
Abstract
Objectives:
In Iranian folklore medicine, boiled extract of Stachys lavandulifolia Vahl is reputed to have therapeutic effects in painful disorders. This study evaluated the efficacy of the standardized formulation of S. lavandulifolia Vahl in reducing pain in primary dysmenorrhea, which is known to be a common disorder with significant impact on quality of life.
Design:
A randomized, double blind, crossover, placebo-controlled pilot study.
Settings/Location:
Bu-Ali Hospital affiliated with Tehran Medical Branch, Islamic Azad University.
Subjects:
Twenty-nine patients with primary dysmenorrhea. Patients were enrolled according to medical history and gynecologic sonography.
Interventions:
Standardized capsules of S. lavandulifolia were prepared. All the patients were allowed to take mefenamic acid up to 250 mg/q6h if they needed, in the first menstruation cycle to estimate the analgesic consumption at baseline. By the use of an add-on design in the next cycle, they were randomly assigned to receive either herbal or placebo capsules every 4–6 h. Then, they were crossed over to the other group during the course of the trial.
Outcome measures:
At the end of the fourth day of each cycle, the intensity of pain was measured by visual analogue scale and McGill pain questionnaire. Statistical significance was evaluated using repeated-measures one-way analysis of variance.
Results:
Pain intensity was significantly decreased during consumption of Stachys lavandulifolia capsules in comparison with basic and placebo cycles (p < 0.05). Interestingly, the consumption of mefenamic acid capsules was reduced dramatically in the S. lavandulifolia cycle in comparison with basic and placebo cycles (p < 0.001).
Conclusions:
It was demonstrated that S. lavandulifolia-prepared formulation can reduce menstrual pain, and can probably be recommended as an add-on therapy or even an alternative remedy to nonsteroidal anti-inflammatory drugs (NSAIDs) with fewer side effects in primary dysmenorrhea.
Introduction
D
Approximately, 10%–15% of absences in high school students are due to primary dysmenorrhea. 4 It has been estimated that 50% of girls after menarche suffer from primary dysmenorrhea and 10% have severe pain that leads to disability with 1–3 days per month frequency. 5 Multiple factors play a role in the pathophysiology of the disease. Increased secretion of prostaglandin by endometrium during menstrual cycles is the most common cause. 6 Moreover, vasopressin plays a crucial role in the myometrial activity, which is accompanied with uterine ischemia and pain. 7 With regard to pathology, prostaglandin inhibitors such as nonsteroidal anti-inflammatory drugs (NSAIDs) like mefenamic acid ibuprofen, can alleviate symptoms of dysmenorrhea. 8
Traditional medicines such as herbal remedies still play an important role in management of diseases such as dysmenorrhea in Asia and Europe. The genus of Stachys belongs to labiatae family, which contains about 270 distinct species in the world. 9 In Iran, 34 species of Stachys-like lavandulifolia (Common name: Chai Koohi) exist as native plants. 10 Based on Iranian traditional medicine, boiled extract of Stachys lavandulifolia Vahl aerial parts is effective in painful disorders. 11 It is also known as an antitoxic, 12 antibacterial, 13 and antinephritis remedy. 14 Furthermore, anxiolytic, 15 analgesic, and anti-inflammatory properties 16,17 of S. lavandulifolia have been reported. Pervious phytochemical analysis of S. lavandulifolia has identified flavonoids, saponins, iridoids, phenyl ethanoids, and diterpenoid in this plant. 18,19 Despite the traditional use of S. lavandulifolia Vahl and its wide growth in Iran, 20 the efficacy of S. lavandulifolia Vahl in abdominal pain and dysmenorrhea has not been clinically elucidated. The aim of this study was to evaluate the therapeutic effects of standardized formulation of S. lavandulifolia Vahl on primary dysmenorrhea. To authors' knowledge, to date, therapeutic effects of any formulation of S. lavandulifolia Vahl on pain management in primary dysmenorrhea have not been investigated in any clinical trial.
Material and Method
Preparation of the plant material
Aerial parts of S. lavandulifolia Vahl were collected from the Alamut region in Qazvin province, located in central part of Iran, in January 2014 (E 50 ° 35′13/92″, N 36°26′340/08″, altitude 2060 m), under the supervision of Islamic Azad University, Pharmaceutical Sciences Branch, Pharmacognosy department. Since the region was neither a protected area nor a private property, no specific permission was required for entering the location. It is also confirmed that this study did not involve endangered or protected species.
The plant was identified by Professor Gholamreza Amin, from botany department of Faculty of Pharmacy, Tehran University of Medical Science (TUMS), Tehran, Iran. Furthermore, a voucher specimen was deposited in the herbarium of the pharmacy faculty (herbarium number: 6695).
