
Abstract
Objective:
The purpose of this study was to evaluate the cost-effectiveness of Safflower Yellow Injection (SYI) plus conventional treatment (SYI group) versus conventional treatment only (conventional group) for the treatment of stable angina pectoris (SAP) patients in China.
Methods:
A decision-tree model was constructed and the treatment impact was estimated for up to 1 year. The data, including treatment effectiveness, episodes of angina pectoris (AP)-associated hospitalization and its in-hospital mortality, mortality rate of heart diseases, and cost of hospitalization, were obtained from literature. The costs of medications were calculated based on their average bidding prices in China. The authors also conducted a doctor survey to obtain cost associated with death of cardiovascular events. Sensitivity analysis was performed to evaluate the robustness of the results.
Results:
SAP patients in the SYI group (n = 1000) gained incremental 66.01 quality-adjusted life years (QALYs) at a cost of $250,294 compared with patients receiving conventional treatment, yielding an incremental cost-effectiveness ratio of $3,791/QALY, which was less than Chinese GDP per capita and is considered to be highly cost effective per WHO-recommended economic evaluation guidelines. Sensitivity analysis indicated that the results were robust with variations for all major parameters of the model.
Conclusion:
SYI combined with conventional treatment is a highly cost-effective therapy option compared with the conventional treatment for treatment of SAP in China.
Introduction
S
The treatment for chronic SAP patients is mainly to prevent myocardial infarction and sudden death, prolong survival, relieve ischemia symptoms, and improve quality of life. Safflower Yellow Injection (SYI, brand name “Letan”) is made of an effective element extracted out of the safflower and is produced as aseptic freeze-dried powder. It is marketed as a Traditional Chinese Medicine (TCM) for its pharmaceutical effects on promoting blood circulation, reducing blood stasis, and relieving pain associated with ischemia. In clinical practice, SYI is usually used as an adjunct therapy with conventional drugs for the treatment of heart-blood stasis syndrome. Results from a phase IV clinical trial showed that the frequency and duration of angina pectoris (AP), pain severity, and TCM syndrome integral were significantly improved when SYI was administered in combination with conventional therapy compared with conventional therapy alone. Subgroup analysis also showed that SYI was effective and well tolerated for elderly patients with AP, severe hypertension, or diabetes mellitus. 3
This study focuses on pharmacoeconomic evaluation of SYI for treatment of SAP based on the clinical efficacy obtained from this phase IV trial. The objective is to evaluate the cost-effectiveness of SYI plus conventional western medicines (SYI group) versus conventional western medicines only (conventional group) for SAP patients in China.
Materials and Methods
Population
The phase IV clinical trial was an open-label, single-arm, and pre–post design to evaluate clinical efficiency and safety of SYI for the patients with SAP. A total of 2103 patients with SAP in 31 clinical centers were enrolled and administered SYI (100 mg in 250 mL 0.9% normal saline, once per day for 14 days) in addition to conventional western medicine clinical management. The mean age of the SAP patients was 59.99 (±standard deviation: 12.87) and 51.1% of them were males. Most of the patients had a CCS (Canadian Cardiovascular Society) Grade I (Grade I: 49.1%, Grade II: 33.4%, Grade III: 13.0%, and Grade IV: 4.5%).
Before entering into the clinical trial, 57.4% (1203/2103) of the patients had received standard of care western medicines for SAP, including oral anticoagulants, beta blockers, statins, and nitrate esters. The outcomes of interest, including AP frequency, dosage of nitroglycerin, ECG, TCM syndrome efficacy, and disease effects, were measured both before and after injection of Safflower yellow. Adverse drug reactions (ADRs) were also recorded. Fourteen patients (0.67%) showed mild ADRs and most of them did not need additional treatment. 3
Model description and structure
The authors developed a cost-effectiveness decision-tree model using MS Excel to assess the costs and quality-adjusted life years (QALYs) when either SYI with conventional western medicines or conventional western medicines alone were used for the treatment of SAP patients (Fig. 1).
