
Abstract
Background:
Probiotics are purported to reduce symptoms of allergic rhinitis. This study sought to determine the proportion of participants with an improvement in the mini Rhinoconjunctivitis Quality of Life Questionnaire (mRQLQ) in response to a multispecies probiotic supplement with a Simon Two-Stage design.
Methods:
This study was based on a Simon Two-Stage Design for p1 -p 0 = 0.18 to account for seasonal variation in symptoms. Under this design, ≥10 patients are required to exhibit an improvement in quality-of-life scores to determine that there was sufficient activity for the supplement to be considered effective. Participants consumed a probiotic supplement (Ecologic® AllergyCare; probiotik®pur) twice daily for 8 weeks. The primary outcome measure was based on a change in mRQLQ scores following supplementation. Secondary outcomes include assessment of change in symptoms and medication usage with a twice-weekly symptom and medication diary, nasal congestion by rhinomanometry, and total serum Immunoglobulin E (IgE) and specific IgE for Bermuda grass.
Results:
A total of 40 participants completed the study. A total of 25 participants (63%, 49–76%, p < 0.001; mean, 95% confidence interval, p-value) out of 40 participants had a clinically meaningful response to treatment based on assessment of mRQLQ. On average, mRQLQ scores changed from 2.83 ± 1.51 at baseline to 1.66 ± 1.36 at week 4 and 1. 38 ± 1.13 at week 8 (p < 0.01) (mean ± SD, p-value). Sum of individual symptom scores and overall symptom scores over the course of treatment was significantly reduced (p = 0.036 and p = 0.039, respectively). A moderate reduction in frequency of allergy-related medication use in the final 4 weeks of supplementation period was observed (52.5% weeks 0–4 to 41.4% weeks 4–8; average proportion of total diary responses, p = 0.085). The supplement was largely well tolerated by participants at the dose provided.
Conclusions:
The proportion of participants exhibiting improvement in quality-of-life metrics warrants continued investigation in the form of a phase III placebo-controlled trial.
Background
A
Probiotics may have beneficial effects in the prevention and management of a range of infectious and immune conditions, 10,11 including AR. 12 –15 The purported mechanisms responsible for improving AR symptoms by probiotics are poorly defined. One explanation is that specific probiotic strains have the ability to alter the composition of the gut microbiota and modify the host immune system. These immune modulatory effects have been recognized in cell culture models where specific probiotic strains have shown strong T helper 2 (TH2) suppressive abilities determined by cytokine and gene expression analysis. 16,17 There is also evidence that some probiotic strains may have the capacity to influence the development of tolerogenic dendritic cells, 18 stimulate Toll-like receptors, and promote the immunosuppressive regulatory T cell lineage. 19
While a number of studies have examined if probiotic supplementation can reduce AR symptoms in clinical settings, the results to date remain mixed. 15,20 The beneficial effects of probiotics are known to be strain specific, and differences in trial design, dosage, route of administration, and outcome measures make determining their efficacy difficult. 15,21,22 Therefore, additional well-controlled studies with clinically relevant outcomes are needed to better elucidate the effectiveness of probiotics in the management of AR. Given there is often a lack of early phase data to support phase III clinical trials, progressive phase II designs, such as the Simon Two-Stage design, provide early essential data and support for large phase III trials. Such an approach is consistent with good clinical practice guidelines for the clinical development of new products.
Methods
Study design
Full methodological details have been previously published. 23 Briefly, this phase II intervention study used a Simon Two-Stage design protocol to determine the response rate of AR sufferers to a multispecies probiotic supplement. Participants consumed a probiotic supplement twice daily for 8 weeks and attended the allergy clinic at the beginning and end of intervention for assessment. The Simon Two-Stage design protocol was defined as p1 -p 0 = 0.18 where p0 (noneffective treatment) was nominated as a response in ≤15% of participants and p1 (effective treatment) was as a response in least 33% of participants. 23 Response rates were calculated based on the proportion of participants reporting a clinically beneficial change in the validated mini Rhinoconjunctivitis Quality of Life Questionnaire (mRQLQ) 24 scores using a threshold of 0.7 as described in the work of Juniper et al. 24
Participants
Participants were both male and female aged between 17 and 65 years with a more than 2-year history of AR and positive allergic response to Bermuda grass (couch). Allergy status was confirmed through either a skin prick test and/or serum-specific IgE radioallergosorbent test (QML Pathology, Murarrie, Queensland, Australia) to Bermuda grass. Participants also underwent skin prick testing against a panel of dust mite and pollen allergens, to characterize the sensitivities of the cohort (Table 1). Participants were excluded on a number of criteria, including existing medical disease and medication usage as detailed previously. 23 Clinical assessments were conducted at the Queensland Allergy Services Clinic in Southport, Gold Coast, Australia, during the peak pollen season of September to March 2015–2016. This study was approved by the Griffith University Human Research Ethics Committee (Ref# 2015/564) and registered with the Australian and New Zealand Clinical Trials Registry (ACTRN12615001103550). All subjects provided written and informed consent before participation.
