
Abstract
Background:
Tanreqing injection (TRQ) is often used in the treatment of pulmonary infection in patients with tuberculosis (TB). But its efficacy and safety are still unclear; to further reveal its efficacy and safety, the authors systematically evaluated all relevant trials.
Methods:
The authors searched published trials using the search strategy as (Tanreqing OR “Tanreqing injection”) AND (“Tuberculosis” [MeSH] OR Tuberculosis OR TB) in Embase, PubMed, CNKI, VIP, Wanfang Database, CBM and CENTRAL, and ongoing trials in Chinese and U.S. clinical trials and World Health Organization International Clinical Trials Registry Platform (WHO-ICTRP) (established to January 2017). The authors evaluated the methodological bias risk of all included trials using the Cochrane evaluation handbook of randomized controlled trials (RCTs) (5.1.0), extracted data following the PICO principles, and synthesized the data using meta-analysis.
Results:
Twenty-six RCTs involving 2404 patients were included. In TRQ alone versus antibiotics, the merged risk ratio (RR) values and their confidence interval (95% CI) of meta-analysis for overall efficacy, lesion absorption, and bacterial clearance were as follows: 1.05 (0.99–1.10), 0.98 (0.89–1.08), and 1.36 (1.09–1.70). All differences were not statistically significant. In TRQ plus antibiotics versus antibiotics, the RR values and their 95% CI of overall efficacy, lesion absorption, and bacterial clearance were as follows: 1.17 (1.10–1.25), 1.24 (1.11–1.38), and 1.61 (1.36–1.90). All differences were statistically significant. Except for the bacterial clearance, sensitivity analyses showed that the overall efficacy had good stability.
Conclusions:
TRQ may have the same overall efficacy as antibiotics in pulmonary infection in patients with TB. TRQ plus antibiotics may improve the clinical efficacy. TRQ may have synergistic effect to antibiotics through bacteriostatic activity and eliminating inflammatory mediators. Its antibacterial activity may be better than some antibiotics and does not increase adverse drug reaction. But all these need new evidences for further investigation.
Introduction
T
Traditional Chinese Herbal Medicine had important antipathogenic activities, and it has been used in many infectious diseases. 7 –10 Tanreqing injection (TRQ) was one of important Traditional Chinese Herbal Medicines. As a compound for injection, it includes extracts from Radix Scutellariae (Scutellaria baicalensis Georgi), Flos Lonicerae (Lonicera japonica Thunb), and Fructus Forsythiae (Forsythia suspensa Thunb). 11 Related meta-analysis reported that TRQ alone or plus antibiotics could significantly improve the clinical efficacy in the treatment of pulmonary infection after malignant solid tumor, hematologic malignancies, and chronic obstructive pulmonary disease (COPD). 12 –14 Pulmonary infection in patients with TB is a double infection and not a single infection as respiratory infection is often in patients with malignant solid tumor, hematologic malignancies, acute exacerbation of COPD (AECOPD), and et al. Can TRQ improve the clinical efficacy for pulmonary infection in patients with TB? In clinical practice, TRQ alone or plus antibiotics is often used in pulmonary infection in patients with TB. Many clinical studies reported that TRQ alone or plus antibiotics might have anti-infective efficacy with low risk of toxicity. 15,16 Unfortunately, these conclusions were different in different trials with limited samples. And their efficacy and safety are still unclear. Up to now, there is a lack of ideal evidences to substantiate the efficacy and safety of the treatment. Therefore, to further reveal its efficacy and safety and provide the optimal evidences for new strategies, the authors systematically reevaluated all related trials.
Materials and Methods
This article followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (PRISMA guidelines). 17 As this study was a meta-analysis of published or unpublished trials, ethical approval was not required.
Searching strategies
Two reviewers (Lian Xiong and Jianbo Yue) independently retrieved trials in Chinese and English database using the search strategy as (Tanreqing OR “Tanreqing injection”) AND (“Tuberculosis” [MeSH] OR Tuberculosis OR TB). All retrievals were implemented using the Mesh and free word. Published trials were retrieved in Embase, PubMed, China National Knowledge Infrastructure Database (CNKI), Chinese Scientific Journals Full-Text Database (VIP), Wanfang Database, China Biological Medicine Database (CBM) (established to January 2017), and Cochrane Central Register of Controlled Trials (CENTRAL, Issue 1 of 12, January 2017). Ongoing trials were retrieved in Chinese clinical trial registry (Chi-CTR), U.S. clinical trials, and World Health Organization International Clinical Trials Registry Platform (WHO-ICTRP) (established to January 2017). Finally, the authors rigorously evaluated similar or related systematic reviews or meta-analysis and selected the trials meeting inclusion criteria from the references.
Inclusion and exclusion criteria
Included trials must meet the following criteria: (1) Pulmonary infection in patients with TB was diagnosed using symptoms, signs, bacteriology, and imaging features 18 and without putting on limitations such as limiting to drug-resistant TB. (2) All patients received anti-TB treatment. The experimental group was TRQ alone or plus antibiotics, and the control group was antibiotics alone. All trials were randomized controlled trials (RCTs). (3) Clinical efficacy was evaluated using the indicators of the overall efficacy, lesion absorption, and bacterial clearance. And safety was evaluated by assessing adverse drug reactions. The duration of follow-ups and types of settings were unrestricted. All indicators were evaluated on 10–14 days after treatment.
Excluded trials meet the following criteria: (1) duplicates; (2) reviews and meeting summaries without data; (3) trials about nonpulmonary TB, pulmonary TB alone, pulmonary TB with COPD, other therapies, and irrelevant themes; (4) case report and case–control trials; and (5) trials without any overall efficacy, lesion absorption, or bacterial clearance.
