
Abstract
Background/Objective:
Respiratory problems can aggravate pain located in the coincident areas with tender points in the upper half of the body in patients with fibromyalgia (FM) and easily become fatigued, thus can lead to a decrease in the functionality of daily activities. The purpose of this study was to examine the effects of a breathing exercises program on pain thresholds tolerance on tender points and FM impact on daily life.
Methods/Design:
Thirty-five women with FM (age 34–67 years) were randomly assigned to an exercise group (n = 18), performing breathing exercises (30 min/session, 7 times/week; for 12 weeks), or to a control group (n = 17). Pain thresholds tolerance on tender points were measured by the physician using digital pressure algometer and FM impact on daily life was evaluated with the Portuguese version of the Fibromyalgia Impact Questionnaire (FIQ).
Results:
After 12 weeks of breathing exercises significant improvements were observed in the mean values of the treatment effects on pain thresholds tolerance on tender points and in the functional capacity to perform daily life, pain, and fatigue in favor of the exercise group. Gains in second rib, occiput, and supraspinatus pairs of the tender points predict improvements in the functional capacity, pain, and fatigue.
Conclusion:
Our study demonstrated that breathing exercises produced relevant benefits on pain thresholds tolerance on tender points located in the upper half of the body, some of which predicted improvements in the impact of FM in the functional capacity to perform daily life, pain, and fatigue. These results provide further support of an idea that breathing exercises are a real and effective intervention to consider in women with FM.
Trial Registration:
International Standard Randomized Controlled Trial Number ISRCTN37081460, available information in
Introduction
F
In pathologies as chronic obstructive pulmonary disease (COPD) or asthma, which also present respiratory muscle weakness, these sorts of programs based on breathing exercises are applied with success, improving the quality of life and/or exercise ability. 9,10 Nevertheless, the rehabilitation of the respiratory muscles in patients with FM has been little explored. In these patients only breathing exercises were included in multimodal programs where they were carried out together with relaxation and physical exercises, 11 or become part of techniques such as t'ai chi or qigong. 12,13 Hence, it is crucial to know the effects of breathing exercises, focused in psychological relaxation and motor control component, to show if they may become, by themselves, an alternative therapy in patients with FM.
On the other hand, respiratory disorders can aggravate pain located in the cervical paravertebral, intercostal, and thoracolumbar spine muscles. 3 These areas are coincident with the tender points located in the upper half of the body of the patients with FM. So, the present study considers the hypothesis that the improvement of the respiratory muscles can reduce pain on the tender points located in the upper half of the body (low cervical, second rib, occiput, trapezius, and supraspinatus). Moreover, as the pain located mainly in the upper half of the body compromises the daily life of the FM patients, 14 these improvements in pain thresholds of the tender points in the upper half of the body, would also be associated with the improvements in FM impact on the daily life of the patients.
With this idea, our group developed a pilot randomized controlled trial of 12 weeks where a breathing exercises program was applied having as objectives: (1) to provide knowledge of the effects of a breathing exercises program about pain and the FM impact, and (2) to verify whether the changes in pain thresholds on the tender points are associated with improvements in the daily life of patients.
Materials and Methods
Participants
Women were recruited by advertisements at the local Fibromyalgia Association–Myos (Lisbon District). They were included if they met the diagnosis of FM according to the American College Rheumatology (ACR). 1,15 Our physician verified the diagnosis of FM with 1990 ACR criteria 1 and with the provisional criteria of the ACR 2010. 15 The exclusion criteria were severe spinal injuries, severe musculoskeletal abnormalities, inflammatory rheumatic diseases, psychiatric disorders that increased the FM, and also, if they were taking part in another psychological or physical therapy. After having written the informed consent, 35 patients were randomized, 1:1 ratio, into an exercise group (EG; n = 18) or a control group (CG; n = 17). Two patients were excluded as they failed to attend at least 90% of the training sessions and three of them as well, since they missed the follow-up assessment. Finally, 15 patients in the EG and 15 in the CG fully completed the study protocol (Fig. 1).