BMI, body mass index; cm, centimeters; IgE, Immunoglobulin E; kg, kilogram; kU, kilounits; L, liter; m2, meters squared.
Intervention
Participants consumed twice daily one sachet containing 2 g of the freeze-dried multispecies probiotic supplement (Ecologic® AllergyCare, Winclove Probiotics B.V., The Netherlands; marketed as probiotik®pur, Nutrimmun GmbH, Germany). 23 The probiotic preparation contained six bacterial strains Bifidobacterium bifidum W23, Bifidobacterium lactis W51, Lactobacillus acidophilus W55, Lactobacillus casei W56, Lactobacillus salivarius W57, and Lactococcus lactis W58 (total colony-forming units 1 × 109/g), as well as vitamin B2 (35 mg/100 g), biotin (750 μg/100 g), maize starch, and maltodextrins.
Outcome measures
The primary outcome of this study was the proportion of AR patients showing an improvement in mRQLQ scores in response to probiotic supplementation. 23 Participants completed the mRQLQ at baseline (week 0), midpoint (week 4), and postsupplementation (week 8). All items in the questionnaire were averaged to give an overall score. Specific domains of the mRQLQ were also recorded as a secondary outcome measure, including “nose symptoms” (consisting of questions relating to sneezing, stuffy blocked nose, and runny nose) and “eye symptoms” (consisting of questions relating to itchy eyes, sore eyes, and watery eyes). 24
Additional secondary endpoints were collated from an online symptom and medication diary completed twice weekly during the study. 23 The questionnaire scored overall severity of symptoms, along with specific symptoms (nasal itch, eye itch, sneezing, runny nose, postnasal drip, unrefreshed sleep, and sinus pain) experienced in the previous 24 h on a 11-point Likert scale (0 “No distress” to 10 “Unbearable distress”). The scores for each symptom were summed to give a “sum of individual symptoms” score with a possible maximum score of 70. The maximum “severity of symptoms overall” score was 10. Participants also reported all medications and supplements used over the last 24-h period. Change in self-reported frequency of medication used to treat AR symptoms was collated from this survey.
Nasal obstruction was assessed objectively presupplementation and postsupplementation by determination of unilateral nasal resistance measured with a Nasal Rhinomanometer (NR6 Rhinomanometer; GM instruments, Scotland, United Kingdom) and reported as 150 Pascals (Pa)/flow (cc/s).
Laboratory measures
Venous blood samples were collected at weeks 0 and 8 for analysis of full blood count, white cell differential, and specific IgE to Bermuda grass. Analyses were completed by a local pathology provider (QML Pathology, Murarrie, Queensland, Australia). Erythrocyte sedimentation rate (ESR) over 1 h was measured using fresh blood samples collected in sodium citrate tubes and using commercially available Vacuette ESR pipettes (Greiner Bio-One, Kremsmünster, Austria) as per the Westergren method. 25 For total IgE and Immunoglobulin G (IgG), serum samples were separated by centrifugation at 3500 rpm for 10 min and stored at −80°C until analysis. Total serum IgE and IgG were measured using commercially available enzyme-linked immunosorbent assay kits (eBioscience, San Diego, CA).