Selection of trials
Two reviewers (Chengqiong Wang and Yuqin Li) independently selected the potential trials using the inclusion and exclusion criteria. Any disagreements were resolved by discussing with each other or with Ling Chen.
The assessment of methodological bias risk
Two reviewers (Ling Chen and Weijing Zhou) independently evaluated the methodological bias risk of all included trials using the Cochrane evaluation handbook of RCTs (5.1.0). 19 And any disagreement was resolved by discussing with each other or with Ling Chen. The bias parameters were the random sequence generation (selection bias), the allocation concealment (selection bias), the blinding of participants and personnel (performance bias), the blinding of outcome assessment (detection bias), the incomplete outcome data (attrition bias), the selective reporting (reporting bias), and the other bias (to see whether or not the baseline is comparable). The authors judged each item on three levels (“Yes” for low bias, “No” for high risk of bias, and “Unclear”). Then, the authors assessed the trials and categorized them into three levels such as low risk of bias (all the items were categorized “Yes”), high risk of bias (at least one item ranked “No”), and unclear risk of bias (at least one item was “Unclear”). Finally, the authors generated figures and summaries using RevMan version 5.3.5.
Definition of outcome measures
The indicators of overall efficacy included body temperature (normal), clinical symptoms and signs (disappearance or improvement), and chest X-ray (most lesion absorption). Lesion absorption included lesion absorption in chest X-ray imaging. Bacterial clearance included negative sputum culture or smear. Safety evaluated using the adverse drug reactions such as hematologic toxicity, hepatorenal toxicity, gastrointestinal toxicity, drug allergy, and other toxicities.
Data extraction
Two reviewers (Yang Yuan and Quanxian Liu) independently extracted all the data in a standard data extraction form. All the data included the first authors, publishing time, types of disease, demographic characteristics, cases of experimental and control group, usage of TRQ, antibiotics and anti-TB treatments and outcomes which included the overall efficacy, lesion absorption, and bacterial clearance, and adverse drug reactions.
Statistical analysis
Meta-analysis was implemented by two reviewers (Lian Xiong and Jianbo Yue) using Review Manager 5.3 (The Cochrane Collaboration, Oxford, United Kingdom). The risk ratio (RR) and confidence intervals (95% CI) were calculated. Statistical heterogeneity across trials was assessed by chi-square based Q-statistic test, the inconsistency was calculated by I 2, and the significance level was fixed at p < 0.10. When the heterogeneity (p < 0.10; I 2 > 50%) was rejected, the fixed-effects model (FEM) was applied to calculate the RR and the 95% CI. Otherwise, the random effects model (REM) was used to calculate the data. Subgroup analyses were performed according to different types of antibiotics. Funnel plots were used to reveal possible publication bias when the number of trials was 10 or greater. The sensitivity was evaluated through excluding the poor quality trials and trials with overestimated efficacy or underestimated adverse drug reaction. 20 Trials with at least one domain considered as high risk of bias were defined as poor quality trials. The authors draw up criterions as “The trials were identified as over- or underestimated trials, whose results had significant statistical difference and positive effects on publication bias or heterogeneity.”
Results
Search results