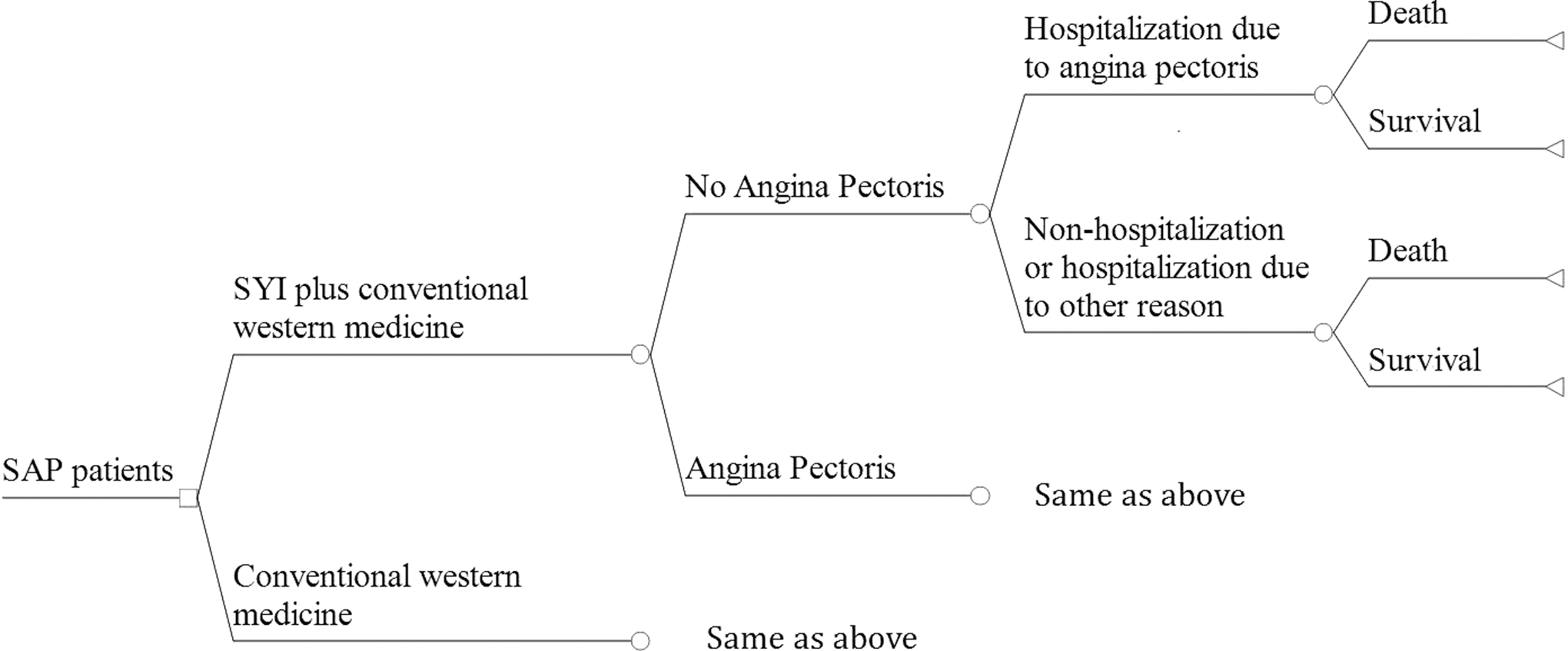
Decision-tree model structure. SAP, stable angina pectoris; SYI, Safflower Yellow Injection.
The cost-effectiveness was evaluated from perspective of government payers over a 1-year observation period built upon prior work by Beatty et al. 4 on the relationship between the frequency of SAP attacks, rehospitalization, death in cardiovascular events, and the clinical treatment pathway of SAP in China. The authors also referenced the decision-tree model developed by Coleman et al. 5 for the cost-effectiveness analysis of SAP. The cost-effectiveness analysis of SAP patients was compared between SYI group and the conventional group. Each group had 1000 patients simulated in the model. The model was constructed to simulate the primary efficacy endpoint of the phase IV clinical trial: achieving absence of AP attacks. Prior research has demonstrated that absence of AP is associated with a lower risk of hospitalization and mortality. The model assumed the efficacy of SYI and remained unchanged during the 1-year observation period.
The authors estimated the drug cost for standard treatment (2 weeks) with SAP using the national average price in China. A written survey of cardiologists from 12 Chinese tertiary hospitals was conducted to quantify the costs associated with death due to cardiovascular events.
Model inputs
Inputs of model, including efficacy, transition probabilities, and resource utilization, were derived from the clinical trials and literature, and the survey of cardiologists for the cost estimate associated with cardiovascular death (Tables 1 –3).
The range of these variables was 95% confidence interval, the rest of variables were floating (up and down) the basal value by 10%.
AP, angina pectoris; SAP, stable angina pectoris; SYI, Safflower Yellow Injection.
SAP, stable angina pectoris.
The average price of SYI (50 mg) was accessed from IMS database on March 3, 2017.
The average price of medical service was gained from the website of Municipal Commission of Health and Family Planning of each provinces.
AP, angina pectoris; SYI, Safflower Yellow Injection.
Efficacy of SYI combined with conventional therapy
Percentage of patients achieving AP free
Efficacy data were obtained from a multicenter, open label (single arm and pre–post design) phase IV clinical trial in 31 hospitals in China (Huang et al.