Statistical analysis and sample size calculation
Full methodological details of the sample size calculations have been previously published. 23 Statistical analyses were performed with IBM SPSS Statistics for Windows, Version 23 (IBM Corporation, Armonk, NY). Data are reported as mean ± SD or mean effect and 95% confidence interval (95% CI) unless otherwise indicated. Change in mRQLQ scores, nasal resistance measures, and blood examinations presupplementation to postsupplementation were assessed with a t-test. Changes in biweekly symptom scores were assessed with a one-way analysis of covariance, where presupplementation baseline values were used as covariates. If a main effect was detected for the symptom scores, Fisher's Least Significant Difference tests were used to identify which survey response entries differed during the intervention. Frequency of medications to manage AR symptoms (i.e., oral antihistamines, nasal steroid sprays, antihistamine nasal sprays, and eye drops) was tallied for each participant and expressed per number of symptom and medication diary responses for weeks 1–4 versus weeks 5–8 of intervention. Statistical significance was accepted at p < 0.05.
Results
Baseline characteristics of participants, compliance, and tolerability
A total of 44 participants were recruited to the study, with the clinical response to supplementation evaluated in 40 participants (Fig. 1). A total of four participants did not complete the trial. Reason for withdrawal included gastrointestinal disturbance (n = 2) and inability to meet study requirements due to personal commitments (n = 2). The demographic and baseline characteristics of the study group are given in Table 1. In general, the study cohort comprised middle-aged adults, majority female (60%), and in the healthy-to-overweight range according to body mass index (BMI). The majority of participants in the cohort (80%) reported a family history of allergic disease.
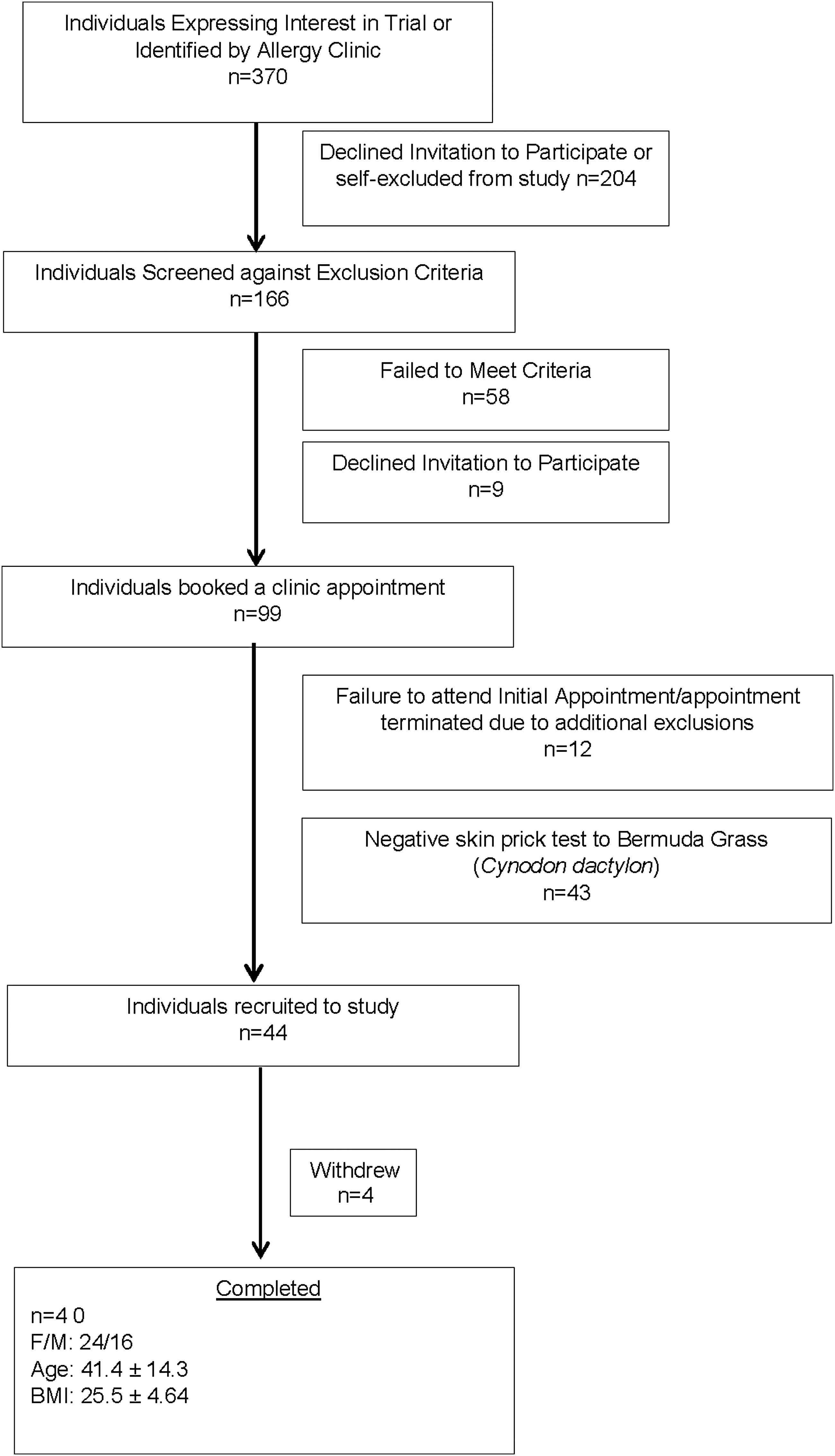
Study flow diagram indicating participant progression and retention for an 8-week study of a multispecies probiotic supplement. BMI, body mass index.
