
Abstract
Objective:
Constipation is quite common and has impact on life quality in the elderly diabetic patients; therefore it is important to seek better treatments. The aim of this study is to evaluate the effect of Chang Run Tong (CRT) decoction on constipation in elderly diabetic patients in comparison with the effect of Macrogol 4000 powder (Forlax).
Design:
This study was designed as a prospective study consisting of two parallel arms: CRT group and Forlax group.
Settings/Location:
The study was conducted in China-Japan Hospital.
Subject interventions:
Eighty elderly diabetic patients with constipation were evaluated, among them 52 patients were treated with CRT and 28 patients were treated with Forlax.
Outcome measures:
The patients were interviewed for Bristol stool scale, spontaneous complete bowel movements (SCBM) and symptoms of defecation feeling, defecation weakness, feeling of incomplete evacuation, bloating, and flatulence at different time points. The changes of all above parameters from treatment for 2 and 4 weeks and follow-up for 1 and 2 months with reference to the baseline (before treatment) were compared between CRT and Forlax treatments. The treatment efficiency was evaluated and compared between two different treatments.
Results:
For the improvement of Bristol stool scale, SCBM and feeling of incomplete evacuation, CRT was significantly better than Forlax at different time points (p < 0.01, p < 0.001). For the symptoms of defecation feeling, defecation weakness, bloating, and flatulence, CRT was significantly better than Forlax for follow-up improvement (p < 0.01, p < 0.001); whereas no difference was found at other time points of the treatment (p > 0.05). Furthermore, CRT had a significantly better treatment efficiency than Forlax (p < 0.001).
Conclusions:
Both CRT and Forlax treatment could effectively improve bowel habits and symptoms of constipation in elderly diabetic patients. CRT was better than Forlax to treat constipation in elderly diabetic patients and had better follow-up improvement after stopping drugs.
Introduction
I
Normally there is no specific treatment for diabetes-associated chronic constipation in old people; these patients are generally treated in the same way as general old people with chronic constipation. Usually the treatment initiates with bulk-forming agents such as fiber laxatives. 9 For patients with lack of response to a bulking agent, an osmotic agent such as lactulose 10 and polyethylene glycol 11 could be selected and followed by stimulants. 12 Finally, some agents such as chloride channel activators 13 or 5-HT4 agonist 14 may be selected for severe cases. It is well known that constipation is difficult to treat and has a high recurrence rate. 15 Furthermore, a lot of patients are not satisfied with these symptomatic treatments. A large number of clinical data have shown that Chinese herbal medicine has good clinical effects on constipation. 16 Therefore, many patients with constipation seek help from Traditional Chinese Medicine (TCM). 17
Through clinical observation (Zhao et al., unpublished data), it has been found that Chang Run Tong (CRT) decoction produced by China-Japan Hospital could effectively treat constipation in elderly. Furthermore, in our previous study we have demonstrated that CRT could partly restore the colonic remodeling in streptozotocin (STZ)-induced diabetic rats. 18 Diabetes-induced colon remodeling is likely to be closely related to diabetic constipation. 19 Therefore, CRT may be a better treatment for constipation in elderly patients with diabetes. The aim of this study is to evaluate the clinical effect of CRT on constipation in elderly patients with diabetes. Macrogol 4000 powder (Forlax) was used as control drug in this study.
Materials and Methods
Participants
Ethics approval from the Ethics Committee of China-Japan Hospital was obtained for this study. The patients with diabetes diagnosed as constipation at the Department of Chinese Medicine Geriatrics, China-Japan Hospital from March 2010 to June 2017 were selected. Among those patients who met the following criteria of diagnosis, inclusion and exclusion were included in the study. All patients have signed the informed consent.
Diagnostic criteria
The diagnostic criteria of diabetes and constipation were summarized in Table 1.
TCM, Traditional Chinese Medicine.
All cases in this study have been diagnosed as diabetes. Insulin injection or oral administration of hypoglycemic agents such as sulfonylureas or biguanide has been used to control diabetes. Constipation should meet the Rome II diagnostic criteria. 20
Furthermore, the patients were also meeting the requirements of diagnostic criteria for constipation in TCM theory. 16
Design of the study
This study was designed as a prospective study consisting of two parallel arms: CRT group and Forlax group.