Aerial parts of S. lavandulifolia were dried in the shade at room temperature. The hydroalcoholic extract was obtained by percolation method. Powdered aerial parts of the plant (340 g) were macerated with 2500 mL of ethanol (Bidestan Co.) and distilled water (8:2) at room temperature for 5 days. The extract was filtered and concentrated under vacuum in a rotary evaporator IKA*RV10® (45°C). The yield percentage of the extract was 10%.
Determination of safety doses
Acute and subchronic toxicity study of S. lavandulifolia Vahl have been conducted on mice and its safety is confirmed at doses up to five times greater than maximum consumption doses in this study. 21
This study was approved by the ethics committee of Islamic Azad University, Pharmaceutical Science Branch (IAUPS) with the registration number of 4113. It was also registered in Iranian Clinical Trials Center affiliated with Ministry of Health and Medical Education (Registration Number: IRCT138904133106N2).
Preparation of standardized formulation
The herb used in this trial is available over the counter as a traditional remedy throughout Iran. Capsule dosage form was selected for masking the intensely herbal taste to promote the compliance of the patients. Each capsule contained 100 mg of extract. The excipients were of quantified constituents per capsule as follows: microcrystalline cellulose (Avicel PH102) 350 mg and magnesium stearate about 5 mg (1%) per capsule.
Essential oil of the plant as well as essential oil of hydroalcoholic extract were extracted by hydrodistillation in Clevenger-type apparatus and steam distillation (EOV2000) for a 3-h period, in accordance with the British Pharmacopoeia recommended method. To determine the suitable compound for standardization, all extracted essential oils were elucidated by GC/MASS (Hewlett-Packard 5973) analysis with capillary column HP-5MS Agilent (30 m × 0.25 mm, film thickness 0.25 μm).
Thymol was selected for standardization due to its spasmolytic effects. The amount of thymol per capsule was 0.15 mg as the effective dose of thymol to produce spasmolytic activity has been reported as 1 μM in guinea pig which is equal to 0.15 mg. However, no human data were available. 22 Control and stability tests such as assay, content uniformity, and dissolution were conducted using gas chromatography with flame-ionization detection (GC-FID), a general detector for organic compounds in GC, (CP-3800 Varian) according to the mentioned method in British Pharmacopoeia. Thymol standard (Gyan Flavours) was used to obtain the calibration curve. Stability tests were done at accelerated temperature and humidity conditions, according to the ICH guidelines (40°C ± 2°C and 70% ± 5% humidity). Samples were analyzed after first, second, third, and sixth month of storage at accelerated conditions of temperature and humidity. Furthermore, other tests such as loss on drying, disintegration time, brittleness, and the average of the weight of content, and microbial control tests were conducted. Quantification of thymol was done using GC/FID by an expert, at Jaber Ebne Hayyan pharmaceutical Company, according to the British Pharmacopoeia; this method is described in Appendix 1A of British Pharmacopoeia. The placebo capsules used in this study were identically sized capsules filled with microcrystalline cellulose (Avicel PH102). Moreover, since the capsules were semiclear, food-grade color was added to placebo powder.
Clinical trial
Patients were recruited from obstetrics and gynecology ward in Bu-Ali teaching hospital affiliated with Islamic Azad University, Tehran Medical Branch (IAUTMU), and enrolled in a randomized, double-blind, crossover, placebo-controlled pilot study for 3 months. Patients were assessed according to medical history and gynecologic sonography, which are the established standards for diagnosis of primary dysmenorrhea, 23 by a professor of obstetrics and gynecology, who enrolled the patients as well. Due to the design of a pilot and crossover study, a number of 40 participants were suggested. Since the study was crossover in design, it allowed for a smaller sample size collection. Sample size selection was done according to previous studies. 24 –26 Figure 1 summarizes the study procedure.