The supplement was well tolerated by the majority of participants. Reported adverse events for all recruited participants were predominantly gastrointestinal in nature (n = 16) (change in bowel habits, feelings of excess bloating/gas, or nausea) and short-lived, typically occurring within the first few weeks of supplementation. These adverse events are consistent with reports from other probiotic studies. 15,26 Other reported adverse events included increased thirst (n = 1) and acne breakouts (n = 1). Compliance was 92% ± 7%, which was calculated from returned supplement and self-report.
Clinical response to probiotic supplementation (mRQLQ)
After 8 weeks of supplementation, 25 participants (63%, 49%–76%, p < 0.001; mean, 95% confidence interval, p-value) showed an improvement in mRQLQ scores greater than 0.7 U (0.71–4.07 U). An additional 10 participants showed improvement in mRQLQ scores under 0.7 U (0.07–0.64 U). Using the threshold for a defined beneficial effect (>0.7 U change), three participants showed no change in mRQLQ scores following supplementation (0 U, −0.21 U, −0.29 U). Only two participants showed increasing mRQLQ scores (−1.21 and −1.10 U), which could suggest a worsening of rhinitis symptoms. A propensity for improvement in AR symptoms was also evident at week 4 of the study; 20 participants (51%, 38%–65%, p < 0.001) exhibited an improvement in mRQLQ scores greater than 0.7 U (0.79–3.92 U), eight participants showed an improvement in mRQLQ less than 0.7 U (0.21–0.64 U), and six participants exhibited a worsening of mRQLQ scores (−0.9 to −0.07 U).
Overall, global mRQLQ scores decreased from 2.83 ± 1.51 at baseline to 1.66 ± 1.36 at week 4 and 1.38 ± 1.13 at week 8 (p < 0.01) (Fig. 2). The scores for the “eye symptoms” and “nose symptoms” domains of the mRQLQ also significantly improved following supplementation. For the “eye symptoms” domain, scores decreased from 2.83 ± 1.74 at baseline to 1.16 ± 1.31 at week 8 (p < 0.01) and for “nose symptoms,” scores decreased from 3.10 ± 1.80 at baseline to 1.38 ± 1.30 at week 8 (p < 0.01).
