
Abstract
Introduction/Aim:
To assess the effectiveness and safety of Traditional Chinese patent medicines (TCPMs) for managing impaired glucose tolerance (IGT).
Methods:
Seven databases were searched to identify eligible trials published from incepting to May 1, 2016. Randomized controlled trials (RCTs) involving TCPM for IGT with a minimum follow-up duration of 6 months were included for analysis. Data extraction and quality assessment were performed by two reviewers independently. Data synthesis was analyzed using Review Manager 5.3 software. Subgroup analysis was carried out to assess the robustness of results of meta-analysis.
Results:
Eighteen trials with a total of 3172 participants met the inclusion criteria. The methodological quality of the RCTs was variable. Comparing with receiving lifestyle modification (LM) alone, TCPM plus LM was significantly better at reducing the incidence of diabetes (risk ratio [RR] 0.45; 95% confidence interval [CI] 0.36–0.57, p < 0.00001) and normalizing the blood glucose (RR 0.72; 95% CI 0.64–0.82, p < 0.00001). TCPM plus LM was superior in decreasing the levels of 2hPG, body mass index (BMI), fasting insulin, and 2 h insulin compared with LM alone (2hPG: mean difference [MD] −1.13; 95% CI −1.68 to −0.58, p < 0.0001; BMI: MD −0.42; 95% CI −0.71 to −0.14, p = 0.004; fasting insulin: MD −2.44; 95% CI −3.79 to −1.09, p = 0.0004; and 2 h insulin: MD −8.26; 95% CI −8.47 to −8.05, p < 0.00001). Compared with placebo plus LM, TCPM plus LM was superior in reducing diabetes (RR 0.54; 95% CI 0.42–0.69, p < 0.00001) and normalizing blood glucose (RR 0.55; 95% CI 0.41–0.73, p < 0.00001; the interventions were also associated with a decline in the two-hour postprandial blood glucose (2hPG) levels (MD −1.45; 95% CI −2.11 to −0.79, p < 0.0001) and BMI levels (MD −1.12; 95% CI −2.00 to −0.24, p < 0.0001). There were no significant differences in adverse events between two groups. Subgroup analysis found no significant difference in overall effects among all study characteristics, indicating that the overall effects were stable.
Conclusions:
The study indicated that TCPM combined with moderate lifestyle modification had significant effect on IGT. Further studies are needed to provide more reliable evidence. The PROSPERO registration is No. CRD42016039312.
Introduction
T
In China, many patients with IGT are willing to choose Traditional Chinese patent medicine (TCPM) because it had not yet reached the stage of long-term use of antidiabetic drugs, and TCPMs are more convenient to be administrated and taken along. 11 Several studies suggested that TCPMs combined with LM treating patients with IGT were better than LM alone, but systematic evidence was lacking. Aim of this study was to assess the possible beneficial effects of TCPM on the incidence of diabetes and the regression toward normoglycemia for IGT subjects.
Methods
The protocol of the review has been registered with the International Prospective Register of Systematic Reviews (PROSPERO registration No. CRD42016039312; available online:
Search strategy
The following seven electronic databases, including Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews, PubMed, EMBASE, Chinese Biomedical Database (CBM), Chinese National Knowledge Infrastructure (CNKI), and Wanfang database, were searched to identify eligible trials published from inception to May 1, 2016. Because TCPMs were mainly used in China, the authors conducted a literature search in the four Chinese electronic databases to include the maximum possible number of clinical trials. The search terms are listed in the Appendix Table A1. To include unpublished studies, the websites of the international clinical trial registry provided by the U.S. National Institutes of Health (available at
Study selection
All included trials had to meet the following selection criteria.
Participants
The authors focused on the participants irrespective of gender, age, and ethnicity, with clinical diagnoses of IGT by clearly defined or internationally recognized criteria. Studies with type 1 diabetes patients, pregnant women, or children were included.
Intervention
The study was conducted as a randomized controlled trial (RCT), which used TCPM combined with LM versus LM alone or placebo combined with LM. Combinations of TCPM and nonmedicinal therapy, such as herbal medicine decoction, acupuncture and acupoint injection, and herbal extracts or comparisons between different types of herbal medicines, were excluded, to limit the similar effects of other Traditional Chinese Medicine (TCM) therapies and observe the therapeutic effect of TCPMs more effectively.
The authors defined TCPM as refined dosage forms, such as capsules, tablets, oral lipids, and powders, which originated from herbal medicine (whole plants or their adjuncts), relative standardization in composing the main effective components, and manufactured in accordance with the PRC Pharmacopoeia's monograph. However, decoctions, herbal extracts, or synthetic plant-based drugs were excluded. There were no restrictions on frequency and dose; the follow-up duration should last for 6 months or more. Moderate LM was defined as achieving a weight reduction, at least no weight gain, through a healthy low-calorie, low-fat high-fiber diet, and moderate, but consistent, exercise helps to prevent diabetes.
Outcome measures
The primary outcomes were the incidence of T2DM and adverse events. The secondary outcomes were as follows: (1) normalization of blood glucose; (2) 2-h postprandial blood glucose; (3) body mass index (BMI); (4) fasting insulin and 2-h postprandial insulin; and (5) homeostasis model assessment-insulin resistance (HOMA-IR).
Data extraction
Two reviewers (Y.-Q.L. and Y.-T.W.) independently extracted data. The authors extracted the following information using a predesigned collection form: general trial characteristics (title, authors, and year); baseline patient and disease data (sample size, age, and gender); interventions (component and dosage of Chinese patent medicine and details of the control interventions); and outcomes (follow-up length, outcome measures, and adverse events). Any discrepancies were resolved by discussion (95% level of agreement) or further evaluated by the third party (X.-L.T.).
Quality assessment
Two reviewers (Y.-J.Z. and X.-M.Z.) independently assessed the methodological quality of the RCTs using the Cochrane Collaboration Risk of Bias tool, 13 which consists of seven items as follows: random sequence generation; allocation concealment; blinding of participants and personnel; blinding of outcome assessment; incomplete outcome data; selective reporting, and other sources of bias. The authors judged each item from three levels: “high risk,” “low risk,” and “unclear”: “low risk of bias” means that it is unlikely that a bias seriously alters the results; “high risk of bias” means that it is plausible that a bias seriously weakens confidence in the results; and “unclear risk of bias” means that it is plausible that a bias raises some doubt about the results. Discrepancies in the interpretation were resolved by consensus or the third party (S.F.).