The initial database search identified 226 published trials, of which 89 trials remained after duplicates were removed. After eliminating reviews and meeting summaries and irrelevant trials, 35 trials were included. After screening the full texts, the authors included 26 trials meeting the inclusion criteria. And of the 26 trials, 10 trials 21 –30 reported the clinical efficacy of TRQ alone, and 16 trials 31 –46 reported the clinical efficacy of TRQ plus antibiotics (Fig. 1).
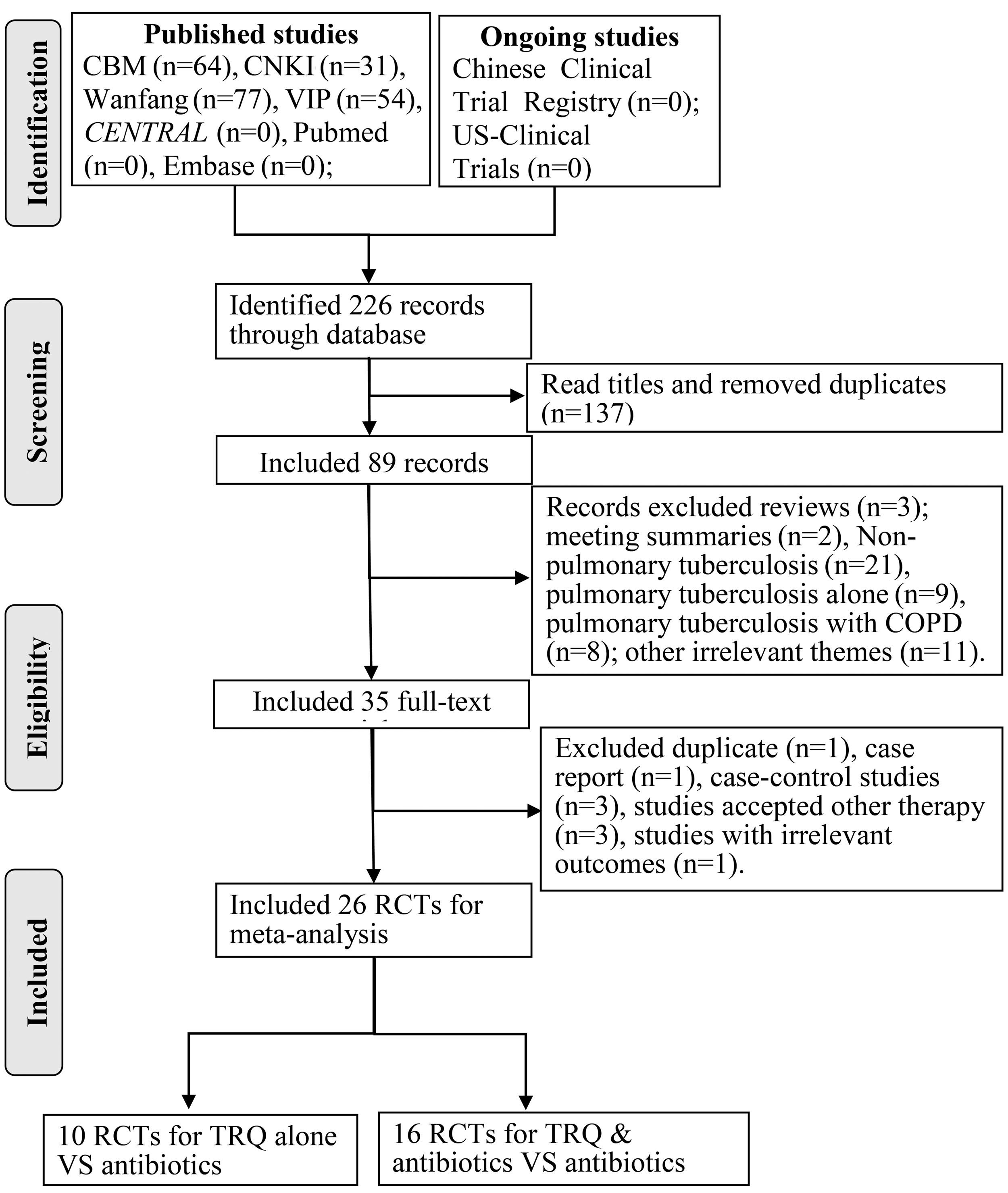
Articles retrieved and assessed for eligibility. CBM, China Biological Medicine Database; CNKI, China National Knowledge Infrastructure Database; RCTs, randomized controlled trials; TRQ, Tanreqing injection.
Characteristics of the included trials
In this meta-analysis, the authors included 26 trials from China. Ten trials 21 –30 with 910 patients reported the clinical efficacy of TRQ alone (“a” in Table 1), patients involved 452 males and 298 females with age ranging from 15 to 80 years. TRQ alone group and antibiotics group each had 455 patients. The usage of TRQ was 20 mL quaque die with 10–14 days' interval by intravenous (IV) injection. Antibiotics included Ceftezole (CTZ), Azithromycin (AZM), Cefuroxime (CFX), Ceftriaxone (CRO), Cefotaxime (CTX), Cefoperazone (CPZ), and Levofloxacin (LVX). Only three trials provided the information about anti-TB regimens such as 2HRZE/4HRE, 2HRZE/4HR, or HRE. Ten trials reported about the overall efficacy, three trials reported the lesions' absorption information, three trials reported about the bacterial clearance conditions, and seven trials reported the gastrointestinal reaction and vascular irritation. None of the trials provided detailed information about evaluation criterion.
AMB, Ambroxol; AZM, Azithromycin; bid, bis in die; CFX, Cefuroxime; CPZ, Cefoperazone; CRO, Ceftriaxone; CTX, Cefotaxime; CTZ, Ceftezole; D/A/F/T, dose/approaches/frequency/times; E, experimental group; HR, Isoniazid (H), Rifampicin (R); HRE, Isoniazid (H), Rifampicin (R), Ethambutol (E); HRZE, Isoniazid (H), Rifampicin (R), Pyrazinamide (Z), Ethambutol (E); HRZE (S), Isoniazid (H), Rifampicin (R), Pyrazinamide (Z), Ethambutol (E), Streptomycin (S); iv, intravenous; LVX, Levofloxacin; MDR-TB, multidrug-resistant TB; M/F, male/female; O1, overall efficacy; O2, lesion absorption; O3, common bacterial clearance; O4, adverse drug reactions; PI, pulmonary infection; qd, quaque die; SCF, Cefoperazone sulbactam; TB, tuberculosis; TRQ, Tanreqing injection; —, unclear.
Sixteen trials 31 –46 with 1494 patients reported the clinical efficacy of TRQ plus antibiotics (“b” in Table 1). Patients included 902 males and 532 females with age ranging from 14 to 89 years. TRQ plus antibiotics group had 748 patients, and antibiotics group had 746 patients, respectively. The usage of TRQ was 20 mL quaque die with 10–14 days' interval by IV injection. Antibiotics included Cefoperazone sulbactam (SCF), Ambroxol (AMB), CRO, and CPZ. Four trials provided information about anti-TB regimens such as HRZE(S) and 2HRZE/4HR. Sixteen trials reported the overall efficacy, six trials reported the lesions' absorption, three trials reported the bacterial clearance, and seven trials reported about the adverse drug reactions such as gastrointestinal reaction and vascular irritation.
Methodological bias of the included trials
In TRQ alone, no trials reported random sequence generation, allocation concealment, or blinding to patients or doctors. Two trials 27,30 had lost to follow-up. None of the included trials had selective reporting. And except for the five trials had baseline comparability; others' baseline comparability was unclear (Fig. 2A).