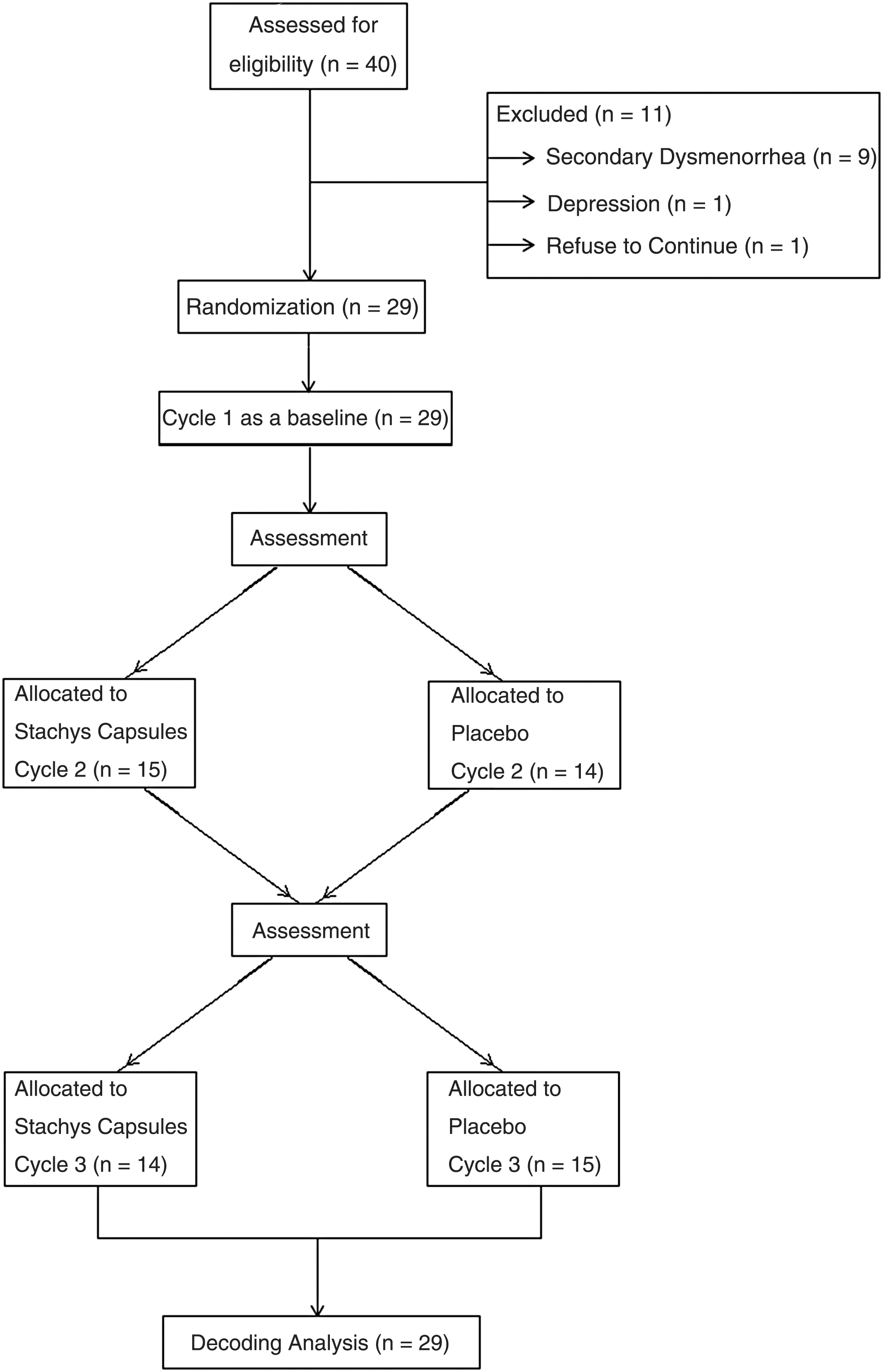
Enrolment and follow-up procedure of the study participants.
Inclusion criteria were as follows: age between 18 and 45 years, regular menstrual cycles, diagnosis of primary dysmenorrhea, and existence of dysmenorrhea indicated by average of visual analogue scale (VAS) ≥6 in the last three cycles (Table 2). Any drug consumption was an exclusion criterion in this study. No concomitant medication was used in both groups. Exclusion criteria were pregnancy, lactation, abnormal vaginal bleeding, moderate to severe menorrhagia, body mass index (BMI) more than 30, and oral contraceptive or any hormone consumption.
After a complete description of the study, an informed written consent was obtained from all participants before entering the trial. It was indicated that they can withdraw from the study at any time without any obligation for justification. The 10-step VAS and McGill pain questionnaire were used to assess change in pain during the menstruation cycles. In VAS, zero means no pain and 10 means the worst experienced pain. The McGill pain questionnaire consists of intensity scale as 0 = none, 1 = mild, 2 = moderate, and 3 = severe related to each kind of pain (shooting, stabbing, sharp, cramping gnawing, hot-burning, aching, heavy, tender, splitting, tiring-exhausting, sickening, fearful, and punishing-cruel). The primary outcome measures analgesic effect, including drop in VAS and McGill pain questionnaire scores.
Randomization was done by a sequence of recruitment, which means the first patient was assigned to one group by tossing a coin and the next patient was assigned to another group by an independent third party. As it was not ethical to deprive patients of routine analgesic use, we decided to focus on the quantity of analgesic (mefenamic acid) use as a secondary outcome measurement. Any decrease in analgesic use may indicate effect size of the treatment. Before the intervention, as a basic cycle, all patients were allowed to take mefenamic acid up to 250 mg/q6h, if they needed, for the first menstruation cycle.
By the use of an add-on design in the next cycle, they were randomly assigned to receive either the herbal preparation or placebo every 4–6 h. Then, patients were crossed over to the other group (Fig. 1). This dosage regimen was determined by converting the traditional medical data with acceptable estimation. The patients were followed up for 3 months after treatment.