Assessment of the quality of evidence
The authors used The Grading of Recommendations Assessment, Development and Evaluation (GRADE) methodology to assess the quality of the evidence for each outcome. 14 According to GRADE, outcomes of an intervention are categorized into four levels of evidence quality as follows: + very low, ++ low, +++ moderate, and ++++ high. In GRADE, their confidence assessment addressed the Risk of bias (in individual studies), inconsistency (heterogeneity in estimates of effect across studies), indirectness (related to the question or due to intransitivity), imprecision, and publication bias. Bodies of evidence from RCTs start as high quality evidence, whereas those from observational studies start as low quality evidence. Defined criteria are applied to either decrease or increase quality of evidence rating. The GRADE profiler (GRADEPRO) was applied to create Summary of finding table.
Statistical analysis
Data regarding outcomes in the eligible trials were combined in the meta-analysis using the RevMan 5.3 software (Cochrane Collaboration, Oxford, United Kingdom). For dichotomous outcomes, the authors calculated risk ratios (RRs) using the Mantel–Haenszel method, and for continuous variables, the authors calculated weighted mean differences (MDs) using the inverse variance method. For all estimates, the authors computed the 95% confidence intervals (CIs). The authors quantified statistical heterogeneity using the I-squared statistic (I2); statistical heterogeneity between the trials was significant when I2 > 50%. A fixed-effects model was used if there was no significant heterogeneity of the data (I2 < 50%); random-effects model was used if significant heterogeneity existed. Publication bias was assessed through visual inspection of funnel plots. Sensitivity and subgroup analysis would then be carried out to assess the robustness of results of meta-analysis for primary outcome.
Results
The PRISMA flow chart in Figure 1 depicted the search process and trial selection. In their initial literature search, 4992 articles were identified from the 7 electronic databases, of which 2718 articles were repeated and 2274 left. After reading the titles and summaries, the other 1993 articles were excluded as they were experimental studies, case reports, and reviews of literatures. There were 281 that needed full texts screening. Two hundred sixty-three of them were excluded for the following reasons: participants did not meet the inclusion criteria (n = 197), duplication (n = 5), protocol (n = 2), not RCTs (n = 54) and intervention included other TCM intervention (n = 5). Finally, 18 RCTs 15 –32 met their eligibility criteria and were included in the systematic review, 4 trials 15 –18 were published in English, and the rest were published in Chinese.
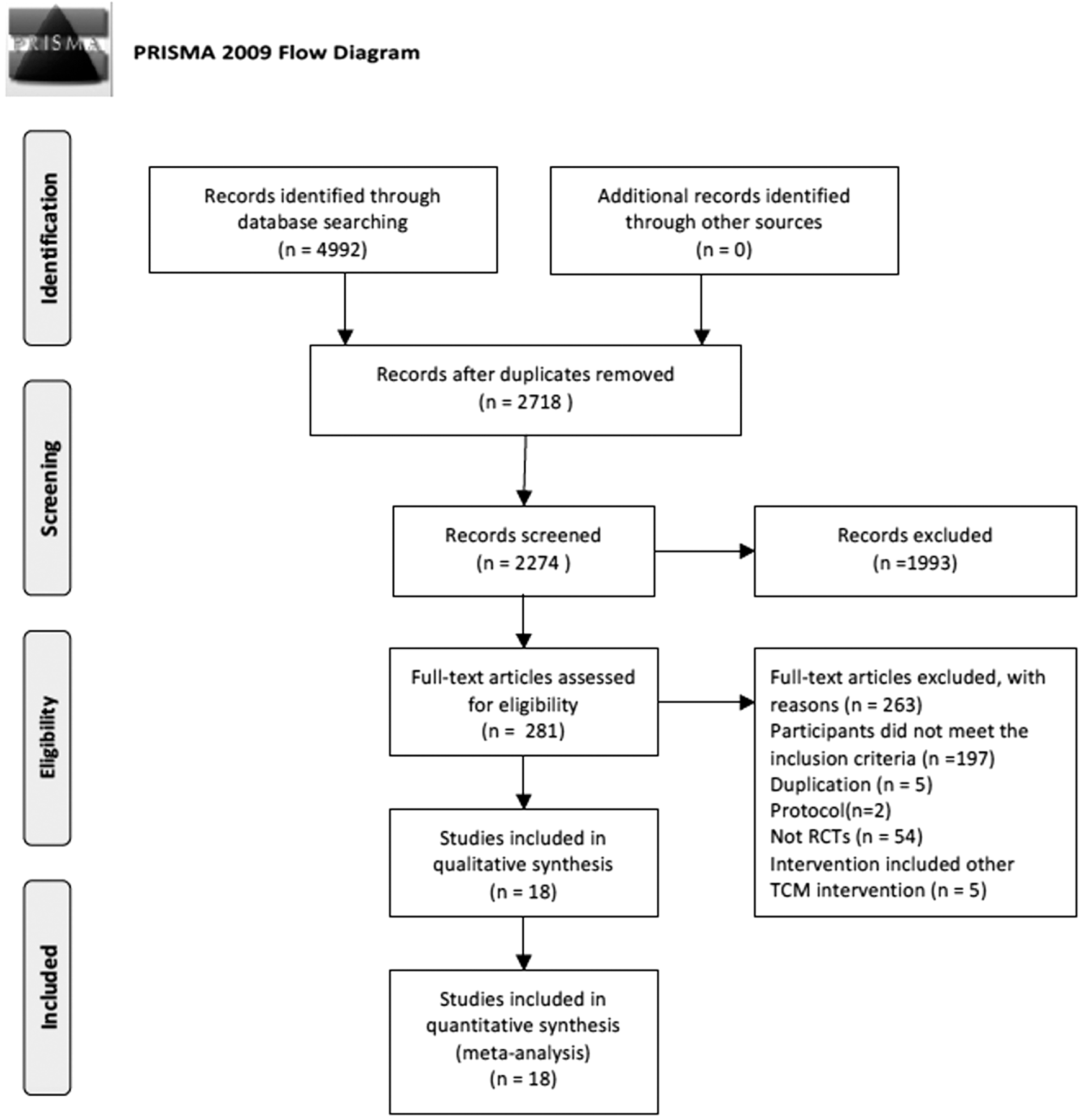
PRISMA flow chart of literature.