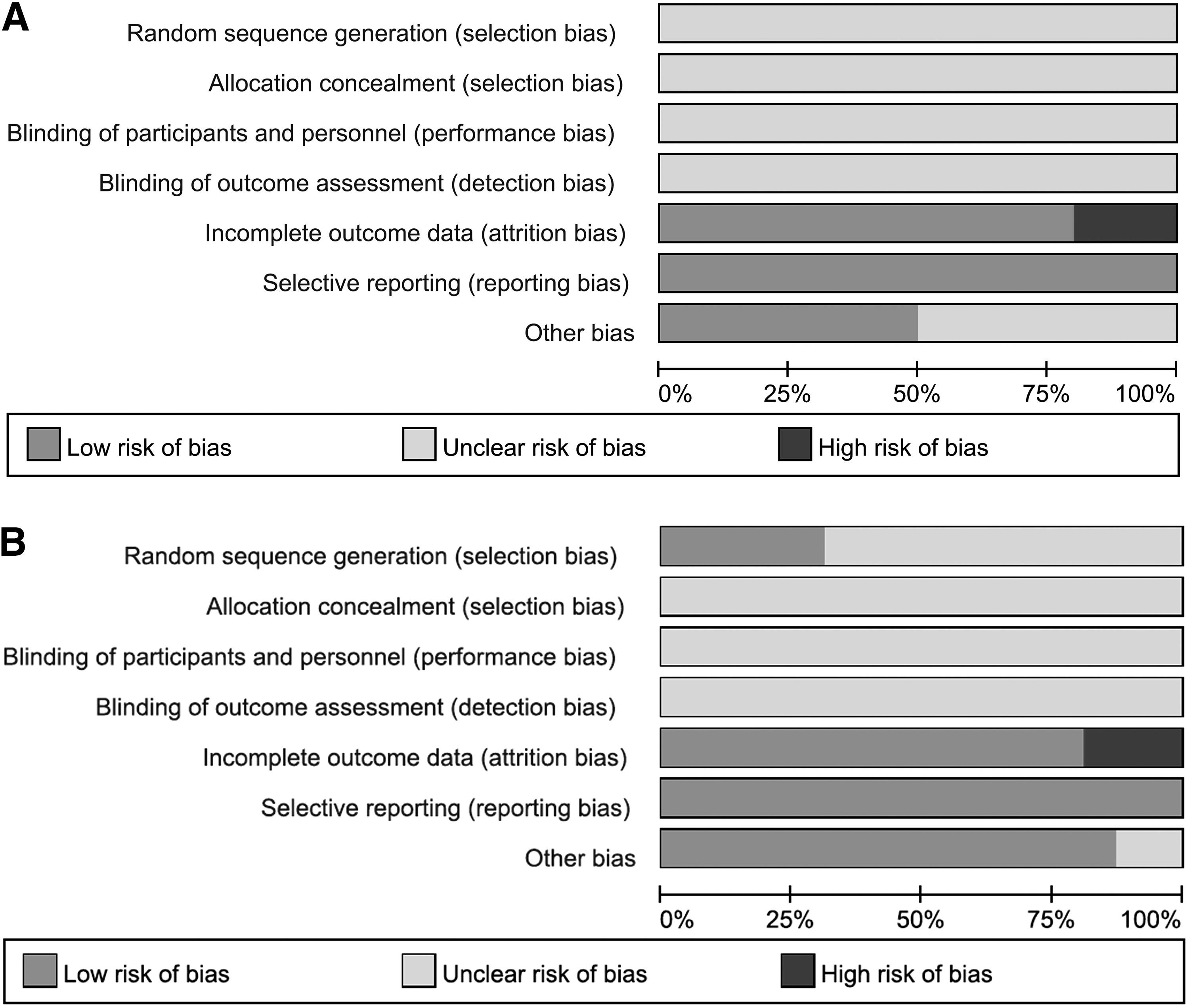
In TRQ plus antibiotics, four trials clearly described randomization methods as random number table 31,34,42 and draw. 36 None of these trials reported random allocation concealment and blinding to patients and doctors. One trial 33 had lost to follow-up. Two trials 34,36 failed to completely report the information about lesions. No trials had selective report. Fourteen trials had baseline comparability, and others' baseline comparability was unclear (Fig. 2B).
Overall efficacy
In 26 trials, 10 trials 21 –30 with 910 cases reported the overall efficacy of TRQ alone (Fig. 3A). Chi-square test showed that there was statistical heterogeneity among the trials (I 2 = 67%, p = 0.001). Therefore, the data were synthesized using REM. Meta-analysis showed that there was no statistical significance between TRQ and antibiotics alone (RR = 1.05, 95% CI 0.99–1.10, p = 0.09) in the overall efficacy.