Herbal and placebo capsules were identical in shape, color, and weight. Duration of treatments was 4 days, 1 day before the onset of menstruation and 3 days after the onset of menstruation, for three consecutive menstrual cycles, as recording the analgesic consumption in basic cycle showed that some patients started to take mefenamic acid 1 day before the onset of the cycle for the purpose of pain prophylaxis. Participants reported no use of mefenamic acid in the fourth day of menstruation cycle.
Herbal and placebo capsules were coded before the initiation of the study by the third party and were not decoded until the end of the study. Thus, neither the patients nor the examiner knew the herbal formulation or placebo until the termination of statistical analysis. In all cycles, patients were allowed to take mefenamic acid capsules if they had uncontrolled pain. At the end of the fourth day of each cycle, the intensity of pain was measured by the 10-step VAS and McGill pain questionnaire.
Statistical analysis
Data analyses were performed and plotted using GraphPad Prism (version 4.03; GraphPad Software, Inc., San Diego, CA). Statistical significance between the control and tested groups was evaluated with repeated-measures one-way analysis of variance with Bonferroni multicomparison post-test. *p < 0.05, **p < 0.01, ***p < 0.001, and ****p < 0.0001 indicate statistically significant difference between the control and tested groups. Furthermore, the improvement rate, the consumption of mefenamic acid capsules, and probable side effects of herbal treatment were evaluated
Results
Electron impact mass spectra of thymol in the essential oil of the plant and the extract are shown in Figure 2. Control tests used for stability of the prepared capsules are summarized in Table 1. Accelerated stability assessments were shown to be compliant over 6 months.
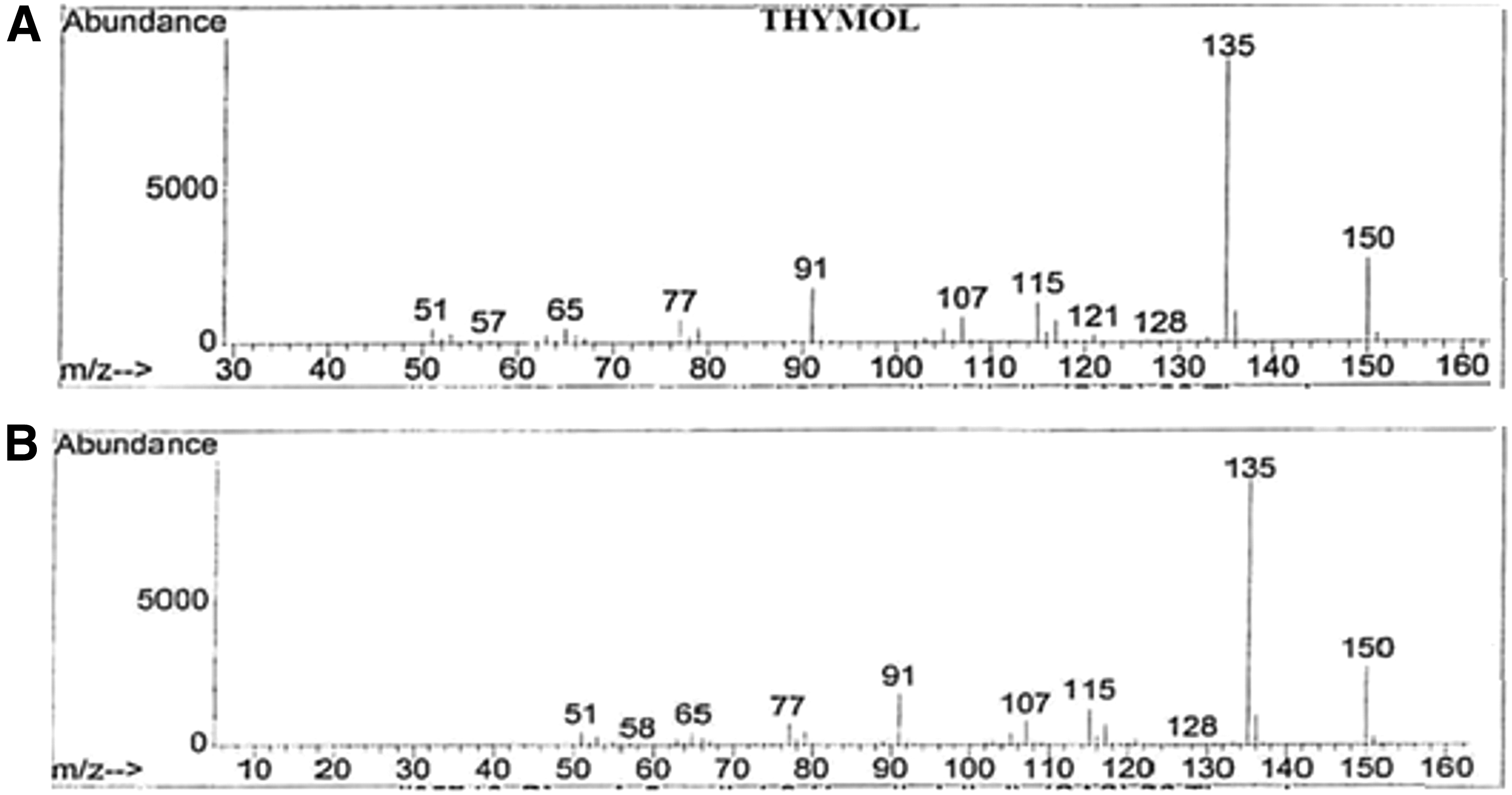
Electron impact mass spectra of thymol in the essential oil obtained from the plant
Eleven patients who were diagnosed with secondary dysmenorrhea consumed antidepressant drugs and refused to continue the study were excluded. After patient screening, 29 patients were enrolled and completed the study. Demographic information of the patients is shown in Table 2. The majority of the patients were single and only three of them were married. At the beginning of the study, there were no significant differences between the groups in Stachys and placebo cycles regarding age, cycle duration, duration of menstrual flow, height, weight, and BMI (p > 0.05).