Description of the included trials
The basic characteristics of these studies are summarized in Table 1. A total of 3172 participants were involved (1607 in intervention and 1565 in control group). Trial sample size ranged from 60 to 514 participants; the age of participants ranged from 22 to 78. The included participants were diagnosed of IGT according to clearly defined or internationally recognized criteria. Twelve trials compared TCPM plus LM with LM alone, and 6 trials compared TCPM plus LM with placebo plus LM. The formulations of TCPMs contained capsule (six trials), granule (five trials), tablet (three trials), pill (three trials), and oral liquid (one trial). The ingredients of the included TCPMs are shown in Table 2. The intervention period lasted from 3 to 36 months, and follow-up duration ranged from 6 to 36 months. All the included trials reported the incidence of diabetes.
A, incidence of diabetes; B, normalization of blood glucose; C, BMI; D, 2hPG; E, fasting insulin; F, 2 h insulin; G, HOMA-IR; H, adverse events.
Diet and exercise advice for all participants involved limiting the amount of diet, consuming more vegetables, controlling their intake of alcohol, reducing their intake of simple sugars, and losing the body weight, and increasing the amount of their leisure physical exercise by at least once a day.
Diet and lifestyle advice for all participants involved quitting smoking and drinking and adopting diabetic diet.
Dietary education consisted of advice on maintaining a balanced and reasonable diet. The intervention education included two face-to-face counseling sessions with certified nutritionists. The daily caloric requirements were calculated based on the individual subject's height, weight, and physical activities.
2hPG, two-hour postprandial blood glucose; BMI, body mass index; HOMA-IR, homeostasis model assessment-insulin resistance; LM, lifestyle modification.
TCPMs, Traditional Chinese patent medicines.
Methodological quality
The methodological quality of the RCTs was variable. Overall, 1 trial was rated as having a low risk of bias, 15 5 as having an unclear risk of bias, 19 –21,28,29 and 12 as having a high risk of bias. Six trials reported the method of random sequence generation, the rest 15 trials reported “randomly allocating,” while the detailed method of randomization was not provided. Two trials reported the method of allocation concealment. Seventeen trials reported dropouts or withdrawals, seven of whom reported no dropout or withdrawal. The authors tried to contact Zhang et al. for the data on loss to follow-up, but no additional data could be provided, so unclear risk of attrition bias was judged. Furthermore, the authors judged three trials to be at low risk of selective reporting bias as their trial protocols were available. An overview of the judgments regarding each risk of bias items in the included trials is shown in Figure 2.
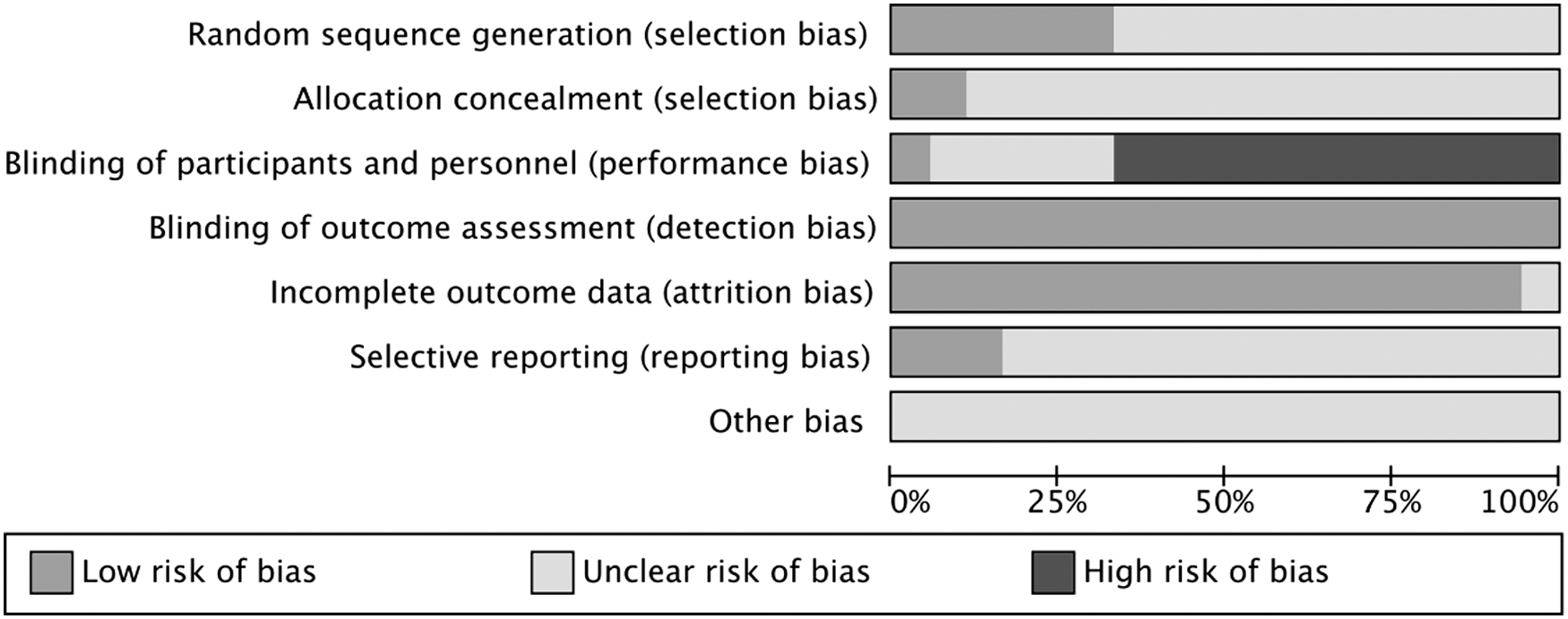
Risk of bias graph.
Primary outcomes
Incidence of diabetes
Results are shown in Figure 3.

T2DM incidence comparison. CI, confidence interval; LM, lifestyle modification; T2DM, type 2 diabetes mellitus; TCPM, Traditional Chinese patent medicine.
TCPM+LM versus LM
Twelve trials assessed the incidence of diabetes of TCPM+LM in comparison with LM alone. Meta-analysis showed that there was a significant difference found in favor of the combination group (n = 2008, RR 0.45; 95% CI 0.36–0.57, p < 0.00001; I2 = 0%).