Inclusion criteria
Patients were included if (1) they met all the criteria of diabetes; (2) they met all the diagnostic criteria of Rome II and TCM theory for constipation; (3) they had stayed without the use of any laxative for 2 weeks; (4) they were without bowel organic and obstructive disease to lead constipation showed by colonoscopy; (5) they were without serious diseases of heart, liver, and kidney; (6) they were able to walk on their own and coordinate the examination and treatment; and (7) they were willing to participate in this study and sign the informed consent.
Exclusion criteria
Patients were excluded if they met one or more of the following: (1) unwilling to participate in this study and sign the informed consent; (2) have cancer or acute asthma; (3) have bowel organic and obstructive disease; (4) currently using other treatment for constipation (drug or nondrug); (5) pregnancy or breast-feeding; (6) serious adverse events; (7) have severe concomitant diseases during the experiment; and (8) did not complete the follow-up observation.
Drugs
CRT decoction
CRT is composed of Herba Cistanches, Semen arecae prepareta, Fructus aurantii immaturus, Radix cyathulae, Fructus cannabis, Radix angelicae sinensis, Semen persicae, and Rhizoma cimicifugae. It was provided by China-Japan Hospital, The Ministry of Health of the People's Republic of China. CRT was orally used two times per day, 66.5 g per time. The composition, usage, and action of each herb are summarized in Table 2.
TCM, Traditional Chinese Medicine.
Forlax (Macrogol 4000 powder)
Forlax was dissolved in water and orally used two times per day, 10 g per time.
Outcome measures
All patients were treated with CRT or Forlax for 4 weeks and then followed up observation for 2 months. The researchers interviewed patients before treatment (B-T, baseline), 2 weeks treatment (T-2w, within treatment), 4 weeks treatment (T-4w, end of treatment), 1 month after follow-up (F-1m, within follow-up), and 2 months after follow-up (F-2m, end of follow-up). The Bristol stool scale, spontaneous complete bowel movements (SCBM), and observing symptoms (yes/no) including defecation feeling, defecation weakness, feeling of incomplete evacuation, bloating, and flatulence were considered as primary measures. The treatment efficiency consideration according to Bristol stool scale was considered as secondary measure. All these parameters were also considered with gender factor taken into account. The recorded and calculated values were averaged for each time points of observation.
Bristol stool scale 37,38 is a seven-point scale according to cohesion and surface of the stool character as follows: (1) Separated hard lumps (like nuts); (2) Sausage-shaped, but lumpy; (3) Like a sausage or snake, but with cracks on its surface; (4) Like a sausage or snake, and smooth and soft; (5) Soft blobs with a clear-cut edge; (6) Fluffy pieces with ragged edges and mushy; and (7), Watery with no solid pieces.
The number of daily bowel movements was recorded on a subject daily card. Two defecation intervals <10 min were considered as one time of defecation. The patients also recorded the stool character on their diary cards. SCBM is often used to observe the improvement in spontaneous bowel movements of constipation patients after getting treatment. 39
Treatment efficiency consideration
Effective cases were defined as such if the Bristol stool scale score was over 4 (including 4) or at least increasing one point of Bristol stool scale compared with the value of B-T.
Statistical analysis
The software package SigmaPlot version v11.0 (Jandel Scientific, Erkrath, Germany) was used for statistical analysis. The comparison of all outcome measures including Bristol stool scale, SCBM, defecation feeling, defecation weakness, feeling of incomplete evacuation, bloating, and flatulence in different time points was made between two different groups. The improvement of different above-mentioned parameters at different time points of treatment and follow-up in relation to B-T was also compared between two groups. The comparison was also considered the effect of gender differences. The difference was analyzed by two-way analysis of variance or t-test. The sample size analysis was performed. The results were regarded as significant when p < 0.05.
Results
Patients' data
Totally 80 patients who met the inclusion and exclusion criteria of diagnosis were included in the study. Among them, 52 patients (29 male and 23 female) were treated with CRT and 28 patients (15 male and 13 female) were treated with Forlax. All patients have signed the informed consent. The main demographic data of the patients were summarized in Table 3. As we did not find gender difference for the results shown below, we compared the average results from mix gender between CRT and Forlax groups.
SD, standard deviation.