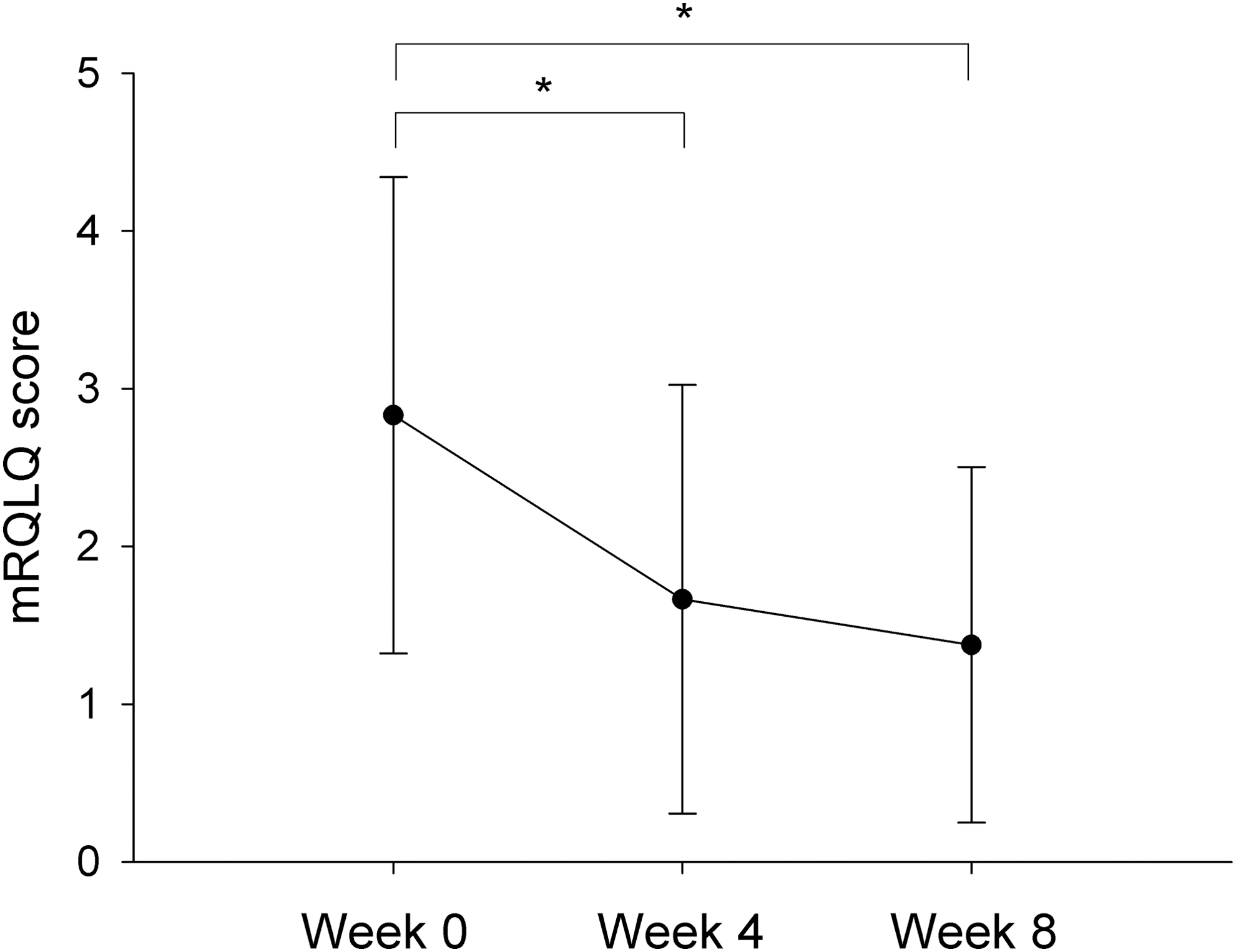
mRQLQ scores at baseline, midpoint, and postsupplementation. Data are presented as the group mean ± SD. A significant improvement in mRQLQ scores was observed at midpoint and postsupplementation when compared to baseline. Asterisks indicate significant difference (p < 0.05). mRQLQ, mini Rhinoconjunctivitis Quality of Life Questionnaire.
There were no significant differences between responders and nonresponders in baseline measures of age, gender, BMI, family history of allergic disease, total and specific IgE, co-allergy to dust mites, or week recruited to study (Table 2). There was also no significant difference between responders and nonresponders in reported frequency of allergy medication usage during the supplementation period (responders 27.6% ± 32.8% versus nonresponders 22.8% ± 29.9%, p = 0.65). A notable feature of the intervention was that participants exhibiting a higher baseline global mRQLQ were more likely to meet the clinical threshold for global mRQLQ improvement.
N.b. Responders were significantly more likely to be allergy medication users and have higher mRQLQ scores at baseline. Participants were classified as a medication user based on reporting of allergy-related medication use at baseline screening.
Lavene's test indicated unequal variances.
BMI, body mass index; mRQLQ, mini Rhinoconjunctivitis Quality of Life Questionnaire.