TCPM+LM versus placebo+LM
Six trials assessed the incidence of diabetes of TCPM+LM in comparison with placebo+LM. Meta-analysis showed that there was a significant difference found in favor of the combination group (n = 1164, RR 0.54; 95% CI 0.42–0.69, p < 0.00001; I2 = 0%).
Adverse events
Adverse effects were reported in 12 trials, while the rest 6 included trials did not mention adverse events. In the 12 trials that reported adverse events, 8 trials reported that there were no adverse events, while 4 trials 15 –17,24 recorded the condition of adverse events, which are shown in Table 3. However, statistical analysis showed that no significant differences of adverse events were observed between two groups.
CI, confidence interval; LM, lifestyle modification; TCPM, Traditional Chinese patent medicine.
Secondary outcomes
Normalization of blood glucose
Results are shown in Figure 4.
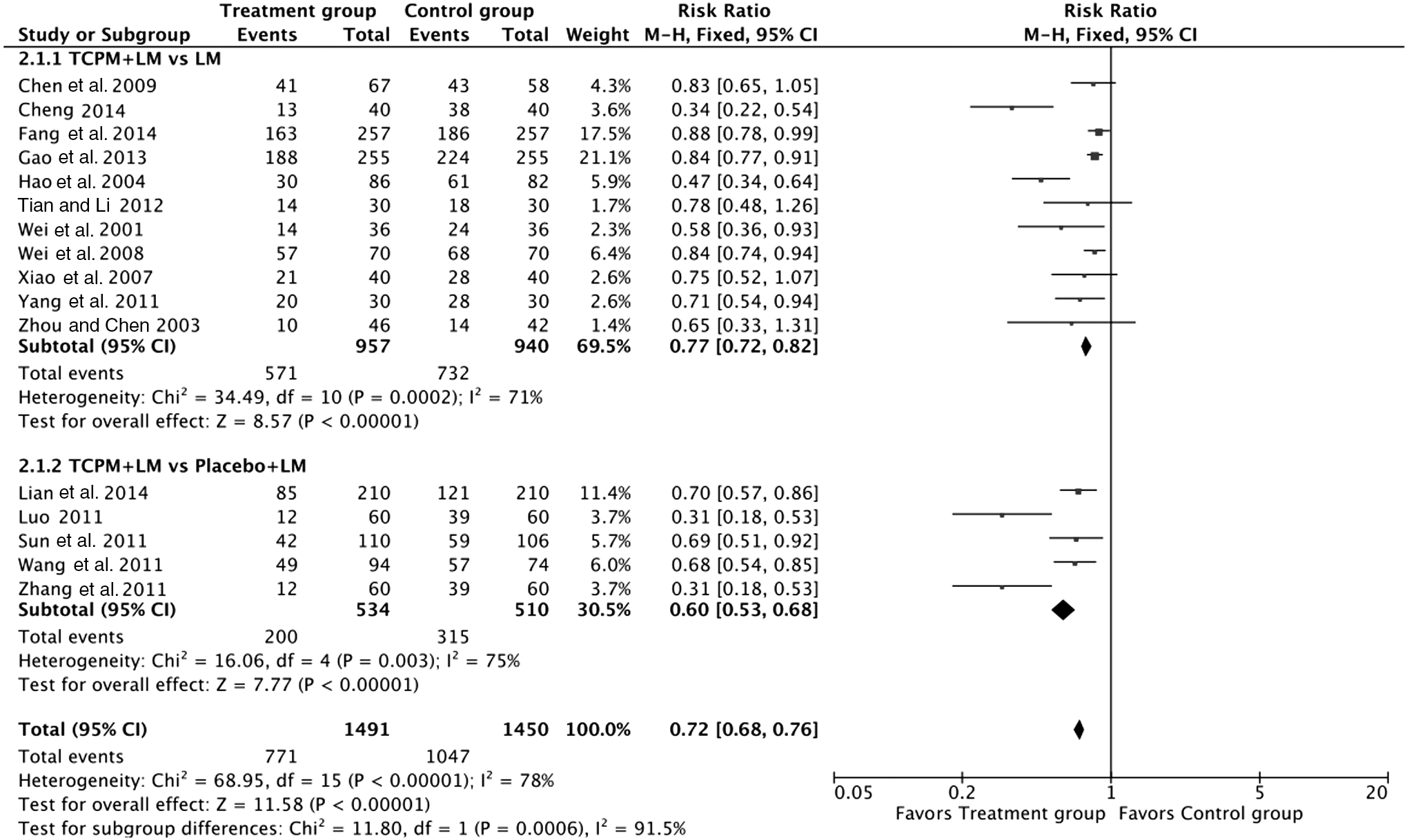
Blood glucose normalization comparison. CI, confidence interval; LM, lifestyle modification; TCPM, Traditional Chinese patent medicine.
TCPM+LM versus LM
Eleven trials reported the normalization of blood glucose; those receiving TCPM+LM combination were more likely to have normalized the blood glucose compared to those receiving LM only (n = 1897, RR 0.72; 95% CI 0.64–0.82, p < 0.00001; I2 = 71%).
TCPM+LM versus placebo+LM
Five trials reported the normalization of blood glucose. Meta-analysis displayed significant difference on normalization of blood glucose in favor of TCPM+LM group (n = 1044, RR 0.55; 95% CI 0.41–0.73, p < 0.0001; I2 = 75%).
Two-hour postprandial blood glucose
Results are shown in Figure 5.