3
and an unpublished clinical trial report). At the study entry (baseline), all patients reported one or more AP attack episodes per week while receiving conventional therapy. Following SYI treatment, the median AP attack frequency was 0 per week, that is, at least 50% of the patients achieved AP free (Supplementary Table S1; Supplementary Data are available online at
Transition probabilities
Hospitalization associated with AP
Hospitalization associated with AP in Beatty et al.'s 4 study was defined as hospitalization for definite or probable AP on the basis of symptoms, physician diagnosis, medical treatment, documented coronary heart disease revascularization during admission, stenosis >70% documented during admission ischemia by electrocardiogram, or ischemia by stress testing. Patients admitted to hospitals with chest pain were not considered AP without objective evidence of cardiac ischemia. 5 The AP-related hospitalization rate in patients without active AP (patients who had AP history, but are currently without AP) and the risk of hospitalization in patients with active AP (hazard ratio) were obtained in literature. The AP-related hospitalization rate in patients with current AP was then calculated based on the hazard ratio (Table 1).
Mortality
The mortality of patient with AP and the mortality of in-hospital AP patients were obtained in literature. The mortality of patients with AP was calculated based on the reported hazard ratio (patients without AP vs. patients with AP) (Table 1).
Utility
Reduction in utility values (disutility) for patients with SAP, for patients during hospitalization and posthospitalization with cardiovascular diseases, and utility value for general population were derived from the literature (Table 2).
The SAP patients' utility was calculated as utility for general population minus disutility value for SAP. The utility for patients with cardiovascular diseases after discharge from hospitalization was calculated as utility for general population minus disutility value for patients with cardiovascular diseases during hospitalization.
Cost of SYI
The recommended SYI treatment regimen is 100 mg/QD for 14 days. All costs are presented in USD (6.64 RMB = 1 USD, average exchange rate in 2016, National Bureau of Statistics of China). The unit price of SYI (contain hydroxy safflower yellow pigment A42.5 mg, Zhejiang Yong Ning Pharma) is $9.49 per 50 mg (national average price). The total drug cost of SYI per course of treatment was estimated to be $265.66 per patient (Table 3).
Cost of laboratory test and electrocardiograph during treatment
The laboratory test and electrocardiograph cost were calculated based on frequency (twice during the trial) of treatment reported in the clinical trial of SYI and average price of medical service published (Table 3).
Cost of hospitalization and death for AP
The cost of hospitalization associated with AP was based on Liu et al.'s study. 7 The authors obtained costs of death due to cardiovascular events by surveying 50 cardiologists from 12 tertiary hospitals across the country. All data obtained were validated and double-checked and median value was used for cost input. The results are shown in Table 3. The authors applied a 3.0% discount rate for all costs estimates.
Sensitivity analysis
The authors conducted one-way and probabilistic sensitivity analyses (PSA) to assess the uncertainty of model parameters. They performed one-way sensitivity analysis for all key variables in their priori determined plausible ranges (95% confidence intervals), including frequency of AP attack in SYI and conventional groups, hazard ratio for AP-related hospitalization, and hazard ratio of death in patients with AP. For other variables, they tested the sensitivity of model by adjusting basal values by 10%. In addition, they performed three scenario analyses assuming (1) lower end of clinical efficacy on the primary endpoint (% of patients achieving AP free); (2) efficacy maintains for 2 months (instead of 12 months); and (3) 50% of SAP patients could afford SYI cost. The authors performed a Monte Carlo simulation (MCS) with 1000 iterations to determine the joint uncertainty of model parameters. For each variable in MCS, beta distributions were chosen for the utility, probability, and proportion variables; log-normal distributions were chosen for cost values. The results of one-way sensitivity analyses and PSA were displayed as the tornado diagram and incremental cost-effectiveness scatter plot.
Results
Base case analysis
The average age of the study population was about 60 years old, and 50% of them were males. The percentage of patients who achieved AP free following SYI therapy was 52.6% compared with 0% in patients receiving conventional therapy. The frequency of AP attacks per week in the SYI group was 4.1 lower than the conventional group. Compared with patients without AP, patients with AP had a higher risk of AP-related hospitalization and mortality as shown in Table 1.
In comparison to conventional treatment, for 1000 patients treated, SYI regimen was projected to prevent 62.34 patients from AP-related hospitalization, 0.60 deaths, and 213.20 AP attack episodes over 1-year period (Table 4).
Average frequency of AP per person per year, SYI (n = 1000), conventional (n = 1000).
AP, angina pectoris; ICER, incremental cost-effectiveness ratio; QALY, quality-adjusted life years; SAP, stable angina pectoris; SYI, Safflower Yellow Injection.