Effects of probiotics on symptoms and frequency of medication usage
Based on the symptom and medication diaries, there was a significant reduction in the sum of individual symptom scores and overall symptom scores over the course of supplementation (p = 0.036, Fig. 3). Post hoc analysis of the sum of individual symptom scores revealed that symptom severity scores were significantly lower than presupplementation at survey response number 7 (p = 0.015), 8 (p = 0.049), 11 (p = 0.012), 12 (p = 0.034), 13 (p = 0.007), 14 (p = 0.002), 15 (p = 0.001), and 16 (p = 0.001). Similarly, there was a significant reduction in the severity of overall symptoms over the treatment period (p = 0.039, Fig. 3). Post hoc analysis revealed that overall symptom scores were significantly lower than presupplementation at survey response number 7 (p = 0.013), 12 (p = 0.041), 13 (p = 0.018), 14 (p = 0.002), 15 (p = 0.003), and 16 (p = 0.001).
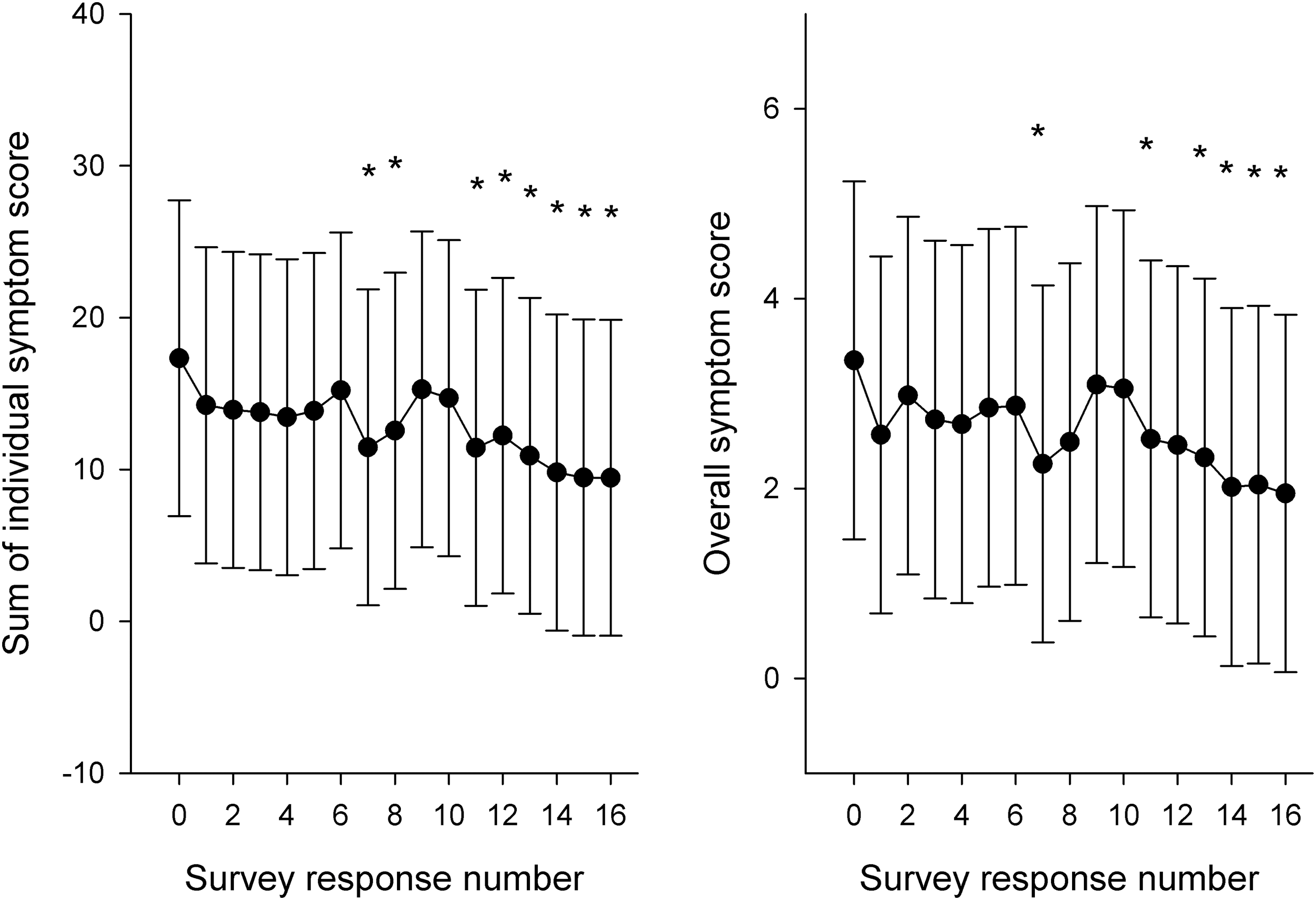
Sum of individual symptom scores (left panel) and overall symptom scores (right panel) measured biweekly during the 8-week intervention. Baseline (presupplementation) corresponds to survey response number 0. Data are presented as the adjusted group mean ± SD. Asterisks indicate significant difference from baseline (p < 0.05).