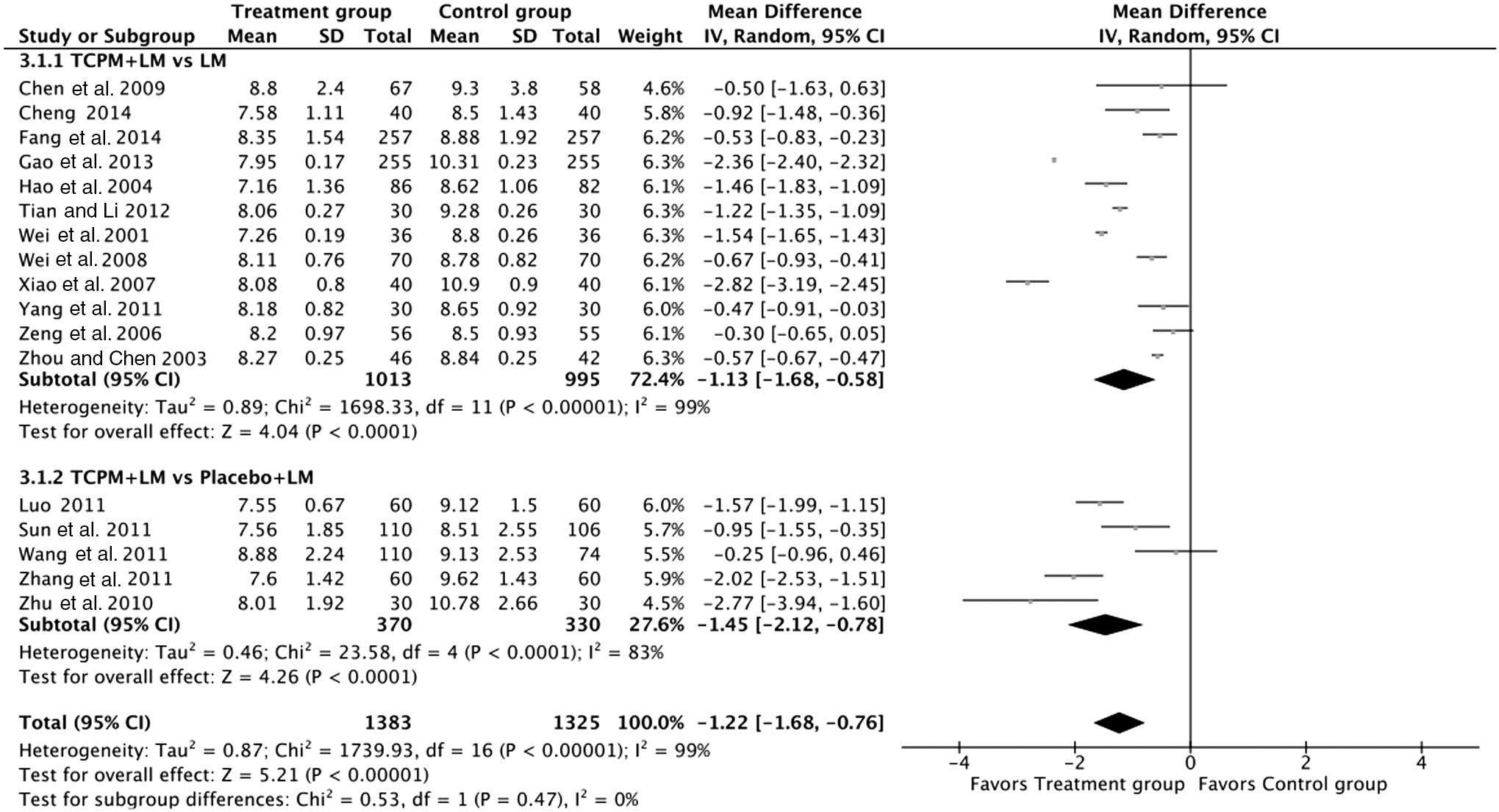
2hPG comparison. 2hPG, two-hour postprandial blood glucose; CI, confidence interval; LM, lifestyle modification; TCPM, Traditional Chinese patent medicine.
TCPM+LM versus LM
Twelve trials showed two-hour postprandial blood glucose (2hPG) as the outcome; the pooled analysis showed a statistically significant decrease in 2hPG with TCPM+LM compared to LM alone (n = 2008, MD −1.13; 95% CI −1.68 to −0.58, p < 0.0001; I2 = 99%).
TCPM+LM versus placebo+LM
In five trials, data for 2hPG variations were measured. Results showed that there was statistical difference between two groups for 2hPG level (n = 684, MD −1.45; 95% CI −2.11 to −0.79, p < 0.0001; I2 = 83%).
Body mass index
Results are shown in Figure 6.

BMI comparison. BMI, body mass index; CI, confidence interval; LM, lifestyle modification; TCPM, Traditional Chinese patent medicine.
TCPM+LM versus LM
There were eight trials comparing BMI of TCPM+LM (n = 764) with LM alone (n = 760). Meta-analysis demonstrated that participants treated with combination therapy decreased more significantly than participants receiving LM alone (MD −0.42; 95% CI −0.71 to −0.14, p = 0.004; I2 = 83%).
TCPM+LM versus placebo+LM
Five trials compared BMI of TCPM+LM with that of placebo+LM. Pooled results were statistically significant in favor of TCPM+LM combined therapy (n = 888, MD −1.12; 95% CI −2.00 to −0.24, p < 0.0001; I2 = 83%).
Fasting insulin, 2-h postprandial insulin, and HOMA-IR
Results are shown in Figures 7 –9.
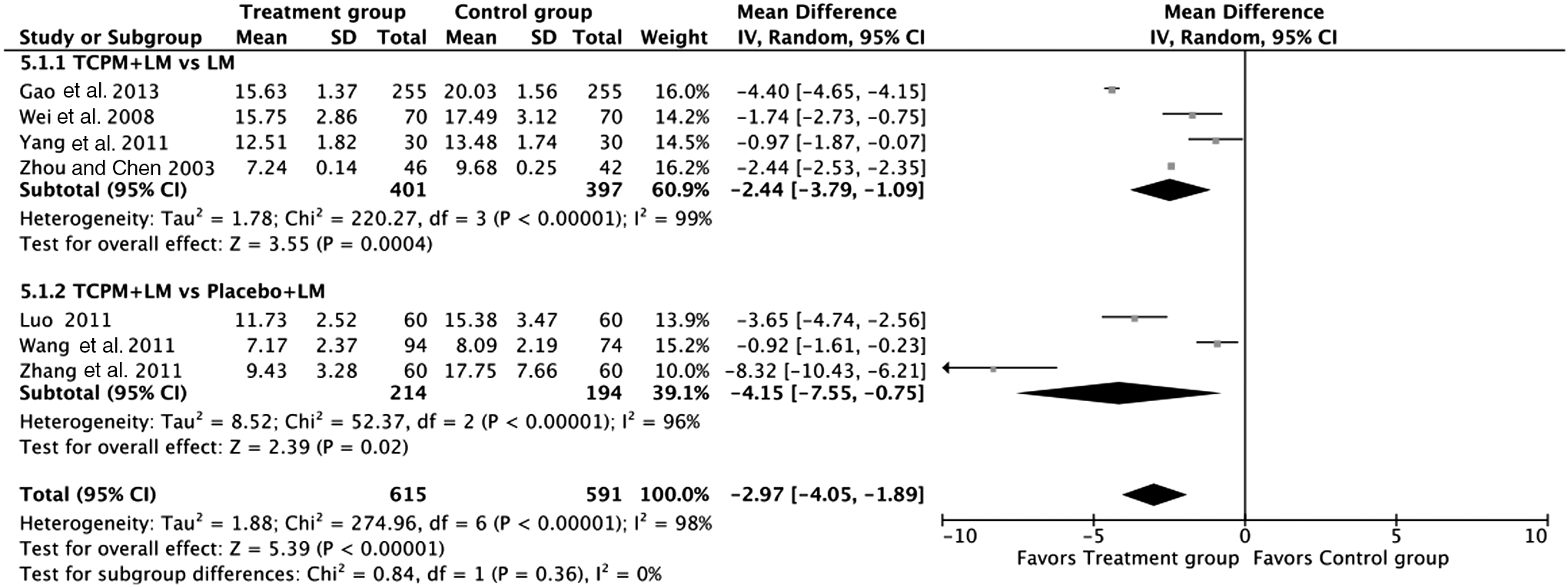
Fasting insulin comparison; CI, confidence interval; LM, lifestyle modification; TCPM, Traditional Chinese patent medicine.