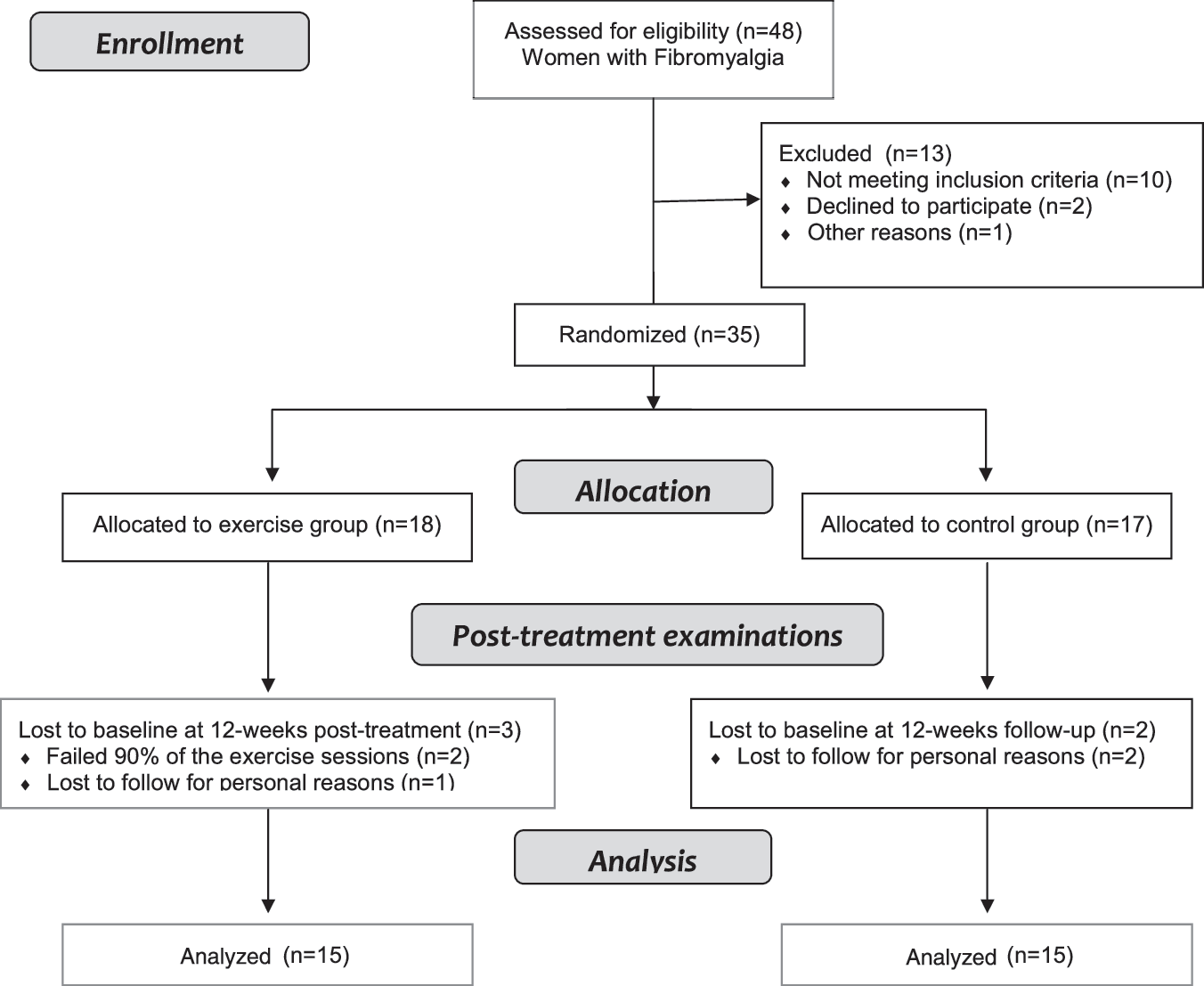
Consolidated Standards of Reporting Trials (CONSORT) flow diagram of the progress of the two groups in this pilot randomized controlled trial.