Bristol stool scale comparison
Bristol stool scale comparison is shown in Figure 1A. The average of Bristol stool scale at B-T did not differ between CRT and Forlax groups (p > 0.05). Compared with B-T, it increased at different time points both for CRT group (p < 0.001) and Forlax group (p from 0.033 to <0.001). This indicated that the Bristol stool scale considerably improved after treatment with both CRT and Forlax. For comparison, CRT is better than Forlax to have high Bristol stool scale at different time points (T-2w, T-4w and F-2m, p < 0.001; F-1m, p = 0.007). Relative change of Bristol stool scale with reference to B-T is shown in Figure 1B. It was also shown that CRT is better than Forlax to improve the Bristol stool scale at different time points (p < 0.05).
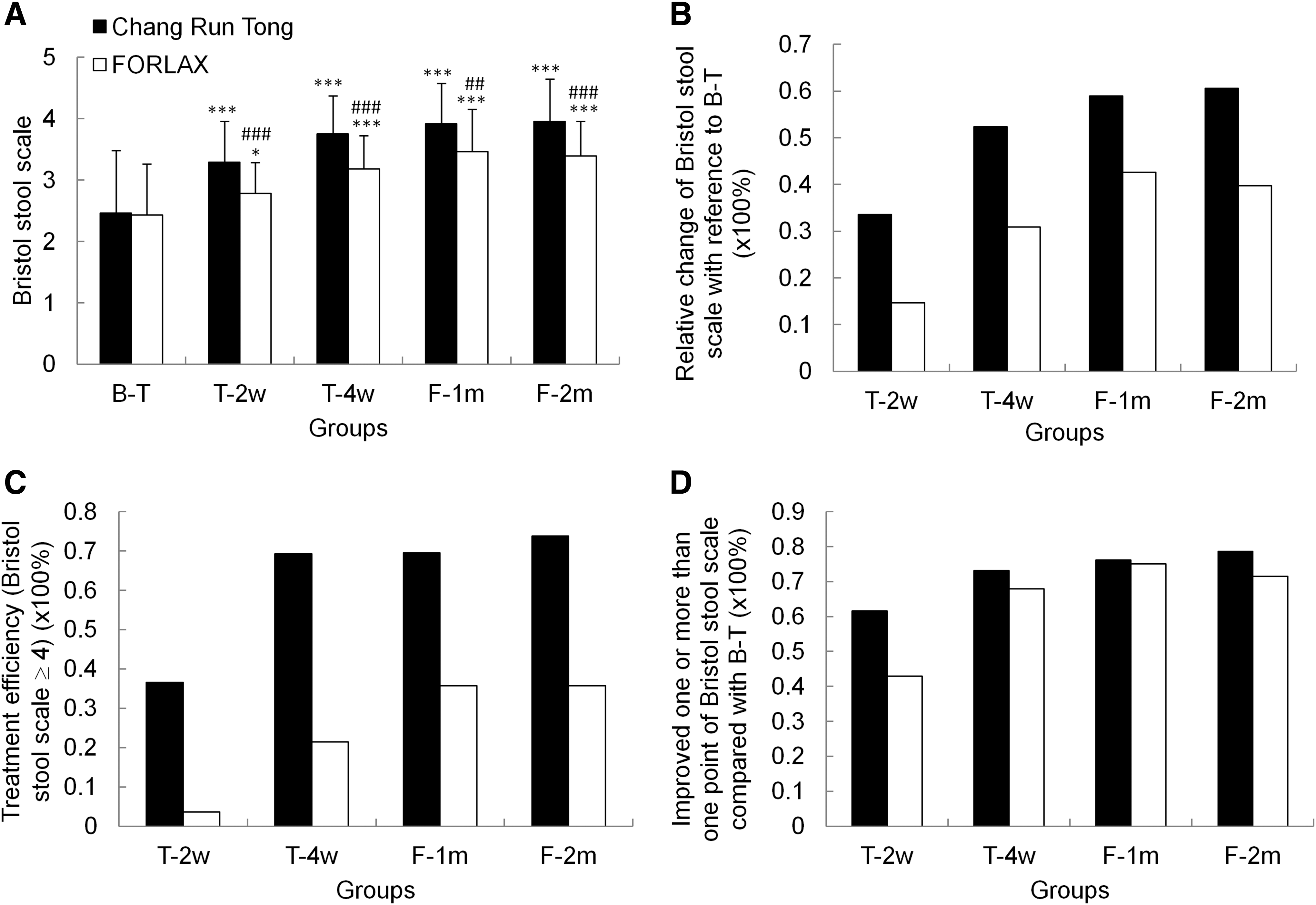
Comparison of Bristol stool scale at different time points and treatment efficiency. Compared with B-T, both CRT and Forlax significantly improved Bristol stool scale in T-2w, T-4w, F-1m, and F-2m
The efficiency percentage of treatment at different time points is defined by the Bristol stool scale equal to and greater than 4, or increasing one point compared with B-T. If consideration of treatment efficiency is based on the Bristol stool scale equal and over 4, the efficiency percentage of CRT was 36%, 69%, 69%, and 74% for T-2w, T-4w, F-1m and F-2m, whereas the efficiency percentage of Forlax was 3%, 21%, 35%, and 35% for T-2w, T-4w, F-1m, and F-2m respectively (Fig. 1C). However, if the consideration of treatment efficiency is based on increasing one point of Bristol stool scale compared with B-T, the efficiency percentage of CRT was 62%, 73%, 76%, and 79% for T-2w, T-4w, F-1m, and F-2m, whereas the efficiency percentage of Forlax was 43%, 68%, 75%, and 71% for T-2w, T-4w, F-1m, and F-2m respectively (Fig. 1D). It indicated that CRT had higher treatment efficiency percentage than Forlax.