There was a moderate reduction in allergy medication usage over the course of the study. A total of 23 out of 40 participants reported use of allergy-related medications during the trial period. Of these participants, use of allergy medications was reported, on average, in 52.5% of symptom and medication diary responses during weeks 0–4 and, on average, in 41.4% of diary responses in weeks 5–8 (p = 0.085).
Effects of probiotics on nasal congestion and laboratory measures
There was no significant reduction in total nasal resistance following supplementation, based on rhinomanometry measurement (baseline 0.44 ± 0.26 vs. week 8 0.73 ± 1.19, p = 0.3). No significant change in full blood count, white cell differential, total IgE and IgG, specific IgE to Bermuda grass, and ESR was observed in response to supplementation (Table 3).
ESR, erythrocyte sedimentation rate; IgE, Immunoglobulin E.
Discussion
This study obtained an estimate of the treatment effect of a specifically designed multispecies probiotic supplement in AR sufferers using a Simon Two-Stage design. In this study, 10 participants or more were required to demonstrate an improvement in their mRQLQ scores at a level greater than the predefined clinically beneficial threshold (0.7) to accept that the probiotic supplement had sufficient activity to deem it effective 23 and worthy for further studies in phase III trials.
The mRQLQ is a commonly used and validated tool that has strong discriminative and evaluative measurement properties. 27 In a systematic review evaluating the performance of rhinitis quality-of-life surveys, the mRQLQ was found to be superior to other rhinitis surveys in measures of overall quality and reliability. 28 The mRQLQ has been applied as an assessment tool in many clinical studies examining AR treatments, including probiotics. 29 –33 In addition, the utility of quality-of-life surveys in clinical practice is also becoming increasingly recognized. 34 –36
Overall, 25 participants experienced a clinically meaningful improvement in mRQLQ scores following probiotic supplementation. The positive findings for improved mRQLQ scores are further supported by the significant improvement in individual symptoms and in overall symptom severity over the course of the supplementation period. Furthermore, the frequency of use of allergy-specific medications was moderately reduced in the final 4 weeks of supplementation. Collectively, these findings provide initial evidence that supplementation with this specific multispecies probiotic formulation may be effective at reducing symptoms and improving the quality of life in AR sufferers.
Phase II studies during early clinical investigation can determine whether an intervention has sufficient activity to warrant continued investigation and provide estimates of effect size for designing phase III clinical trials. 37 Under this Simon Two-Stage design, 33% of participants were required to exhibit an improvement in mRQLQ scores greater than 0.7 of a unit change, to consider the treatment worthy of continued investigation. 23 The findings of our study hold even when the threshold for improvement in mRQLQ is increased above a 1.0 U change, indicating a robust effect of supplementation in this cohort. The observation that ∼63% of the study cohort experienced an improvement in quality-of-life measures is considerably higher than the prespecified target of 33%.
The consistency of change in the symptom scores, quality-of-life scores, and medication usage further supports the beneficial effects of this multispecies supplement in AR. An improvement in RQLQ scores or reduction in AR symptoms following intervention with probiotics, similar to that in this study, has also been established in a number of other trials. 12,13,38 –40 Overall, our cohort comprised participants with moderate mRQLQ scores (average 2.8 at baseline). Participants who experienced a positive response to probiotic supplementation typically had higher mRQLQ scores and were more likely to report medication use at baseline in comparison to participants who did not respond. This suggests that disease severity was initially greater in responder group. The effects of the investigational multispecies probiotic in a cohort of individuals with more persistent/severe AR symptoms are not known, and given the results of the subgroup analysis, is worth investigating as a target group in future studies.