Pain thresholds tolerance on tender points and FM impact on daily life were assessed at baseline and immediately after 12 weeks of breathing exercises program. Each test was performed by the same specialist in the evaluation to reduce variability and improve consistency in the assessment process. The specialist was blinded to the patient's condition and group assignment. Randomization was conducted by computer (Research Randomizer) generating a sequence that was carried out by a staff member who was not otherwise involved in the study.
Measurements
Primary outcome measures: pain thresholds tolerance on tender points
Pain thresholds tolerance on tender points were measured only for research purposes, since they were eliminated of the criteria ACR 2010, 15 by the physician in baseline using a digital pressure algometer (Digital Pain Meter; Miacalcic®; PB by NIM brevettato, Siena) following the criteria ACR. 1 Since the intervention focused on the respiratory muscles, after 12 weeks only the five pairs of tender points located on the body trunk and neck were individually measured: low cervical (at the anterior aspects of the intertransverse spaces at C5–C7), second rib (at the second costochondral junctions, just lateral to the junctions on upper surfaces), occiput (at the suboccipital muscle insertions), trapezius (at the midpoint of the upper border), and supraspinatus (at origins, above the scapula spine near the medial border). The examiner placed the rubber tip on the examination site and the pressure gradually increased at a rate of ∼1 kg/cm2 per second. The patient was asked to report the moment when the sensation at the examination site changed from pressure to pain. A tender point was considered positive when the patient manifested pain with a pressure ≤4 kg/cm2.
Secondary outcome measures: FM impact on daily life
The Portuguese version of the Fibromyalgia Impact Questionnaire (FIQ) was used to evaluate FM impact on daily life. 16 This instrument measures functional capacity to perform daily activities (such as walking, cooking, cleaning, etc.), well-being, work missed, job ability, along symptoms of pain, fatigue, morning tiredness, stiffness, anxiety, and depression. The scale of each item runs from 0 to 10 and the FIQ total score from 0 to 100, where a higher score indicates a greater influence of FM on daily life.
Intervention
The breathing exercises program consisted of 30 min/session for 7 times/week during 12 weeks: 1 time supervised by an expert in breathing exercises, and 6 times/week unsupervised at home with audiovisual training through digital versatile disc. Each participant was highly motivated (in the supervised session; 1 time/week) to perform breathing exercises and with the aim of monitoring the unsupervised training sessions, they signed an attendance sheet every time they did the session, otherwise, they had to explain the reason why they could not do the session. Each session was focused on breathing exercises that strengthened and lengthened the thorax and abdomen skeletal muscles, including five breathing exercises (3 min for each one), which were performed in a circuit form (2 circuits/session) including, an exercise on awareness of breathing: in the supine position, inspire by the nose and exhale through the mouth with lips half-closed slowly; an exercise on costal expansion: in the supine position, with arms along the body with a stick held by the hands. Raise the arms and inspire and exhale and lower your arms; and three exercises on diaphragmatic breathing: exercise 1—in the supine position, overlapping hands on the diaphragm located in the abdominal region: inspire by the nose and exhale through the mouth with lips half-closed slowly; exercise 2—in the prone position, with a folded towel under the diaphragm located in the abdominal region: inspire through your nose and exhale through the mouth with lips half-closed slowly; and exercise 3—in the supine position, with a weight of 1 kg on the diaphragm located in the abdominal region: inspire by the nose and exhale through the mouth with lips half-closed slowly (Fig. 2).

Breathing exercises: (1) awareness of breathing; (2) costal expansion; (3) diaphragmatic breathing—exercise 1 in the supine position; (4) diaphragmatic breathing—exercise 2 in the prone position; (5) diaphragmatic breathing—exercise 3 in the supine with a weight of 1 kg on the diaphragm located in the abdominal region. Permission for image use was obtained with the authorized person's signature.