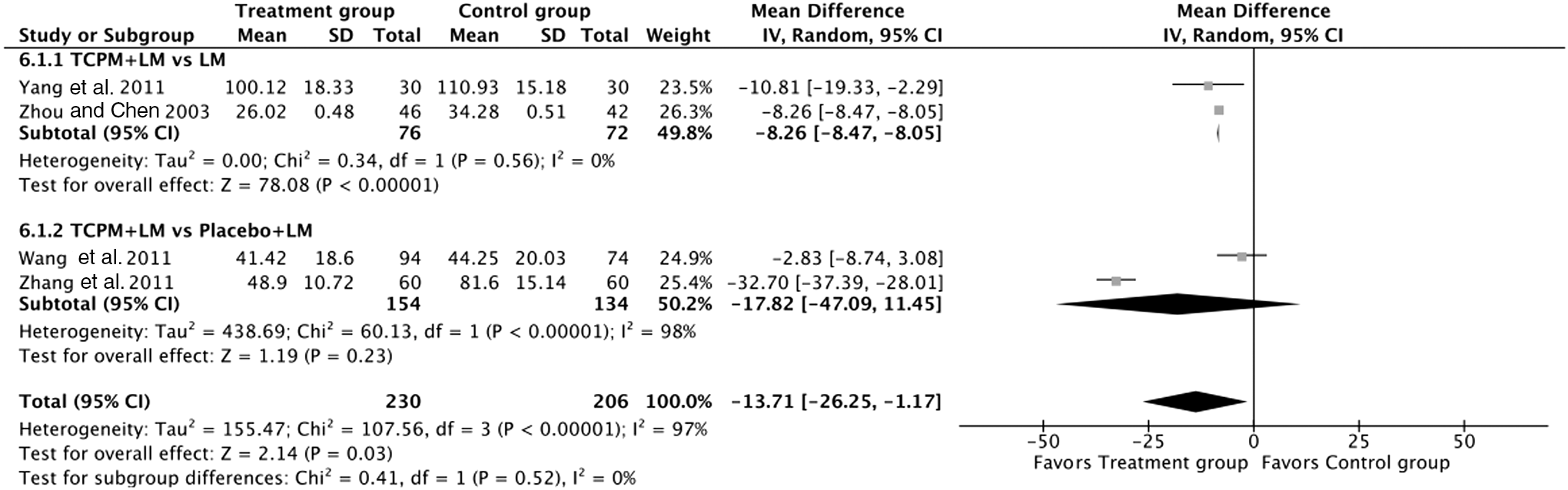
Two hours insulin comparison; CI, confidence interval; LM, lifestyle modification; TCPM, Traditional Chinese patent medicine.
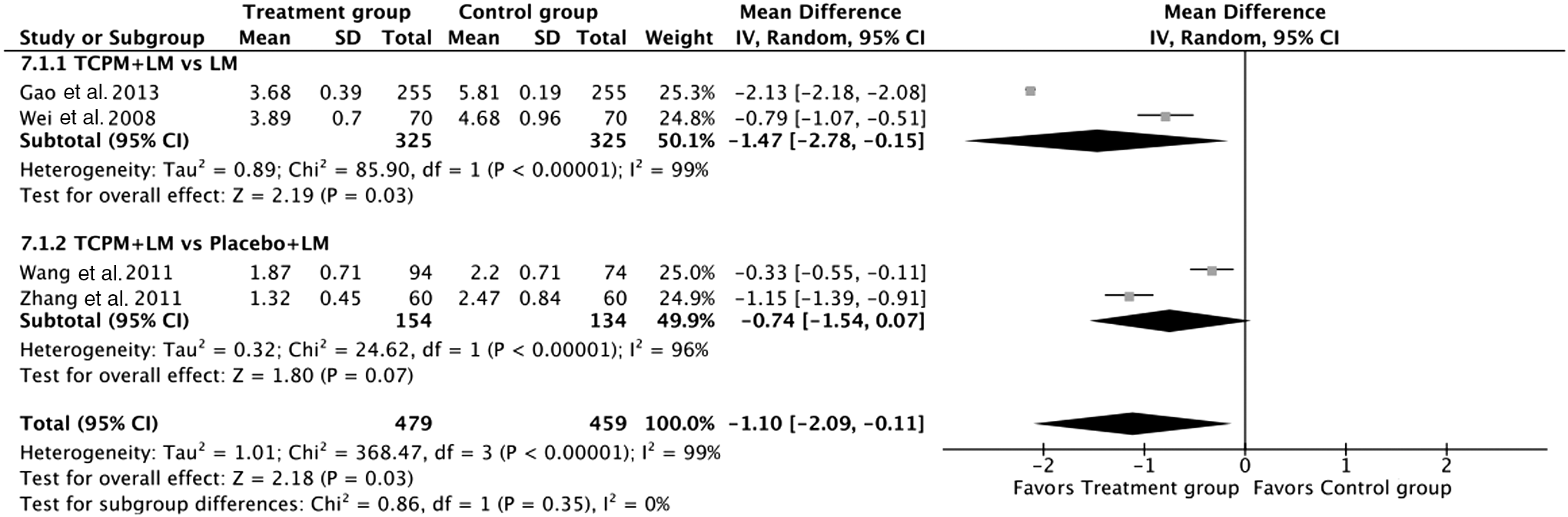
HOMA-IR comparison. HOMA-IR, homeostasis model assessment-insulin resistance; CI, confidence interval; LM, lifestyle modification; TCPM, Traditional Chinese patent medicine.