SBCM comparison
SBCM comparison is shown in Figure 2A. The average number of SBCM at B-T did not differ between CRT and Forlax groups (p > 0.05). Compared with B-T, it increased at different time points both for CRT group (p < 0.001) and for Forlax group (p from 0.02 to <0.001). This indicated that the number of SBCM was also considerably improved after treatment with both CRT and Forlax. For comparison, CRT was better than Forlax to have high number of SBCM at different time points (T-2w, p = 0.008; T-4w, F-1m and F-2m, p < 0.001). Relative change of the number of SBCM with reference to B-T is shown in Figure 2B. It was also shown that CRT is better than Forlax to improve the number of SBCM at different time points (p < 0.01, p < 0.001).

Comparison of SCBM at different time points. Compared with B-T, both CRT and Forlax significantly improved SCBM in T-2w, T-4w, F-1m, and F-2m
Comparison of different symptoms
The defecation feeling, incomplete evacuation, defecation weakness, sensation of bloating and flatulence were compared at time points of T-2w, T-4w, F-1m, and F-2m with B-T for both CRT and Forlax. Generally, CRT significantly improved different symptoms at different time points (Figs. 3 and 4, p < 0.01, p < 0.001) whereas Forlax improved some symptoms at some time points with big variations. The significant differences in regarding to Forlax were: for defecation feeling (Fig. 3A, B, T-4w: p < 0.05; F-1m: p < 0.001); for incomplete evacuation (Fig. 3C, D, T-2w, F-1m and F-2m: p < 0.05); for defecation weakness (Fig. 3E, F, F-1m: p < 0.001; F-2m: p < 0.01); for sensation of bloating (Fig. 4A, B, T-4w: p < 0.001; F-1m: p < 0.01); and for flatulence (Fig. 4C, D, T2-w: p < 0.01; T-4w: p < 0.001).