Statistical analysis
Normality of data was initially tested using the Kolmogorov–Smirnov test using the correction of Lillifort. Between groups differences at the baseline characteristics were tested using one-way analysis of variance (ANOVA) test for continuous variables, and chi-square test for categorical variables. The primary outcome measures are the five pairs of tender points individually measured. The treatment effects in percentage (and 95% confidence intervals) show the effects of breathing exercise in all variables and were obtained using ANOVA (univariate general linear model) of relative change, in percentage, to the initial status in the EG minus relative change to the initial status in the CG (treatment effect (%) = ΔEG – ΔCG)], in which the percentage of relative change to the initial status was calculated with computer variable: [(Variable12-weeks − Variablebaseline)/Variablebaseline] × 100. Effect size (ES) was calculated in all variables for ΔEG – ΔCG with Cohen's d = M1 − M2/Spooled; where Spooled = √[(s1 2 + s2 2)/2]. The magnitude of change considered was small (0.20), moderate (0.50), and large (0.80). To show the predictive capacity of gains in threshold tolerance on tender points to improve the FM impact on daily life, a model of linear regression analysis was applied, where only the pairs of the tender points that improve after the breathing exercise program (second rib, occiput, and supraspinatus) were included. The assumptions of linear regression analysis (e.g., linearity, normal distribution and scattering of residuals, multicollinearity) were tested and they were found to be reasonably valid. For all tests the significance level was set at p < 0.05. All analyses were performed using IBM SPSS statistical software version 22.0.
Results
Baseline data did not show any significant differences between the EG and CG in sociodemographic characteristics (Table 1), pain thresholds tolerance (Table 2), or FM impact on daily life (Table 3). The rate of compliance with training sessions in the EG was 78.6 ± 5.3 (mean ± standard deviation) times out of a maximum of 84 sessions.
Values expressed as mean ± standard deviation; p-value of analysis of variance.
Values expressed as percentage; p-value of analysis of Chi-square.
CG, control group; EG, exercise group.
Values expressed as mean (95% CI). p-Values of analysis of variance (univariate general linear model) to compare differences between groups after 12 weeks of intervention (ΔEG − ΔCG; where ΔEG =
CG, control group; CI, confidence interval; D, dominant side; EG, exercise group; ND, non dominant side.
Values expressed as mean (95% CI). p-Values of analysis of variance (univariate general linear model) to compare differences between groups after 12 weeks of intervention (ΔEG – ΔCG; where ΔEG = [(Variable12-weeksEG − VariablebaselineEG)/VariablebaselineEG] × 100; and ΔCG = [(Variable12-weeksCG − Variable baselineCG)/VariablebaselineCG] × 100. Effect size: Cohen's d = M 1 − M 2/spooled; where spooled = √[(s1 2 + s2 2)/2].
CG, control group; CI, confidence interval; EG, exercise group; FIQ, Fibromyalgia Impact Questionnaire.
Pain thresholds tolerance on tender points and FM impact on daily life
After 12 weeks of intervention, significant benefits were observed in pain thresholds tolerance on tender points: second rib (33%; ES = 0.53), occiput (48%; ES = 0.95), and supraspinatus (63%; ES = 0.82). The sum of the five pairs of the tender points (low cervical, second rib, occiput, trapezius, and supraspinatus) also showed significant improvements in the mean values of the treatment effects (27%; ES = 0.86), in favor of the EG (Table 2). In addition, the exercise intervention led to improvements in the mean values of the treatment effects, which were found in the functional capacity to perform daily life (43%; ES = 1.06), pain (20%; ES = 0.86), and fatigue (39%; ES = 0.92) in favor of the EG. However, it was not enough to obtain significant results in the FIQ total score, although the trend was for improvement (13%; ES = 0.58) (Table 3).
Predictive capacity of changes in pain thresholds tolerance on tender points for improvements in FM impact on daily life
Multivariate regression analyses indicated improvements in second rib, occiput, and supraspinatus pairs of the tender points predicting gains in functional capacity [F(3, 24) = 3.486, R2 = 0.303, p = 0.031], pain [F(3, 24) = 6.667, R2 = 0.455, p = 0.002], and fatigue [F(3, 24) = 7.963, R2 = 0.499, p = 0.001].
