
Abstract

Dear Editor:
S
The human body has evolved an ability to maintain homeostasis in response to the external environment. The ability to recognize pain was selected to cope with harmful stimuli and their subsequent sequelae. Pain is categorized into two types: escapable pain and inescapable pain. 2 The former leads to a stinging superficial sensation originating from the skin and is usually caused by animal bites or thorns on plants and trees. In response to this type of pain, the body adopts a fight or flight-coping strategy to maintain homeostasis by avoiding or eliminating the cause of pain. The latter is a deeper and duller pain originating from muscles, joints, or viscera, and is caused by injuries, intake of rotten foods, or infection. Since this type of pain cannot be avoided or removed, the body adopts a sickness behavior—coping strategy, which saves and reallocates energy until the harmful stimuli are removed. This response may occur in the form of motor quiescence, hyporeactivity, decreased vigilance, reduced responsiveness to tactile or visual stimuli, sympathoinhibition, or vasodepression. 2
The specific coping strategies adopted in response to pain is determined by the periaqueductal gray (PAG), which is located in the midbrain. Superficial pain activates the lateral and dorsolateral PAG column through A-delta-fiber to trigger a fight or flight response. Deep pain activates the ventrolateral PAG column through C-fibers to trigger sickness behavior. Once the PAG is activated by pain, it tends to lower the intensity of pain through negative feedback of the descending pain control system, resulting in opioid-dependent analgesia. Interestingly, this negative feedback system in the PAG acts only on C-fibers, but not on A-delta-fibers. 3 This may be due to evolutionary reasons, as the excessive sickness due to continuation of inescapable pain through C-fibers is unfavorable for survival. Meanwhile, inhibition of the A-delta-fiber response to repeated escapable pain may be accompanied by the risk of survival against avoidable but dangerous causes.
Acupuncture treatment comprises a mixture of two steps consisting of the penetration of the skin and muscle stimulation, which is usually called de qi. This process excites both the A-delta-fibers from the skin and the C-fibers from muscle. The activated PAG then suppresses C-fiber activity in a negative feedback manner and results in a reduction in inescapable pain. 4 This hypothesis may explain how acupuncture therapy is able to reduce inescapable pain from the muscles, joints, or viscera, and improve sickness behavior, such as fatigue, depression, lack of appetite, or indigestion. Our proposal is supported by extensive research evidence indicating that de qi during acupuncture therapy, which is the process of enhancing muscle stimulation, is a critical factor for positive outcomes in clinical pain control. 5 Our assumed theory for mechanism of pain control by acupuncture is summarized in Figure 1.
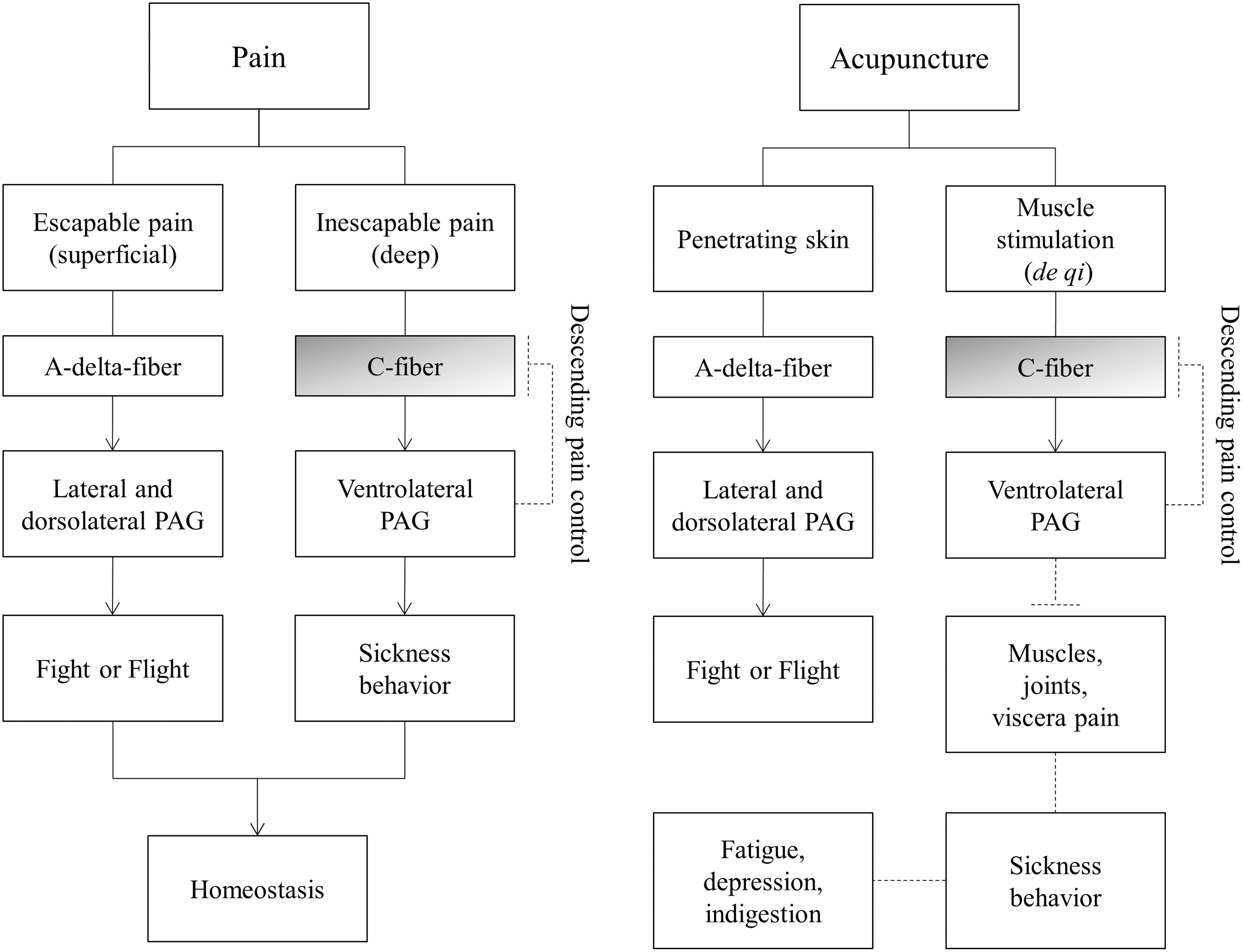
An evolutionary approach to the mechanism of pain control by acupuncture therapy. PAG, periaqueductal gray.
The mentioned observations indicate that acupuncture is a valuable treatment modality that can effectively modulate the pain control system that has evolved over time in humans. This evolutionary approach helps us to explore the mechanisms of acupuncture therapy, which warrant extensive research using scientific study models.
Footnotes
Acknowledgment
This research was supported by the grant of the Traditional Korean Medicine R&D Project, Ministry of Health & Welfare, South Korea (HI15C0112).
Author Disclosure Statement
No competing financial interests exist.