Comparison of defecation feeling, feeling of incompleteness of evacuation and defecation weakness at different time points. Compared with B-T, CRT significantly improved defecation feeling
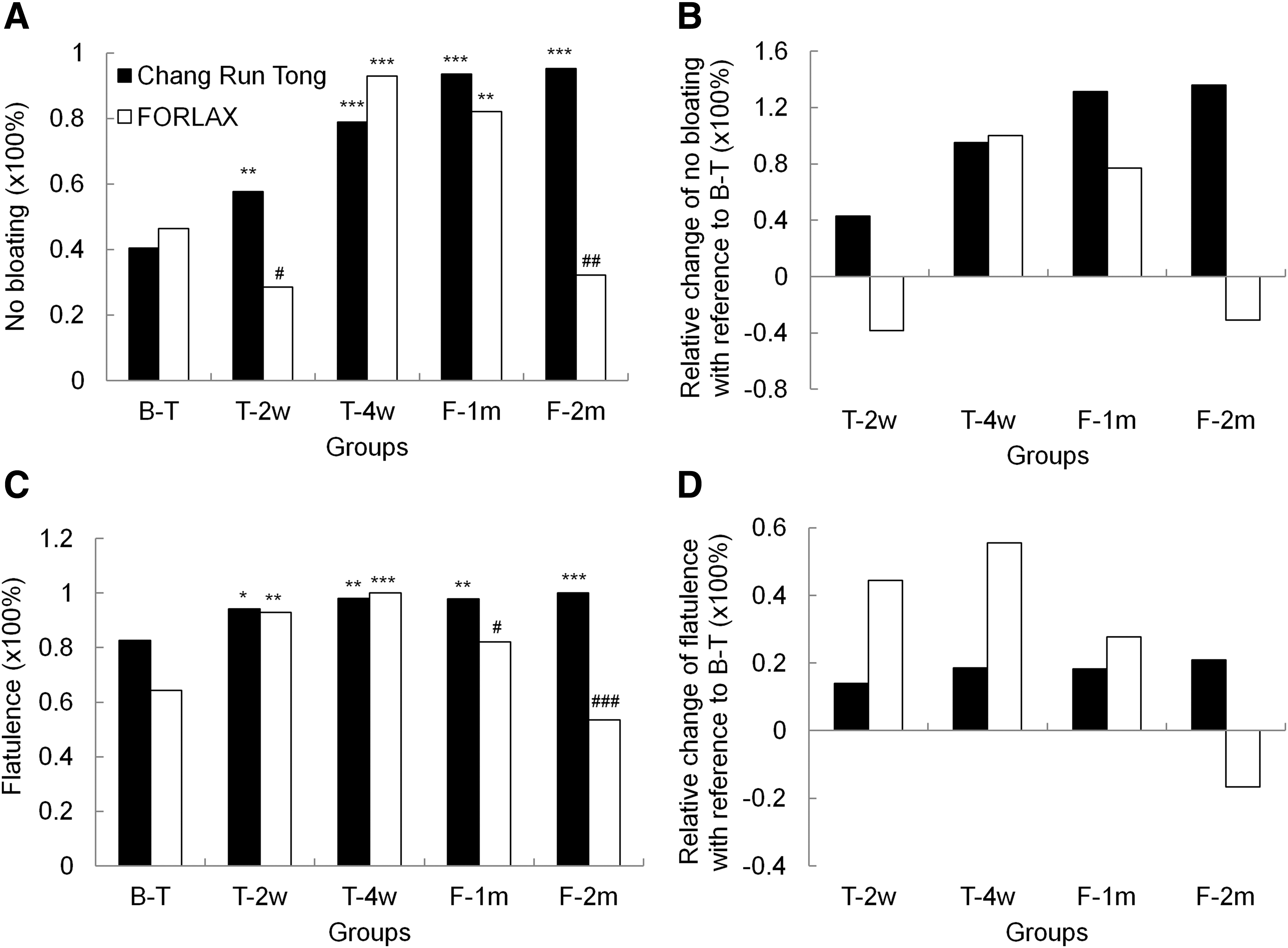
Comparison of sensation of bloating and flatulence at different time points. Compared with B-T, CRT significantly improved sensation of bloating
In comparison between CRT and Forlax groups, the difference was found for the symptom of incomplete evacuation (Fig. 3C, D) at time points of T-4w (p = 0.003), F-1m (p < 0.001), and F-2m (p = 0.002). It indicated that CRT was better than Forlax to improve incomplete evacuation in patients. Furthermore, CRT was better than Forlax to have follow-up improvement for defecation feeling (Fig. 3A, B, p < 0.001), defecation weakness (Fig. 3E, F, p = 0.002), bloating (Fig. 4A, B, p = 0.002) at time point of F-2m, and flatulence (Fig. 4C, D) at time points of F-1m (p = 0.016) and F-2m (p < 0.001).
Discussion
The main findings obtained from this study were as follows: (1) CRT was better than Forlax at different time points for the improvement of Bristol stool scale, SCBM and feeling of incomplete evacuation. (2) For the symptoms of defecation feeling, defecation weakness, bloating, and flatulence, CRT treatment obtained better follow-up improvement in comparison with Forlax. (3) For treatment efficiency, CRT was significantly better than Forlax. Constipation has been cited as the most common GI complaint of diabetic patients. 4 When severity is taken into consideration, constipation is the most severe symptomatic problem in diabetic patients. 40 Constipation has significant impact on the quality of life of involved people, with psychological and social consequences. 41,42 Therefore, it is important to find a better way to treat constipation in elderly diabetic patients.