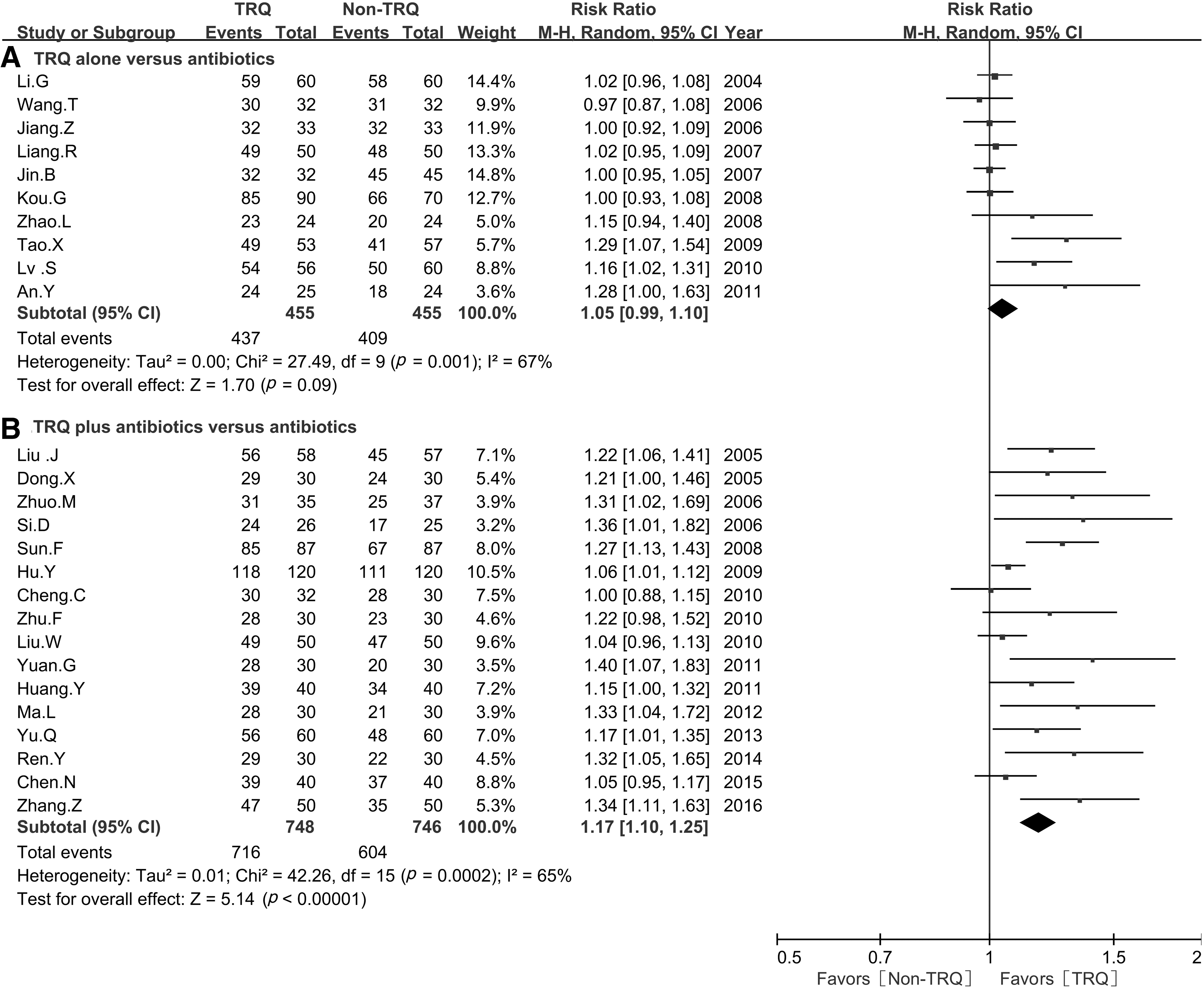
Sixteen trials 31 –46 with 1494 cases reported the overall efficacy of TRQ plus antibiotics (Fig. 3B). There was statistical heterogeneity among the trials (I 2 = 65%, p = 0.0002). Therefore, the data were synthesized using REM. Meta-analysis showed that there was statistical significance between TRQ plus antibiotics and antibiotics alone (RR = 1.17, 95% CI 1.10–1.25, p < 0.00001) in the overall efficacy.
Lesion absorption
In 10 trials, 3 trials 22–23,25 with 263 cases reported the lesion absorption of TRQ alone (Fig. 4A). There was no statistical heterogeneity among the trials (I 2 = 1%, p = 0.36). Therefore, the data were synthesized using FEM. Meta-analysis showed that there was no statistical significance between TRQ and antibiotics alone in lesion absorption (RR = 0.98, 95% CI 0.89–1.08, p = 0.67).
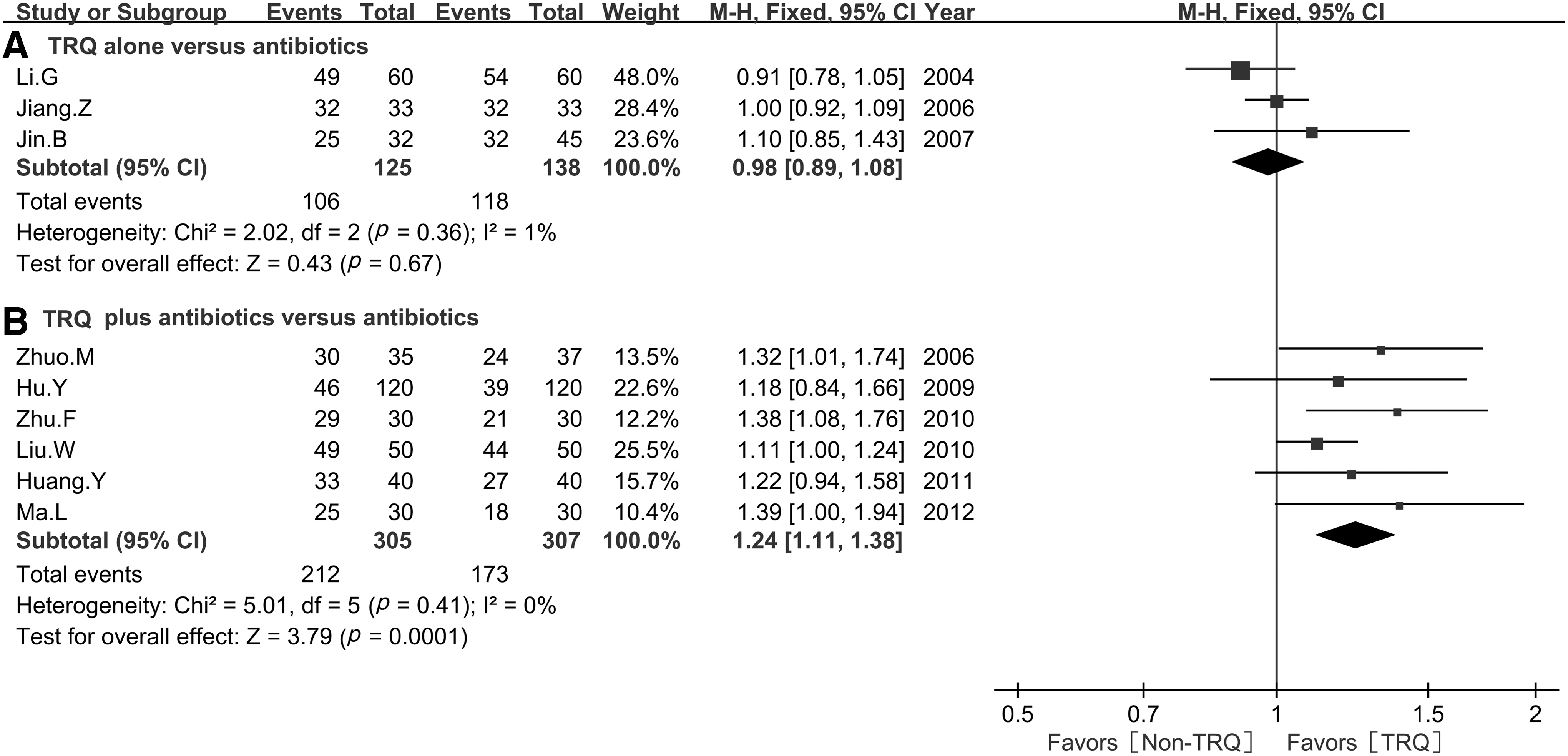
In 16 trials, 6 trials 34,35,38,39,45,46 with 612 cases reported the lesion absorption of TRQ plus antibiotics (Fig. 4B). There was no statistical heterogeneity among the trials (I 2 = 0%, p = 