TCPM+LM versus LM
There were four trials comparing the effects of TCPM+LM on fasting insulin with LM alone. Pooled analysis indicated that fasting insulin in the treatment group had improved more significantly than control group (n = 798, MD −2.44; 95% CI −3.79 to −1.09, p = 0.0004; I2 = 99%). Two trials (n = 148) reported 2-h postprandial insulin of TCPM+LM with that of LM alone. There was significant difference on the improvement of 2-h postprandial insulin between two groups (MD −8.26; 95% CI −8.47 to −8.05, p < 0.00001; I2 = 0%). There were two trials evaluating the effect of TCPM+LM (n = 325) with LM (n = 325) alone on HOMA-IR. No statistical significance was observed on HOMA-IR between two groups (MD −1.47, 95% CI −2.78 to −0.15, p = 0.03; I2 = 99%).
TCPM+LM versus placebo+LM
There were three trials with records for fasting insulin, while two trials reported complete data for 2-h postprandial insulin and two trials for HOMA-IR. The pooled effects of fasting insulin, 2-h postprandial insulin, and HOMA-IR levels showed no significant differences between the treated and control groups (fasting insulin, MD −4.15; 95% CI −7.55 to −0.75, p = 0.02; I2 = 96%; 2-h postprandial insulin, MD −17.82; 95% CI −47.09 to 11.45, p = 0.23; I2 = 98%; HOMA-IR, MD −0.74; 95% CI −1.54 to 0.07, p = 0.07; I2 = 96%).
Sensitivity analysis and subgroup analysis
To investigate specific factors affecting the incident diabetes of RCTs, the authors performed sensitivity analysis and subgroup analysis on the follow-up duration, number of participants, publication year, diagnostic criteria, publication language, and type of TCPM. There were little differences (or much overlaps in CIs) in the overall RRs of incident diabetes (Table 4). All I2 values were <50%, and most groups were 0%, indicating a low heterogeneity. There was no significant difference (p > 0.05) in the overall RRs in all subgroup analysis.
The incidence of diabetes was analyzed according to different criteria based on follow-up duration, number of participants, publication year, diagnostic criteria, publication language, and type of TCPM. Z and p (effect) evaluated the statistics of overall effect; I2 and p (het) were computed to assess heterogeneity.
CI, confidence interval; RR, risk ratio; TCPM, Traditional Chinese patent medicine; WHO, World Health Organization.
Assessment of the quality of evidence
Appendix Tables A2 –A8 showed the summary of the overall evidence for each outcome by the GRADE method. Generally, quality of evidence was low for the incident diabetes, BMI, 2 h insulin, and HOMA-IR. In addition, the quality of evidence was very low for normalization of blood glucose, 2hPG, and fasting insulin.
Publication bias
The number of trials was too small to conduct any sufficient additional analysis of publication bias.
Discussion
IGT may fall under the TCM patterns of “spleen pyretic abundance.” The main pathogenesis lies in the damp-heat accumulation in the spleen and Spleen Qi deficiency in the body. Although the included TCPMs varied in their herbal components, the formulated prescriptions were based on the principle of “tonifying qi,” fortifying spleen, and clearing heat and form part of a “group” of herbal medicines with antihyperglycemic effects designed to prevent T2DM and to decrease blood glucose levels. In this systematic review, 18 trials involving 3172 participants were included. Patients who received TCPM plus LM were less likely to progress to T2DM compared with LM alone. Patients who received TCPM plus LM were also more likely to have their blood glucose levels return to normal compared with those who received LM alone. Compared with the control group, there was a decrease in 2hPG, BMI, and fasting insulin. Compared with placebo plus LM, TCPM plus LM was also superior in reducing diabetes and normalizing blood glucose; the interventions were also associated with a decline in the 2hPG levels and BMI levels. There were no significant differences in adverse events in either group. Similar findings were published to evaluate Chinese herbal medicine for prediabetes, 33 results showed that TCPM combined with LM could help to reduce the incident diabetes compared to LM alone. Strength of their review is that, first, the authors only aimed at IGT subjects in this systematic review, which account for 71% of prediabetes, 34 many clinical trials on prediabetes in China focus on IGT exclusively; second, the article above 33 only included the listed TCPMs, while the authors also focused on precompounded prescription order in this review, which covered broader researches and were consistent with the status of TCM clinical researches; and third, the authors focused on the islet function in this review, such as fasting insulin, 2 h insulin, and HOMA-IR, which are closely related to diabetes prevention. To investigate specific factors affecting the incident diabetes of RCTs, the authors performed subgroup analysis on the follow-up duration, number of participant, diagnostic criteria, publication language, and type of TCPM. Results indicated that a low heterogeneity existed; there was no significant difference (p > 0.05) in the overall RRs in all subgroup analysis. But the clinical effectiveness may be influenced by several factors, such as age, sex, body weight, course of diseases, syndrome, formulations and dosage of TCPM, course of treatment, and so on. The results of GRADE assessment were provided for all outcomes except for adverse events. The risk of bias in most of the included trials was high, which led to a reduced rating for the outcomes. Regarding inconsistency, a meta-analysis for the outcomes of normalization of blood glucose, 2hPG, BMI, fasting insulin, 2-h insulin, and HOMA-IR had high heterogeneity, so the ratings for these outcomes were reduced. As for indirectness, the aim of this review was to explore Traditional Chinese Medicine for IGT, and the authors choose some related indicators, so the authors did not include indirect comparisons. The authors also cannot find any imprecise evidence. For publication bias, significant asymmetry was detected in funnel plots for incidence of diabetes, the normalization of blood glucose, 2hPG, fasting insulin, 2-h insulin, and HOMA-IR, suggesting negligible publication bias. In conclusion, the evidence level for the outcomes was low regarding the incident diabetes, BMI, 2 h insulin, and HOMA-IR and very low for the normalization of blood glucose, 2hPG, and fasting insulin.