BMI, body mass index; VAS, visual analogue scale.
S. lavandulifolia capsules suppressed significantly the average of menstrual pain intensity measured by VAS to 5.29 in comparison with the basic (mean = 6.4, p < 0.05) and placebo cycles (mean = 7.07, p < 0.001). Measuring of the menstrual pain by McGill pain questionnaire showed the similar decreasing trend of pain by taking herbal capsules (12.48) compared to the basic (mean = 14.25, p < 0.05) and placebo cycles (mean = 15, p < 0.01) (Figs. 3 and 4).
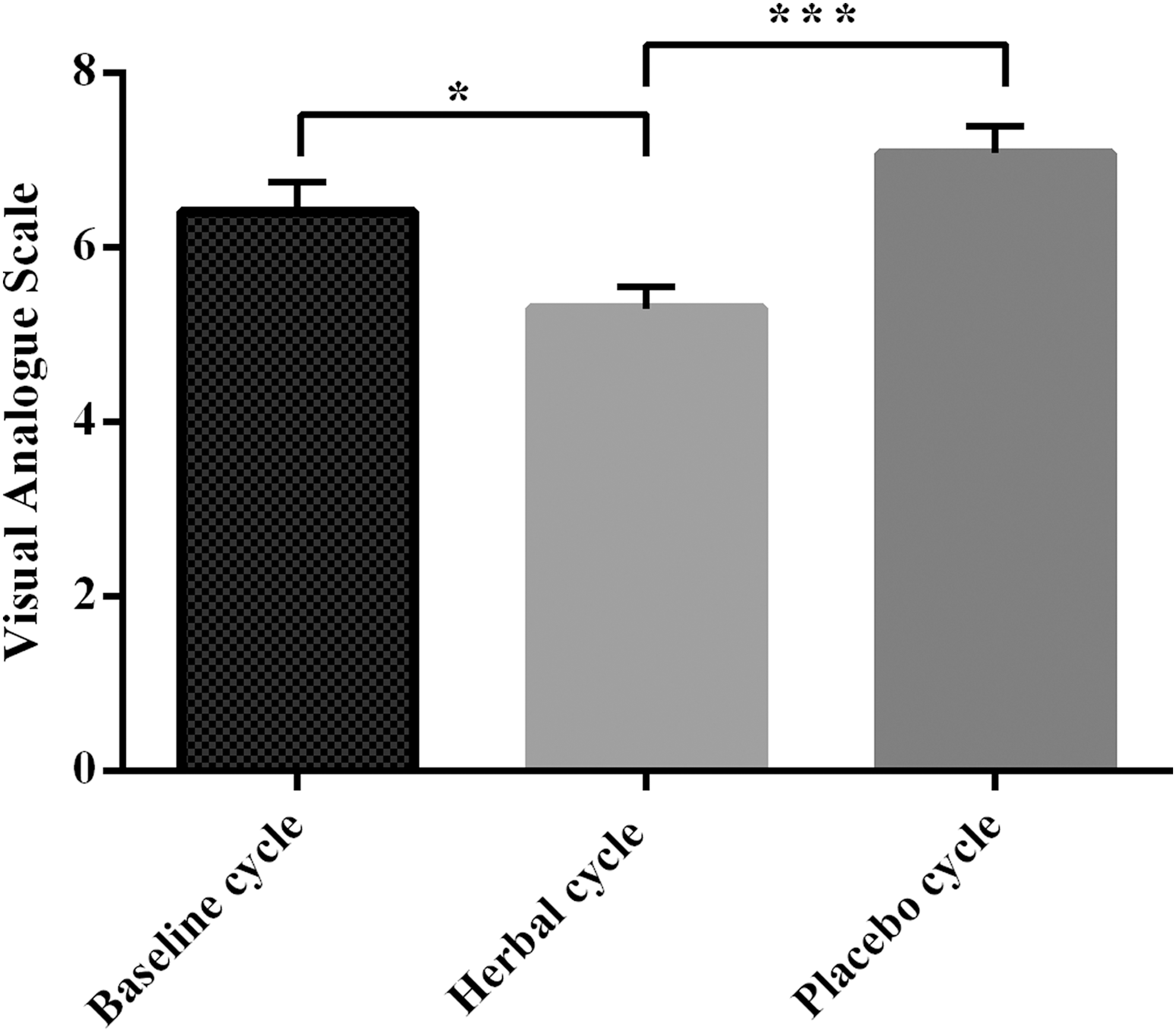
Comparison of pain intensity by visual analogue scale during three consecutive menstruation cycles. Repeated-measures one-way analysis of variance (ANOVA) analyses revealed that the pain intensity was significantly lower in the cycle of the herbal capsule compared to the baseline (*p < 0.05) and placebo cycles (***p < 0.001).