Discussion
The current study with 12-week breathing exercises program not only led to significant improvements in pain thresholds tolerance on tender points located in the upper body of patients with FM, but also, these gains in pain thresholds tolerance induced for breathing exercises program predicted improvements in functional capacity, pain, and fatigue.
Programs based on breathing exercises are usually used in patients with COPD establishing positive effects on dyspnea, fatigue, and quality of life. 8 Respiratory exercise programs, where breathing exercise were correspondingly applied, were effective in improving respiratory muscle weakness, which was associated with improvement in quality of life, in asthma patients as in healthy persons more than 60 years old. 17,18 Nevertheless, in patients with FM breathing exercises were only applied in multimodal programs combined with physical exercise and relaxation, or also they were included in “meditative movement” such as t'ai chi and qigong, manifesting positive benefits in FM impact on daily life, pain, sleep, physical function, and flexibility. 11 –13 Physiologically, the diaphragm is the most important muscle during quiet breathing, however, other muscles as the scalenes and parasternal intercostals are also activated during this breathing, and with the increase of exercise intensity the sternomastoids are required. 19 It is known that respiratory problems can aggravate pain localized in the cervical paravertebral, thoracolumbar spine and intercostal muscles of the patients with FM, 3 where some of the tender points are located. In this way, physical exercise can increase (positive) the pain thresholds of the tender points in patients with FM, 20 even combined with psychological sessions doing part of a multidisciplinary intervention. 21 Also, previous programs that included 3–8 weeks of breathing exercises in their activities (qigong, training in mindfulness meditation, education/cognitive-behavioral component, and formal relaxation/meditation training) showed improvements in pain thresholds tolerance or tender points count. 22 –25 So, the present study showed improvements in the sum of the pain thresholds of the five pairs of the tender points localized in the trunk and cervical (low cervical, second rib, occiput, trapezius, and supraspinatus) with large magnitude of change (ES = 0.86). However, we must be cautious with these results since the vast majority of the tender points measured individually showed a moderate magnitude of change (ES >0.50). Besides, following the recommendations for classifying pain responses in chronic pain patients for clinical trials (IMMPACT), in the present study the reductions of pain of the tender points from baseline are considered minimally important in low cervical dominant side, second rib dominant side, and trapezius dominant and non-dominant side (<30%); moderately important in low cervical non-dominant side, second rib non-dominant side, occiput non-dominant side, and supraspinatus dominant side (≥30%); and of substantial important in occiput dominant side and supraspinatus non-dominant side (≥50%). 26 This improvement in the pain thresholds of our patients could have its origin in the slow breathing, specific of the intervention performed in this study, which reduces pain before slightly painful stimulus, 27 as the pressure realized by an algometer.
On the other hand, it was reported that pain threshold measured by dolorimetry scores was correlated with clinical symptoms as pain and fatigue, 28 which can explain that the increase of the pain thresholds showed in our study predicts the improvements in widespread pain and fatigue. The present study demonstrates similar improvements in widespread pain to previous studies that realized “meditative movement” included breathing techniques (others 12,13 13%–16% vs. our 20%), where our study showed a magnitude of change considered large (ES = 0.86). Furthermore, this improvement in pain is considered as an important clinical difference, ∼2-point improvement on a scale of 0 to 10. 29 In this sense, the exercise can influence pain regulation systems of the patients, and the improvements obtained might be, in part, the result of increases in the functional capacity of pain modulatory system. 30 However, previous literature indicated higher improvements in pain (≈44%) than in our study after qigong program involving meditation, deep breathing, and synchronized rhythmic body movements using specific pain questionnaires. 31 These differences relatively to the current study could be partially due to the fact that visual analogic scale is a one-dimensional instrument, and pain manifestation is a multidimensional experience that might be affected by other facts as fatigue. 32 Therefore, patients with FM describe their fatigue as an overall feeling of tiredness or exhaustion, 33 having an essential role together with pain, in the physical function of the patients with FM reducing the participation in daily activities. 