0.41). Therefore, the data were synthesized using FEM. Meta-analysis showed that there was statistical significance between TRQ plus antibiotics and antibiotics alone in lesion absorption (RR = 1.24, 95% CI 1.11–1.38, p = 0.0001).
Bacterial clearance
In 10 trials, 3 trials 27,29,30 with 228 cases reported the bacterial clearance of TRQ alone (Fig. 5A). There was no statistical heterogeneity among the trials (I 2 = 31%, p = 0.23). Therefore, the data were synthesized using FEM. Meta-analysis showed that there was statistical significance between TRQ and antibiotics alone in bacterial clearance (RR = 1.36, 95% CI 1.09–1.70, p = 0.007).
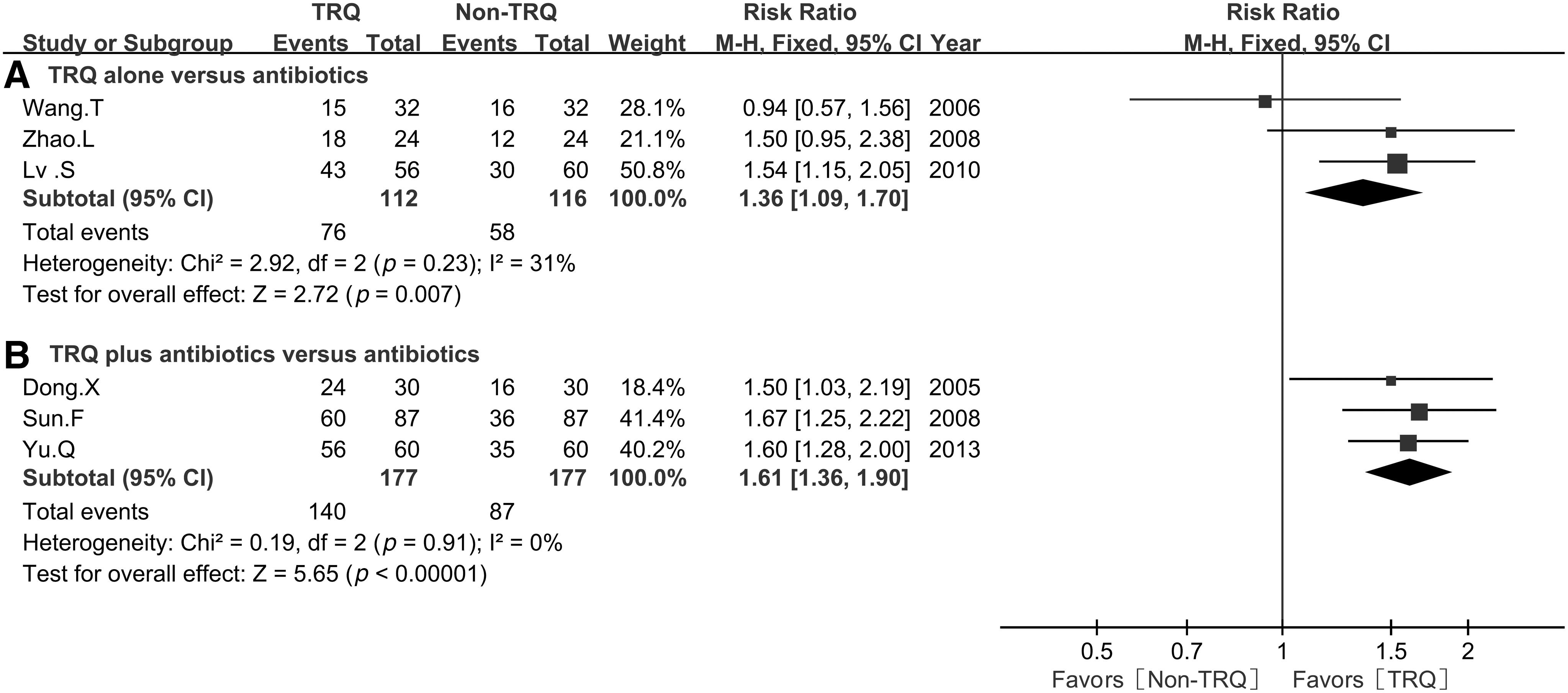
In 16 trials, 3 trials 33,41,42 with 354 cases reported the bacterial clearance of TRQ plus antibiotics (Fig. 5B). There was no statistical heterogeneity among the trials (I 2 = 0%, p = 0.91). Therefore, the data were synthesized using FEM. Meta-analysis showed that there was statistical significance between TRQ plus antibiotics and antibiotics alone in bacterial clearance (RR = 1.61, 95% CI 1.36–1.90, p < 0.00001).