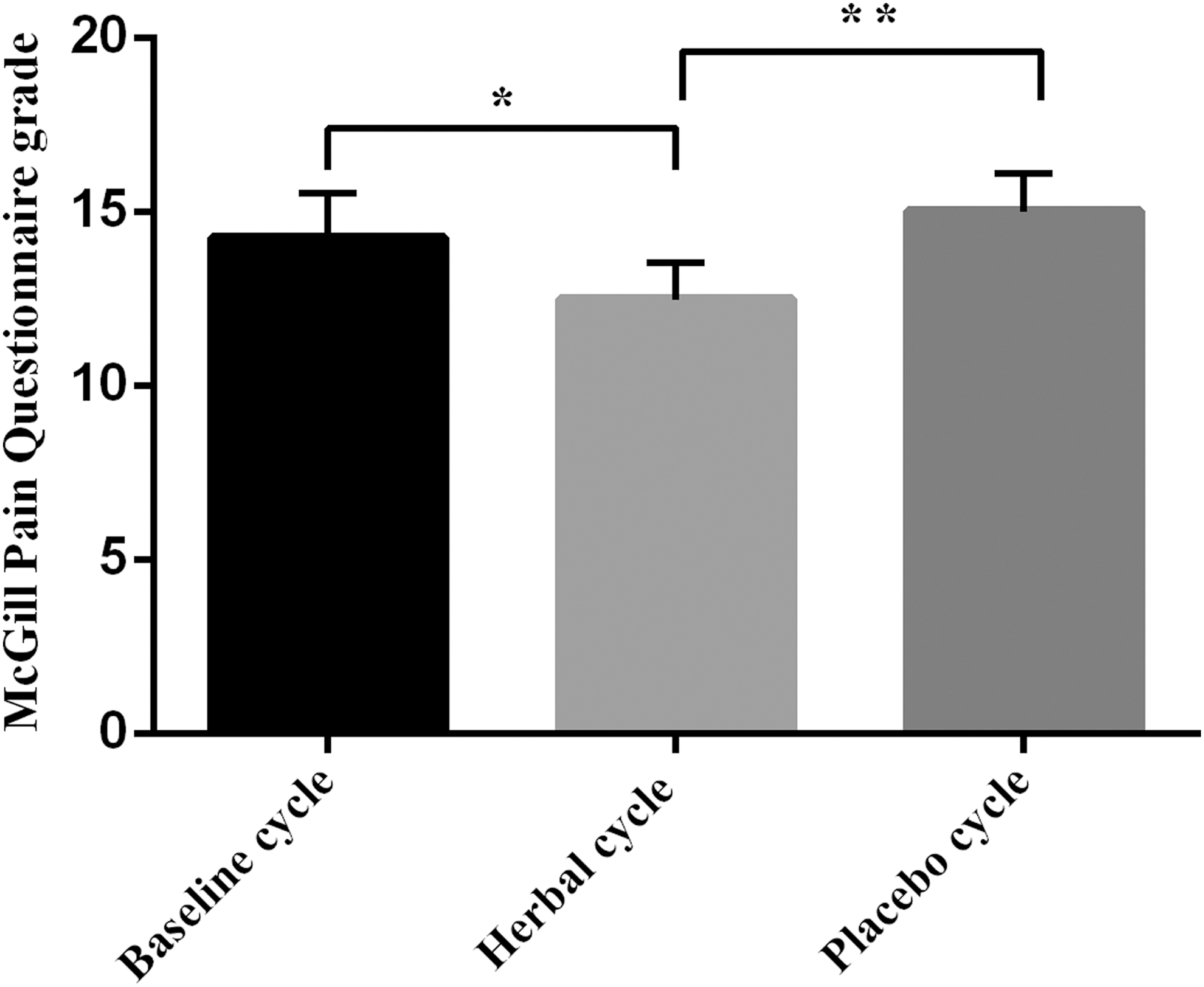
Comparison of pain intensity by McGill Pain Questionnaire during three consecutive menstruation cycles. Pain intensity suppressed significantly in herbal cycle in comparison with baseline and placebo cycles (repeated-measures one-way ANOVA (*p < 0.05) and (**p < 0.01), respectively).