34 The current study shows improvement of 39% in fatigue after the intervention period. Despite being considered that a 14.1% change in the FIQ total score and 13.2% in the FIQ stiffness item as minimal clinically important difference, 35 unfortunately, in the FIQ fatigue item is not known as minimal clinically important difference. However, our results show a large magnitude of change (ES = 0.92), which can be considered as relevant improvement. Previous studies that used breathing exercises, 31,36 together with programs as yoga and qigong, involving meditation and gentle poses or synchronized rhythmic body movement, which were also effective in improving fatigue in patients with FM, demonstrated improvements of ≈25%, less than the present study. This could be because our patients showed, in baseline, high fatigue levels (>7.5; scale 0–10), which could contribute that the improvement, expressed in percentages, was greater. Moreover, our results showed that ≈50% of the fatigue improvements were predicted by the gains in pain thresholds on the tender points. This strong influence appears to make sense since pain and fatigue commonly co-occur, 34 and are established as the two first clinic characteristics of the FM, where the 54% of the patients indicated pain as the first symptom and the 28% fatigue as the main problem. 37
In preceding studies, pain threshold associations with strength, aerobic capacity, and flexibility were observed 38 and also that the 30% of variability in the pain threshold could be explained by strength and flexibility. 39 In this way, the increase of pain thresholds of our patients predicts 30% of the functional capacity to perform daily activities. This could be partially explained by the strengthening of the cervical paravertebral, intercostal, and thoracolumbar spine muscles, located in areas coincident with the tender points of the upper half of the body, which can aggravate localized pain when respiratory problems exist. 3 These are encouraging results since breathing exercises can improve pain thresholds on tender points of the upper half of the body and, thus, also improve functional capacity of patients with FM. Literature shows that patients with FM have a functional capacity similar to elderly persons relatively to flexibility, strength, balance, and aerobic capacity, which must be considered when physical exercise is prescribed by sport professionals. 38 In this context, our intervention based on breathing exercises showed improvements of the 43% in the functional capacity to realize daily activities and with ES = 1.06. Unfortunately, the minimal clinically important difference is neither known in the FIQ functional capacity item. However, our results show a large magnitude of change, which can be considered as relevant improvements.
The present study also included limitations, which require further discussion. The limited size of the sample may have contributed to decrease statistical power to detect changes in some variables. Nevertheless, our trial still showed positive effects in numerous measured variables and changes due to the treatment effect. On this matter, although the percentages of improvement in some pain thresholds after the intervention were high, the majority of tender points measured individually showed a moderate ES. Nevertheless, the sum of the five pairs of tender points shows a magnitude of change considered large. Even so, we must be careful, since the improvements in the pain thresholds showed by the patients could have a limited clinical relevance. Another limitation is related with the possibility of default of the intervention out of the scientific field. The patients should be highly motivated to exercise every day, which could be reached giving motivation by telephone on the side of the sport specialists once or twice per week, realizing periodic assessment to verify how patients are adapting to the breathing exercises, and we also suggest that these breathing exercises can be realized in an hour that the patients are relaxed, they could even be done on the bed just before sleeping time. Lastly, we also consider the functional capacity to perform daily life as a limitation since it only was measured with dimensions of the FIQ and not using objective specific physical tests.
Conclusions
The present study showed that 12 weeks breathing exercises program was effective to produce improvements in the sum of the five pain thresholds tolerance on tender points located in the upper body (especially second rib, occiput, and supraspinatus). The patients who had improvements in pain thresholds tolerance on tender points also showed a decrease of FM impact in functional capacity to perform daily living, pain, and fatigue. These results provide further support to an idea that breathing exercises, without using specific respiratory appliance, are a real and effective intervention to consider in the management of pain and for reducing FM impact on daily life of the patients.
Footnotes
Acknowledgments
The authors thank local Fibromyalgia Association–Myos for helping us to make contact with patients. We are also very grateful to all participants of this study. This study was supported by the National Funds through FCT—Portuguese Foundation for Science and Technology (UID/DTP/04045/2013)—and the European Fund for regional development (FEDER) allocated by European Union through the COMPETE 2020 Programme (POCI-01-0145-FEDER-006969).
Declarations
Author Disclosure Statement
No competing financial interests exist.