions in smooth muscles. 15,16 In traditional medicine, hypotonic uterine dysfunction is recognized as a factor for increased blood flow during the menstrual period. It is believed that the improved uterine tone can facilitate the regulation of menstrual blood flow; therefore, some effective herbs are used to create uterine contractions. 5,13 It could be concluded that one of the mechanisms applied by shepherd's purse to control menorrhagia is to cause contractions in uterine smooth muscles. 13
In a study carried out by Mojahed et al., it was demonstrated that the amount of menstrual bleeding was lower in the date and oxytocin group 2 h after the delivery, compared to the group prescribed to use oxytocin. This finding indicated that the dates include such active substances as tannins that cause contraction, which are effective in uterine contractions. 15 In another study by Goshtasebi et al., it was affirmed that the use of herbal medicine of Gulnar Farsi and tranexamic acid to treat women with menorrhagia was associated with decreased amount and duration of menstrual bleeding. Gulnar can have a positive impact on the treatment of menorrhagia due to active ingredients that cause contraction, such as tannins. 29
In another study conducted by Mahdavian et al., it was demonstrated that the consumption of edible fennel seed extract caused more reduction in the amount of bleeding after delivery, compared to the muscle oxytocin. 30 Fennel seed contains tannin and anethol and could induce contractions in smooth muscles of the uterus. 30 Shepherd's purse has a powerful antioxidant property due to several types of flavonoids. 17,19 It seems that shepherd's purse can use this mechanism to reduce menstrual bleeding. Another study demonstrated that similar to mefenamic acid, Dill (Anethum graveolens) and other herbs could cause a significant reduction in the amount of menstrual bleeding. 14,20,27,31
The reasons for prescribing mefenamic acid for all the participants in this study were the effect of NSAIDs (known as the first line of treatment for menorrhagia), not depriving the subjects of standard treatment, and compliance with ethical issues. 6,11 On the other hand, the selection of shepherd's purse (as a therapeutic intervention) and evaluating its effect on HMB was due to some evidence regarding the effect of this herb on controlling this disease in the related literature. However, regarding the effect of reproductive outcomes, including menopause and unintended pregnancy, on quality of life in women, future studies seem to be necessary in this field. 32,33
The limitations of this study include the researcher's sufficing to the patient's verbal declaration of having no underlying diseases. Moreover, the study duration could be increased for assessing the longer side effects. In addition, two study groups were not same based on BMI and the overweight prevalence was higher in the control group. However, we include the BMI as covariate in ANCOVA model and after adjusting this item, there was no significant interaction. Therefore, BMI was not significant and the overweight effect was adjusted in this study.
Conclusion
The results of this study indicate that the hydroalcoholic extract of Capsella bursa-pastoris reduces the volume of menstrual bleeding. It is suggested that additional study should be carried out using similar methodology and larger cohort to confirm these findings. Moreover further study is required to illustrate reliably that Capsella bursa-pastoris is the safe medication for patients.
Footnotes
Acknowledgments
This article is the result of a project approved by the Research Deputy of Shahid Beheshti University of Medical Sciences in Tehran, Iran. Hereby, we extend our gratitude to all the authorities and professors of Shahid Beheshti University of Medical Sciences for their support. We would also like to thank the School of Pharmacy for preparing the Capsella bursa-pastoris capsules and all the women who participated in this research.
Authors' Contributions
M.N.'s contributions to the conception, design of the work, analysis, interpretation of data, and final approval of article. N.K.'s contributions to the conception or design of the work and final approval of the article. Z.K.'s contributions to the acquisition and analysis of data for the work and drafting the article. N.K.H.'s contributions to the acquisition and analysis of data for the work and drafting the article. F.M.'s contributions to the acquisition and analysis of data for the work and drafting the article. A.M.'s contributions to the conception or design of the work, interpretation of data for the work, and final approval of the article.
Author Disclosure Statement
No competing financial interests exist.