Overall, the treatment with SYI incurred incremental cost of $250,294 and gained 66.01 more QALYs compared to conventional treatment; yielding an incremental cost-effectiveness ratio (ICER) at $3,791/QALY.
Sensitivity analysis
A tornado diagram was developed to illustrate the sensitivity of ICER on the change of key parameters (Fig. 2). The five most sensitive parameters in the cost-effectiveness analysis were cost of SYI, disutility due to AP, hazard ratio for AP-related hospitalization, utility of cardiovascular diseases, and cost of AP-related hospitalization. Results from the scenario analyses described in the Materials and Methods section showed that the ICERs varied from $4,001 to $7,529 per QALY (Table 4). The findings from the MCS indicated that SYI regimen is considered to be a highly cost-effective treatment option in 95.3% of simulations based on the WHO-recommended threshold value for economic evaluation ($8,130/QALY, one-time GDP per capita) (Fig. 3).

Tornado graph for univariate analysis showing the top 5 variables' influence on (AP, CD) X value = 3.791 (base case ICER). AP, angina pectoris; CD, cardiovascular disease; ICER, incremental cost-effectiveness ratio; SYI, Safflower Yellow Injection.

Probabilistic sensitivity analysis of 1000 simulations comparing SYI and conventional treatment for the SAP patients (WHO Recommended Threshold: $8,130/QALY). QALY, quality-adjusted life years; SAP, stable angina pectoris; SYI, Safflower Yellow Injection.
Discussion
Previous clinical research demonstrated that SYI, as an adjunct therapy in combination with conventional treatment, significantly decreased AP attacks, which have been implicated as a major risk for hospitalization and death. Largely owing to its clinical benefits, SYI combined with conventional therapy has been reported as a popular treatment for SAP in China. 8 But there is little evidence in literature to evaluate its economic implications. To their knowledge, their analysis is the first to assess the cost-effectiveness of SYI regimen compared with conventional therapy for treatment of SAP.
The findings of their analysis showed that SYI regimen should be considered a highly cost-effective therapeutic option compared with conventional treatment. In the base case analysis, the estimated ICER at $3,791 per QALY gained was $4,339 less than the GDP per capita in China (GDP per capita was $8,130, National Bureau of Statistics of China, 2016), which is deemed to be highly cost-effective threshold as recommended by WHO.
However, the economic evaluation has several limitations. The clinical efficacy data are based on a phase IV trial, which was open label, single arm, and pre–post in design not a randomized blinded trial. Despite the large sample size, the study was subject to potential selection and information bias inherent in the study design. The cost data for AP-related hospitalization were obtained from a health insurance claim database of Tianjin, which is an economically advanced area in China. Had they used national average for cost input, they would have expected a smaller cost gap between the two treatment groups. But the sensitivity analysis showed that, when cost data were floated ±10%, the ICER was within the cost-effectiveness threshold, indicating the robustness of the model on cost data they used. At the time of writing this article, SYI was not covered in the national medical insurance scheme in China, which means the cost of SYI was paid out-of-pocket and only patients with high income could afford the payment and benefit from the treatment. The sensitivity analysis showed that even if there were only 50% of patients who could afford SYI, the SYI plus conventional therapy was still highly cost effective. Due to lack of clinical data on long-term follow-up, the authors assumed that the clinical benefits observed over the first 2-week treatment could be maintained for the remaining of the year. To address this uncertainty, they shortened the persistency of efficacy to 2 months in the sensitivity analysis, and the ICER value was still below the one time GDP per capita threshold. The population in this study was simulated from the clinical trial, and all patients received SYI treatment for free. In the real world, however, not all patients can afford the $266 treatment cost. When they assumed that 50% of the patients could not afford the SYI cost in the sensitivity analysis, the result still indicated that SYI is an attractive cost-effective treatment option. Finally, the authors did not include the ADRs in this analysis, as only 0.67% of patients reported mild ADRs and most of them resolved without treatment. The utility values for some health status (cardiovascular disease patients during hospitalization and discharged from hospitalization) used in this model were for cardiovascular disease due to lack of specific utility value for the SAP patients. To further improve the accuracy of the assessment, a prospective long-term large sample size multicenter clinical study of SYI might be needed to collect high-quality utility values.
Conclusion
Compared with conventional treatment alone, SYI combined with conventional therapy is a highly cost-effective therapeutic option for treatment of patients with SAP in China.
Footnotes
Acknowledgments
This study was funded by the Yongning Pharma.
Y.L. received funding from Yongning Pharma. The funders had no role in study design, data collection and analysis, preparation of the article, or decision to publish.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.