The mean number of the consumed mefenamic acid capsules was compared across the three cycles. The consumption of mefenamic acid capsules decreased dramatically in the cycle that patients received S. lavandulifolia capsules to 1.59 compared to the basic (mean = 4.88, p < 0.0001) and placebo cycles (mean = 4.03, p < 0.001) (Fig. 5). Summary of the figures is shown in Table 3. It is noticeable that in ∼40% of the patients during this cycle, the pain was completely controlled by the prepared herbal capsules and there was no need to take mefenamic acid at all.
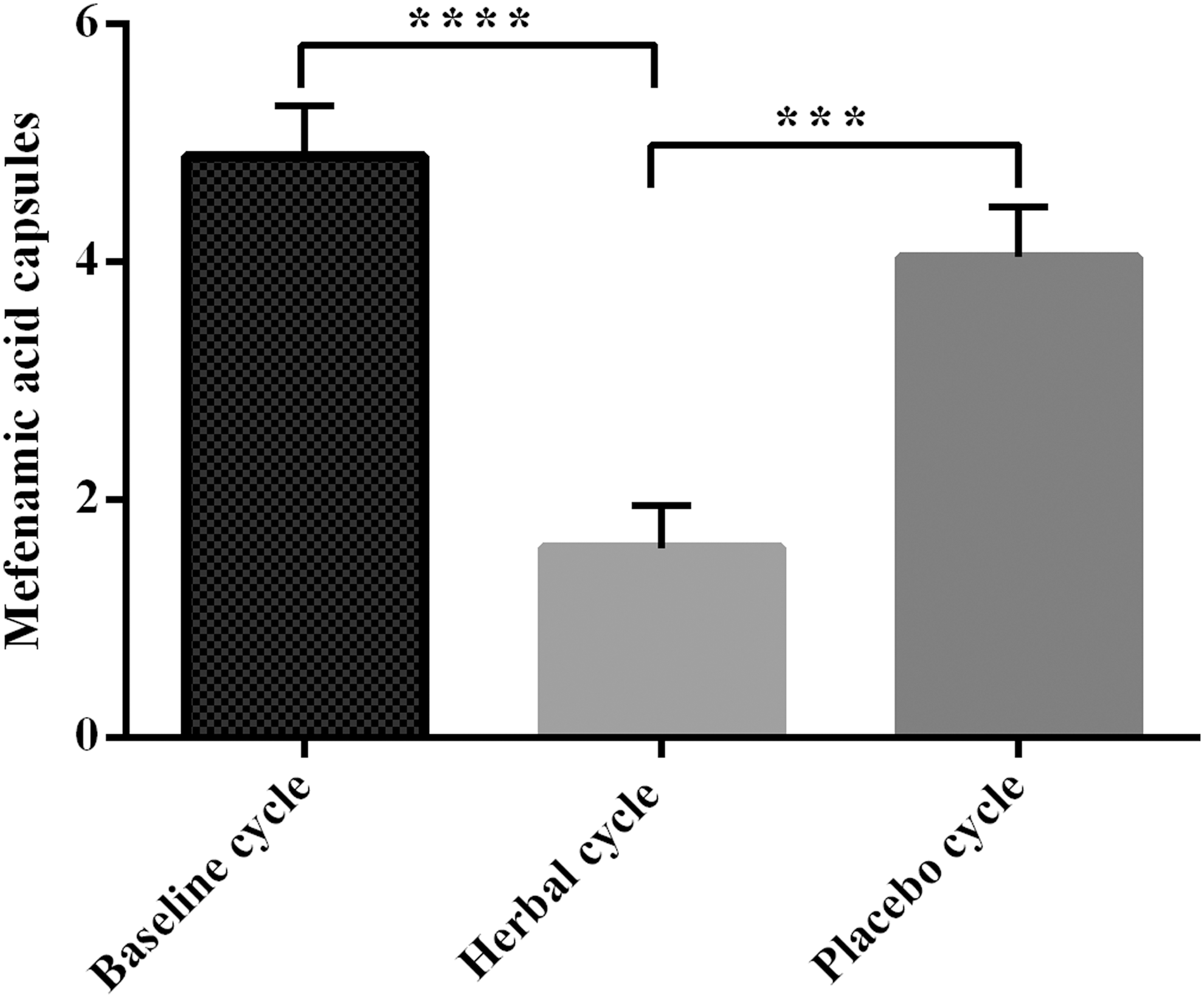
Comparison of the number of mefenamic acid capsules taken during three consecutive menstruation cycles. Repeated-measures one-way ANOVA analyses showed a potent analgesic effect of the herbal capsule and decrease in consumption of mefenamic acid in herbal cycle compared to baseline (****p < 0.0001) and placebo cycles (***p < 0.001).