Adverse reaction
In TRQ versus antibiotics alone, only one trial 22 reported that antibiotics group had two cases of slight stomach discomfort and one case of vascular irritation. In TRQ plus antibiotics versus antibiotics alone, only one trial 37 reported that antibiotics group had two cases of slight stomach discomfort. None of the trials reported that TRQ alone or plus antibiotics had hematologic toxicity, hepatorenal toxicity, or drug allergy.
Subgroup analysis
The authors performed subgroup analysis to reveal the influence of different antibiotics on the overall efficacy between TRQ and antibiotics alone (Table 2). First, subgroup analysis showed that there was only statistical significance between TRQ and CPZ group in the overall efficacy (RR = 1.29, 95% CI 1.07–1.54, p = 0.006).
AMB, Ambroxol; AZM, Azithromycin; CFX, Cefuroxime; CI, confidence interval; CPZ, Cefoperazone; CRO, Ceftriaxone; CTX, Cefotaxime; CTZ, Ceftezole; LVX, Levofloxacin; REM, random-effects model; RR, risk ratio; SCF, Cefoperazone sulbactam; SM, statistical method; TRQ, Tanreqing injection.
The authors performed subgroup analysis to reveal the influence of different antibiotics on the overall efficacy between TRQ plus antibiotics and antibiotics alone. Subgroup analysis showed that there were statistical significances between TRQ plus SCF and SCF group (RR = 1.15, 95% CI 1.01–1.30, p = 0.03), TRQ plus CRO and CRO (RR = 1.17, 95% CI 1.07–1.28, p = 0.0006), TRQ plus AZM and AZM (RR = 1.27, 95% CI 1.13–1.43, p<0.0001), and TRQ plus CPZ and CPZ (RR = 1.22, 95% CI 1.06–1.41, p = 0.006).
Publication bias
In TRQ versus antibiotics alone, the funnel plots were significantly asymmetric in the overall efficacy. There was publication bias in them, and the result was underestimated in one trial 23 (Fig. 6A). In TRQ plus antibiotics versus antibiotics alone, the funnel plots were also significantly asymmetric in the overall efficacy. There was publication bias in them, and the results were underestimated in four trials 31,32,34,37 (Fig. 6B).

Sensitivity analysis
In TRQ versus antibiotics alone, two trials with poor quality 27,30 had lost to follow-up. The sensitivity was evaluated through excluding the poor quality trials. Except for the bacterial clearance, the overall efficacy had good consistency before and after excluding the poor trials (“a” in Table 3). There was heterogeneity in bacterial clearance and overall efficacy, and publication bias in overall efficacy. The sensitivity was evaluated through excluding the trials with overestimated efficacy. Except for the bacterial clearance, other results had good consistency (“b” in Table 3).
Poor*: Poor quality trial that had at least one domain considered as high risk of bias; Over*: Overestimated trials when results of which had statistical difference and positive effects on publication bias and heterogeneity.
CI, confidence interval; FEM, fixed-effects model; REM, random-effects model; RR, risk ratio; SM, statistical method; TRQ, Tanreqing injection.
In TRQ plus antibiotics versus antibiotics alone, one trial 33 had lost to follow-up, and one trial 34 failed to completely report the information about lesion absorption. All results had good consistency before and after excluding the poor quality trials (“a” in Table 3). There were heterogeneity and publication bias in overall efficacy. The results had good consistency before and after excluding the trials with overestimated efficacy (“b” in Table 3). In all, this meta-analysis had good stability.
Discussion
In this meta-analysis, 26 trials with 2404 patients assessed the clinical efficacy and safety of TRQ alone or plus antibiotics in pulmonary infection in patients with TB. Ten trials 21 –30 with 910 patients reported the clinical efficacy of TRQ alone. Antibiotics included the CTZ, AZM, CFX, CRO, CTX, CPZ, and LVX. Patients involved 452 males and 298 females with age ranging from 15 to 80 years. Sixteen trials 31 –46 with 1494 patients reported the clinical efficacy of TRQ plus antibiotics. Patients involved 902 males and 532 females with age ranging from 14 to 89 years. Antibiotics included the SCF, AMB, CRO, and CPZ. The usage of TRQ was 20 mL quaque die with 10–14 days' interval using IV injection in most trials. The overall efficacy, lesion absorption, bacterial clearance, and adverse drug reactions were evaluated at 10–14 days after treatment, respectively.
TRQ is often used in infectious diseases, especially in secondary infection. Ai et al. 12 meta-analysis had shown that TRQ alone could improve the clinical efficacy; its symptom relief effect and bacterial clearance rate were as good as those of the antibiotics in pulmonary infection after hematologic tumor. Results indicated that TRQ might have the same clinical effectiveness as antibiotics. Can TRQ improve the clinical efficacy for pulmonary infection in patients with TB? In this meta-analysis, the authors included 10 trials with 910 patients to reveal the clinical efficacy of TRQ alone in pulmonary infection in patients with TB. Meta-analysis showed that TRQ had the same overall efficacy, lesion absorption, and bacterial clearance as antibiotics alone. Subgroup analysis showed that TRQ had the same overall efficacy as CTZ, AZM, CFX, CRO, CTX, and LVX. However, it was interesting that TRQ had better overall efficacy compared with cefoperazone. The overall efficacy was underestimated. This was beneficial to the conclusion in which TRQ improves the overall efficacy.