To date, the efficacy of probiotics in reducing symptoms of AR is unclear. This is predominantly due to differences in trial design between studies, and varying features of supplementation such as probiotic formulation, mode of administration, and length of supplementation. 15,21,22 While our study was similar to other probiotic studies in duration of supplementation and outcome measures (i.e., quality of life and symptom surveys), the probiotic supplement studied here contains a greater number of strains than previous studies. 23 The higher number of strains contained in the supplement may account for the robust positive effects observed, possibly due to synergistic effects between strains. 41,42
No change in nasal resistance measured by rhinomanometry 23 was observed following supplementation. Interestingly, a substantial reduction in perceived nasal stuffiness was recorded in the self-reported questionnaire for this study (data not shown). As this study was a community-based trial, prior exposure to allergens in the hours before testing could not be controlled for. Moreover, as assessments of nasal obstruction were made at two time points, only day-to-day variation of nasal resistance is not known. Community-based studies employing this technology should consider controlling for environmental allergen exposure and incorporating more frequent testing throughout the intervention period.
In this study, no significant changes in the concentration of total serum IgE, or specific IgE for Bermuda grass were observed. However, the observations of an improvement in AR symptoms without corresponding changes in serum IgE are consistent with other probiotic studies. 40,43 –45 In practice, the presence of elevated total IgE levels in serum is a nonspecific marker of allergy, and considerable levels of specific IgE levels indicate sensitization toward a particular allergen. 46 As such, we sought to characterize the IgE levels of participants in our study.
The supplement in this study, taken twice daily for 8 weeks, was well tolerated by the majority of participants. This is not surprising, as Lactobacilli and Bifidobacteria occur naturally in mammalian gut microbiota, and these bacteria have been widely consumed in society through food products and supplements for decades. 47 Reported adverse events were mostly transient and gastrointestinal in nature (occurring within the first few weeks of supplementation), which is consistent with probiotic research. 15,26 Indeed, probiotics have the known potential to modulate the composition of the gut microbiota and increase fermentation of complex carbohydrates. The strains contained in the probiotic supplement studied here have a positive in vitro safety profile, and have been granted European Food Safety Authority (EFSA) “qualified presumption of safety.” Although adverse events were limited in our study, this study was otherwise not designed to assess safety.
While this design protocol avoids some of the pitfalls of small underpowered clinical trials, it is not without limitations. In the absence of a placebo group, a conservative rate was chosen for p 1 to buffer for a placebo effect and natural variations in disease across the pollen season. However, to overcome this limitation, a rolling recruitment strategy was adopted so that participants completed the study at multiple points throughout the pollen season, thereby minimizing the influence of varying environmental pollen load during the study period. To reduce study-related burden on participants and maintain participant retention, symptom and medication use were recorded on a biweekly basis. From these data, a general trend in symptom fluctuations can be derived, although greater resolution would be obtained from more frequent monitoring.
Conclusions
This study revealed that a large proportion of participants with AR demonstrated a clinically meaningful improvement in mRQLQ scores in response to supplementation with a specifically designed multispecies probiotic. The change in mRQLQ scores and symptom scores was also significantly reduced following supplementation with the probiotic formulation. The data generated from this study provide initial evidence of efficacy for this probiotic supplement for AR, and provide the basis for continued follow-up investigation in the form of larger phase III placebo-controlled studies.
Footnotes
Acknowledgments
The authors would like to gratefully acknowledge the valuable contributions of the trial participants. The assistance of the Queensland Allergy Services Clinic in providing clinic access and for performing the skin prick tests and Rhinomanometry assessments is appreciated. Funding for this study is provided by Winclove Probiotics B.V. (The Netherlands).
Author Disclosure Statement
I.B.–v.d.V. is employed at Winclove Probiotics B.V. This does not alter this author's adherence to all publication policies on sharing data and materials. All other authors have no conflicts of interest to declare.