On the basis of food and dietary change with exercise and lifestyle change, laxative is the first choice for chronic constipation in diabetic patients. 8 Among laxatives, Forlax is often chosen. 8 Forlax has been widely used to treat constipation both in children and adults. 43 –45 Recently, it has been reported that Forlax had good clinical tolerance in elderly constipated patients with a better clinical efficacy in comparison with lactulose. 46 The polyethylene glycol has been considered as first-line treatment for functional constipation both short- and long term. 45 It has been more recently demonstrated that Forlax is effective and safe to treat constipation in diabetic patients. 47 In this study we found that Forlax could effectively and safely improve Bristol stool scale, SCBM, and different symptoms of constipation in elderly diabetic patients.
In comparison with Forlax, CRT was more effective, especially it did achieve good follow-up improvement after stopping drugs. Why CRT has better effect on constipation in elderly diabetic patients than Forlax? According to TCM theories, the chronic constipation, especially in the elderly, is mainly due to “deficiencies in blood and body fluids.” Therefore, it is believed by TCM physicians that TCM drugs possessed actions of “replenishing blood and nourishing body fluids” and are useful to treat chronic constipation especially in elderly diabetic patients. The composition of CRT includes different Chinese herbs (Table 2). From the TCM point of view, different herbs have different effects (Table 2). 21,23,25,29,31,33,35 Combination of Herba Cistanches and Radix angelicae sinensis can lubricate the bowel and improve the movement. Combination of Fructus aurantii immaturus, Semen persicae, Semen arecae prepareta, and Radix cyathulae can remove the turbid qi in the bowel and promote stool flow downward. Furthermore, combining Rhizoma cimicifugae with Fructus aurantii immaturusm, Semen arecae prepareta, Semen persicae, and Radix cyathulae can ascend the clear, descend the turbid, and regulate function of qi. Therefore, CRT is based on the principle of warming the yang and invigorating the spleen, regulating qi and resolving food stagnancy, and lubricating the bowel and descending the turbid. All components together can achieve the CRT efficacy of reinforcing insufficiency, reducing excessiveness, lubricating the bower, and relieving constipation. The modern pharmacological studies have shown that different herbs have different effects on GI tract and other systems in the body (Table 2). 22,24,26 –30,32,34,36 Therefore, CRT could effectively regulate GI motility and improve the symptoms in patients with constipation.
Long-term hyperglycemia could induce the formation and accumulation of advanced glycation end products (AGEs) that play an important role in diabetic autonomic neuropathy (DAN). 48 It is well known that the contribution of diabetes to constipation is closely associated with DAN. 49 Our previous studies have demonstrated that experimental diabetes could induce colon morphological and biomechanical remodeling, 19 and the expressions of AGEs and transforming growth factor (TGF)-β1 and their receptors in the colonic wall were associated with diabetes-induced colonic remodeling. 50 Such remodeling may play an important role in diabetic GI complications including constipation. 51 From previous study we have also demonstrated that CRT could partly restore the morphometric and biomechanical remodeling of colon in STZ-induced diabetic rats. 50 Furthermore, CRT could inhibit the overexpression of AGE and TGF-β1 and their receptors in the colon of diabetic rats. 50 Therefore, CRT had better effect for improving symptoms of constipation in elderly diabetic patients.
There are some limitations to this study. First, we did not have placebo control in our study. However, through this comparison study we did show that CRT was better than Forlax to improve the signs and symptoms of constipation in elderly diabetic patients. Second, this study involved a relatively small population of elderly diabetic patients with constipation. Third, the effect of individual component of CRT on diabetes-induced colon remodeling was not investigated in this study. In the future a study with a large sample and placebo control should be done. The detailed mechanism of CRT effect on constipation in elderly diabetic patients and the effect of individual components of CRT on diabetes-induced colon remodeling should be investigated in detail.
In conclusion, both CRT and Forlax could effectively improve signs and symptoms of constipation in elderly diabetic patients, and CRT is better than Forlax to improve the symptoms and have good follow-up. From the TCM point of view, CRT has efficacy of reinforcing insufficiency, reducing excessiveness, lubricating the bowel, and relieving constipation. From the western medicine point of view, CRT could effectively improve bowel habits and symptoms of constipation in elderly diabetic patients. Furthermore, CRT could partly restore remodeling and inhibit the expressions of AGEs and TGF-β1 and their receptors in the diabetic colon, which may be mechanisms for CRT to better treat constipation in elderly diabetic patients.
Footnotes
Acknowledgments
The study was financially partly supported by Karen Elise Jensen foundation (Project No. 903959) and partly by China-Japan Friendship Hospital (Project No. 2013-MS-35).
Author Disclosure Statement
No competing financial interests exist.