Values are given as mean ± SE.
p < 0.05, indicates statistically significant difference. (a) Herbal treatment compared to basic cycle. (b) Herbal cycle compared to placebo cycle.
VAS, visual analogue scale.
Discussion
According to our knowledge, this study is the first clinical trial on the therapeutic effects of standardized formulation of S. lavandulifolia Vahl on primary dysmenorrhea. Previous studies on this plant have demonstrated the presence of glycosides such as iridoids, flavonoids, and phenyl ethanoides in this plant. 18 as well as thymol. 22 In addition, several studies confirmed the ability of some of these compounds to inhibit prostaglandin synthesis by cyclooxygenase 1 and 2 inhibition. 27,28 Thus, it is suggested that it may produce analgesic and anti-inflammatory effects. Furthermore, it was shown by pharmacological studies that S. lavandulifolia Vahl has analgesic, anti-inflammatory, 16 and anxiolytic properties. 15 As there is a relationship between anxiety and pain in dysmenorrhea, 29 a portion of the observed therapeutic effects might be related to its anxiolytic activity. As described in the literature, thymol may have some spasmolytic effects, which are mediated through an inhibitory effect on calcium channel and ultimate inhibition of spontaneous contractile activity in smooth muscle cells. 22
It has been shown that the extract of S. lavandulifolia Vahl can inhibit ileum contractility, mainly by disturbing the calcium mobilization and partly by opioid receptor activation. 30 A more recent study has been suggesting the involvement of TNF-α and IL-1β in the antinociceptive and anti-inflammatory activity of S. lavandulifolia Vahl in suppressing orofacial pain following oral administration. 17 The use of this herb for primary dysmenorrhea can alleviate both signs and symptoms of dysmenorrhea, which include spasm and diarrhea due to prostaglandin release in menstruation. 31
Although NSAIDs have acceptable efficacy in treating primary dysmenorrhea, they may have some gastrointestinal side effects. 32 Gastroprotective effects of S. lavandulifolia Vahl has been shown on experimental gastric ulcer by gastric mucosal nitric oxide production. 30 It is possible to speculate that the use of this herb may increase the compliance of patients in taking NSAIDs by prevention of NSAID-induced gastropathy.
One study has shown that S. lavandulifolia Vahl extract may have some protective properties on gastric mucosa. This gastroprotection may be mediated by gastric mucosal nitric oxide production. Thus, the use of this herb in comparison with NSAIDs will have more compliance regarding its gastroprotective effects. 30 Oral contraceptives may also be considered; however, some patients do not desire hormonal contraception for this purpose.
In our study, due to ethical considerations, all patients were given the option of using mefenamic acid for pain reduction if needed. As the results have shown a reduction of pain intensity and total consumption of mefenamic acid in a cycle that patients received Stachys capsules in comparison with basic and placebo cycles, it may strongly be suggested that any observed reduction of pain intensity in Stachys cycle was achieved significantly, in addition to the reduction of mefenamic acid consumption. In other words, if the patients were allowed to omit the use of NSAIDs in this study, the reduction of pain intensity in Stachys cycle would have been more obvious with bigger effect size.
No specific side effects were reported following consumption of the herbal capsules, which is in line with an earlier study that showed few tolerable side effects like abdominal cramps and bloating in management of polycystic ovaries using S. lavandulifolia. 33
Since the study was limited to evaluation of the effectiveness, long-term safety and side effects of consumption of S. lavandulifolia was not addressed in this study. The randomization method was also simple. Another limitation of this study was the limited sample size. However, it was a pilot study in design to pave the way for further larger trials. Further studies are required to clarify the efficacy of S. lavandulifolia by comparing the prepared formulation with standard treatment for primary dysmenorrhea.
Conclusion
This study has shown that S. lavandulifolia Vahl-prepared formulation can reduce menstrual pain and can be used as an add-on therapy with NSAIDs to reduce the frequency of NSAID's use, or it can even be used as an alternative remedy to NSAIDs with fewer side effects. More extensive studies with longer follow-up period are needed to evaluate the effect and safety profile of the intervention.
Footnotes
Acknowledgment
The authors wish to honor the loving memory of Dr. Fatemeh Mohammadyari, a teacher, researcher, and dear friend who passed away young and is missed by many. She gave us great assistance in patient recruitment. Moreover, the authors wish to thank Farhad Rezakhani for his valuable assistance in the analytical division of Jaber Ebne Hayyan pharmaceutical Co. and also Dr. Elnaz Roohi for her efforts in reviewing the article. Financial support was provided by the Islamic Azad University, Pharmaceutical Sciences Branch, a nongovernmental nonprofit organization.
Author Disclosure Statement
No competing financial interests exist.