According to the literature, the lowering of BMI through dietary changes and increased physical exercise decreases the risk of diabetes among people with IGT by ∼50%. 15 The results showed that TCPM as an adjunct therapy could help decrease BMI level, which maybe the important mechanism to prevent diabetes. The overall interventions of TCPM+LM were associated with a decline in the BMI levels. Moreover, compared with LM alone, TCPM combined with LM showed significant advantages for improving 2-h blood glucose, BMI, and the level of insulin, which embody holistic regulation of TCM.
This systematic review provides preliminary evidence for the effectiveness and safety of TCPMs and has revealed that TCPMs combined with LM is an effective and safe therapeutic option used for the treatment of IGT, eventually preventing diabetes. A clinical recommendation cannot be warranted because of the generally low methodological quality of the included trials, which remained to be further determined by methodologically rigorous trials. Although the present evidence is insufficient to support the effectiveness of TCPM, it may warrant further study. Concerns regarding the methodological quality suggest that trials conducted by Lian et al., 15 Gao et al., 16 or Fang et al. 17 could be recommended.
In this review, the authors included 15 kinds of TCPMs; the most frequently used herbs were Huang Qi (Astragali Radix), Shan yao (Dioscoreae Rhizoma), Huang Lian (Rhizoma Coptidis), Gegen (Radix Puerariae), and Di huang (Radix Rehmanniae Glutinosae). Astragalus polysaccharides had an effect to two-dimensionally regulate the level of blood glucose, which could increase the blood glucose of hypoglycemic humans or animals to normal level, and significantly lower the level of blood glucose and triglyceride and improve the metabolism of diabetic rats. 35 The main active ingredient of Rhizoma Coptidis (berberine) can effectively reduce blood glucose, lower lipids, as well as function as antioxidant. Lee et al. 36 demonstrated that berberine upregulated adenosine monophosphate (AMP)-activated protein kinase (AMPK), which resulted in improvement of insulin resistance and promotion of glycolysis. Zhen et al. 37 showed that Rhizoma Coptidis is the key ingredient in a herbal decoction, which rectifies insulin resistance through activation of AMPK enzyme. Puerarin can effectively reduce the blood glucose and body weight and improve insulin resistance among rats with the high fat diet-induced insulin resistance, suggesting the potential role of puerarin in the prevention of T2DM. 38,39
Several limitations are worthy to be mentioned. First, some heterogeneity was found; therefore, making comparisons difficult to be fully reliable and to be taken with caution. Although all included studies examined only IGT patients, there was also some heterogeneity in different ingredients, formulations or dosage of TCPM group, or different follow-up duration across studies, which make conclusions hard to stand. Second, only 18 RCTs were included in their review, and the meta-analysis was performed irrespective of the studies' methodological quality, so it is possible that the statistical power may not have been adequate due to the small number of studies. Third, long-term effectiveness of TCPM on prevention of diabetes in people with IGT is not known, and the authors have no data regarding improvements in diabetes after treatments. Hence the pooled results should be treated with caution.
Conclusion
Preliminary evidence showed that TCPM combined with moderate LM may have significant effect on IGT; they could significantly lower the 2hPG, BMI, fasting insulin, and 2 h insulin. Despite the apparently positive findings, it is premature to conclude the effectiveness of TCPMs for the treatment of IGT due to the high heterogeneity of the included trials and the generally low methodological quality of the included trials. Double-blinded placebo-controlled RCTs are required to provide stronger evidence.
Footnotes
Acknowledgment
This study is supported by the Major Program of the National Natural Science Foundation of China (Grant No. 81430097).
Authors' Contributions
B.P. and Q.N. conceived the study and wrote the article; the two of them contributed equally to this work and are both first co-authors; Y.-Q.L. and Y.-T.W. did the data collection; Y.-J.Z. and X.-M.Z. accessed the risk of bias of references; B.P. and S.F. performed the statistical analysis; and X.-L.T. and Q.N. participated in the design of the study and coordination.
Author Disclosure Statement
No competing financial interests exist.
| Summary of findings | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Quality assessment | Study event rates (%) | Anticipated absolute effects | |||||||||
| Participants (studies) follow-up | Risk of bias | Inconsistency | Indirectness | Imprecision | Publication bias | Overall quality of evidence | With control | With HOMA-IR comparison between treatment group and control group | Relative effect (95% CI) | Risk with control | Risk difference with HOMA-IR comparison between treatment group and control group (95% CI) |
| Treatment group vs. control group (important outcome; better indicated by lower values) | |||||||||||
| 938 (4 Studies) 6 months | Serious a | No serious inconsistency | No serious indirectness | No serious imprecision | Reporting bias strongly suspected b | ⊕⊕⊖⊖ Low a,b due to risk of bias, publication bias | 459 | 479 | — | The mean treatment group vs. control group in the intervention groups was 1.1 lower (2.09–0.11 lower) | |
| Treatment group vs. control group—TCPM+LM vs. LM (important outcome; better indicated by lower values) | |||||||||||
| 650 (2 Studies) 6 months | Serious a | Serious c | No serious indirectness | No serious imprecision | Reporting bias strongly suspected b | ⊕⊖⊖⊖ Very low a –c due to risk of bias, inconsistency, publication bias | 325 | 325 | — | The mean treatment group vs. control group—TCPM+LM vs. LM in the intervention groups was 1.47 lower (2.78–0.15 lower) | |
| Treatment group vs. control group—TCPM+LM vs. placebo+LM (important outcome; better indicated by lower values) | |||||||||||
| 288 (2 Studies) 6 months | Serious a | Serious c | No serious indirectness | No serious imprecision | Reporting bias strongly suspected b | ⊕⊖⊖⊖ Very low a –c due to risk of bias, inconsistency, publication bias | 134 | 154 | — | The mean treatment group vs. control group—TCPM+LM vs. placebo+LM in the intervention groups was 0.74 lower (1.54 lower to 0.07 higher) | |
Chinese patent medicine for impaired glucose tolerance (IGT).
Most of the trials were included as the high risk of bias.
The authors detected the significant asymmetry according to the funnel plot, suggesting a negligible publication bias.
Meta-analysis for the outcome had high heterogeneity.
CI, confidence interval; HOMA-IR, homeostasis model assessment-insulin resistance; LM, lifestyle modification; TCPM, Traditional Chinese patent medicine.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.