There were limited studies and sample sizes in lesion absorption and bacterial clearance, which might lead to inadequate assessment. Except for the bacterial clearance, other results had good robustness. Results further revealed that TRQ might have antibacterial activity as antibiotics in pulmonary infection in patients with TB. And Wang et al. 47,48 had reported that TRQ had outstanding bacteriostatic activity against Staphylococcus aureus and Pseudomonas aeruginosa in vitro. In all, TRQ has the same overall efficacy as antibiotics. Its antibacterial activity may be better than some antibiotics. But this needs to be confirmed by new evidences. Can TRQ plus antibiotics improve the clinical efficacy for pulmonary infection in patients with TB? Related meta-analysis 49 –51 had shown that TRQ combined with antibiotic could improve the clinical curative effect in pulmonary infection after malignant solid tumor, hematologic malignancies, and AECOPD. In this meta-analysis, the authors included 16 trials with 1494 patients to reveal the clinical efficacy of TRQ plus antibiotics in pulmonary infection in patients with TB. Meta-analysis results showed that TRQ plus antibiotics could increase the lesion absorption and bacterial clearance rate and improve the overall efficacy. Subgroup analysis showed that TRQ plus SCF, AMB, CRO, or CPZ could all improve the overall efficacy. Overall efficacy was underestimated, and the results had good robustness, which was beneficial to the conclusion. However, there were also limited studies and sample sizes, and most studies had unclear risk of bias. All these might lead to inadequate assessment of the results. Related meta-analysis 52 had shown that TRQ could improve the clinical efficacy and relieve the clinical signs or symptoms in radiation pneumonitis. Other meta-analysis 53 had shown that compared with Indomethacin, Shuanghuanglian, and Xinhuang Pian, TRQ had a strong antipyretic effect in advanced malignant tumor. Other studies 54 –56 reported that TRQ could inhibit inflammation through eliminating the inflammatory mediators such as nitric oxide (NO), interleukin-1β (IL-1β), interleukin-6 (IL-6), cytokine-induced neutrophil chemoattractant 1 (CINC-1), and tumor necrosis factor and tumor necrosis factor-α (TNF-α). Results indicated that TRQ had outstanding anti-inflammatory activity through downregulating inflammatory mediators. In all, the authors believe that TRQ plus antibiotics may improve the clinical efficacy in pulmonary infection in patients with TB. This meta-analysis further indicated that TRQ might have synergistic effect to antibiotics through bacteriostatic activity and eliminating inflammatory mediators. However, whether TRQ has bacteriostatic activity against Mycobacterium TB or whether TRQ can reduce the dosage of antibiotics needs to be confirmed by new evidences.
As an important Traditional Chinese Herbal Medicine, can TRQ result in an increased rate of the adverse drug reactions? In this meta-analysis, only two trials 22,37 reported that antibiotics group experienced a slight stomach discomfort and vascular irritation. None of the trials reported that TRQ alone or plus antibiotics experienced hematologic toxicity, hepatorenal toxicity, or drug allergy. Related meta-analysis 12,51 also reported that patients receiving TRQ treatment experienced a slight stomach discomfort and vascular irritation. And other meta-analysis 49 reported that patients receiving TRQ treatment had increased risk of rash and thrombocytopenia. But there was no statistical difference between the TRQ treatment and non-TRQ treatment groups. Current evidences showed that TRQ did not increase the adverse drug reactions. But most trials lack a report about the adverse drug reactions. Therefore, the treatment's safety needs to be further investigated with new evidences.
Limitations
There were some limitations in this study. First, Chinese and English database were retrieved, but not Japanese or Korean databases; all included trials were published in China. Second, only four trials clearly described the randomization method. Most trials had unclear risk of bias. Three trials failed to follow-up, and one trial had incomplete outcome data. Third, none of the trials provided detailed information about evaluation criterion, follow-up, and recurrence. Finally, there were limited trials and sample sizes for lesion absorption and bacterial clearance. All the factors may result in an inadequate assessment of the clinical efficacy and safety.
Conclusion
The available evidences indicate that TRQ plus antibiotics may improve the clinical efficacy in pulmonary infection in patients with TB. TRQ does not seem to increase the rate of adverse drug reactions. TRQ might have synergistic effect to antibiotics through bacteriostatic activity and eliminating inflammatory mediators. However, whether TRQ has bacteriostatic activity against Mycobacterium TB or whether TRQ can reduce the dosage of antibiotics is unclear. All the above-mentioned evidences still need to be confirmed and further investigated with new evidences. However, some limitations and poor quality may result in an inadequate assessment of the clinical efficacy and safety. The results need to be further confirmed using large sample RCT or real-world trials with standardized evaluation criterion.
Footnotes
Acknowledgments
The National Natural Science Foundation of China grant no. 81760003 was provided for the performance of this study. Many thanks to Zheng Xiao, Evidence-Based Medicine Center, MOE Virtual Research Center of Evidence-based Medicine at Zunyi Medical College, Affiliated Hospital of Zunyi Medical College, for his valuable scientific suggestions in the search strategy. The authors also thanked the anonymous referees for their helpful comments and advice, which greatly improved the quality of this review. All supporting documentations are under the permission of all the included authors.
Author Disclosure Statement
All authors declare no conflicts of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.