
Abstract
Background:
Acupuncture point (acupoint) injection is a common practice in China. Some trials showed that Chinese herbal extracts and/or conventional medication are injected at the Zusanli (ST36) acupoint for the treatment of diabetic peripheral neuropathy (DPN). The study aimed to assess the effectiveness and safety of acupoint injection for DPN at the ST36 by systematically evaluating the evidence published to date.
Methods:
Six databases were searched for randomized controlled trials (RCTs) of ST36 injection for DPN with primary outcome of pain, global symptom improvement, and quality of life. Methodological quality was assessed by the Cochrane risk of bias (ROB) tool. Data were analyzed using RevMan 5.3.
Results:
Fourteen RCTs involving 1,071 participants with DPN were included. All RCTs were assessed as unclear or high ROB. Few RCTs adequately reported methodology-related items and needling details according to Consolidated Standards of Reporting Trials (CONSORT) and Standards for Reporting Interventions in Controlled Trials of Acupuncture (STRICTA) statement. Medications injected at ST36 included conventional medications (11 RCTs) and Chinese herbal extracts (3 RCTs). The authors of this study did not perform any meta-analysis due to the heterogeneity of medications used for injections. Two individual RCTs favored ST36 injection in relieving pain compared with intramuscular injection of the same medication. For global symptom measured by Toronto clinical scoring system, one RCT showed that ST36 injection of Fufang Danggui was more effective than intramuscular injection of vitamin B12, two RCTs demonstrated that ST36 injection of mecobalamin or Danhong with cointervention was superior, while one RCT showed no significant differences between ST36 injection and intramuscular injection of mecobalamin. For improving nerve conduction velocity (NCV), three of four individual RCTs showed that ST36 injection was better than intramuscular or intravenous injection of the same medication, two RCTs favored ST36 injection with cointervention, and one RCT favored ST36 injection without cointervention. Four RCTs reported monitoring adverse events, all of which showed no significant difference between groups.
Conclusions:
Limited evidence suggests that ST36 injection appears to be safe, and potentially effective in reducing pain score and improving NCV compared with intramuscular injection of the same medication. However, poor methodological and reporting quality reduced confidence in the findings. Rigorously designed and well-reported RCTs evaluating the effectiveness of ST36 injection for DPN are warranted.
Introduction
A
The rigid control of blood glucose can prevent or slow the progression of DPN. 8 Supportive care including podiatric and pain management can improve quality of life and prevent chronic ulceration. 8,9 Some disease-modifying medications including aldose reductase inhibitors, protein kinase C inhibitors, agents acting on the advanced glycation end-product pathway, agents acting on the hexosamine pathway, and reactive oxygen species inhibitors have been considered for the management of DPN. 10
Alpha lipoic acid is an antioxidant that has been shown to improve the symptoms and electroneurographic parameters among subjects with DPN by decreasing lipid peroxidation, reducing oxidative stress, and improving nerve blood flow. 11 And it has been approved for the treatment of DPN in Europe but not in the United States. 11 Pregabalin, duloxetine, and tapentadol have been recommended for the treatment of pain associated with DPN by the U.S. Food and Drug Administration (FDA) and the American Diabetes Association (ADA). 9 However, these therapies were unable to eliminate DPN completely, and there is currently no long-term effective therapy for this condition. 9 –11
In China, Traditional Chinese Medicine (TCM) therapies, including Chinese herbal medicine and acupuncture, 12 –15 have been used in clinical practice for the treatment of DPN. Acupuncture point (acupoint injection) as a combined therapy of Chinese and Western medicine, which is called pharmacoacupuncture in South Korea, has also been used for the treatment of DPN in China. 12,16,17 Acupoint injection involves the injection of medication into certain acupuncture points, also known as acupoints, to treat diseases/conditions through synergetic effects of acupuncture and medication. 16,17
Several systematic reviews have suggested that acupoint injection alone or in combination with acupuncture might be effective for prevention of postoperative ileus, treatment of Bell's palsy, and management of burning mouth syndrome. 18 –20 Recent randomized controlled trials (RCTs) published in China have indicated that acupoint injection with either conventional medication or Chinese herbal extracts could improve motor or sensory nerve conduction velocity (NCV) for patients with DPN. Acupoints selected in these RCTs include Zusanli (ST36), Sanyinjiao (SP6), Quchi (LI11), Yanglingquan (GB34), and Hegu (LI4), among which ST36 is the most commonly used acupoint. 21 –24
Beside the effect of injected medication, acupoint injection involves the effect of acupuncture. According to TCM theory, DPN can be categorized into Bi syndrome (impediment diseases or arthralgia) and Wei syndrome (atrophy-flaccidity diseases) owing to qi and blood deficiency, which results in symptoms such as numbness and pain. 25 Qi translates as “air” and figuratively as “material energy,” “life force,” or “energy flow.” Based on TCM theory, each acupoint has a specific function. ST36 is located below the knee, on the tibialis anterior muscle, along the Stomach meridian. 26 Its function is to fortify the spleen and stomach (promoting gastrointestinal movement), replenish qi and nourish blood, clear and activate meridians and collaterals, and nourish the channels. 26,27
Researchers have shown that ST36 could improve cerebral blood flow, while it decreases sympathetic nerve activity and arterial pressure. 28,29 Acupuncture can significantly reduce blood viscosity and increase blood flow of nerve tissue, which can in turn improve NCV for patients with DPN. 30 In addition, acupoint stimulation may raise levels of plasma morphine, which can relieve pain. 31,32 RCTs evaluating acupoint injection particularly ST36 for DPN have been published in China. However, the evidence has not yet been systematically appraised. The aim of this systematic review was therefore to assess the effectiveness and safety of ST36 injection with conventional medication or Chinese herbal extracts in patients with DPN.
Methods
Search strategy
Six databases were searched from inception until January 2017 with no language restrictions. Two English-language databases were PubMed and the Cochrane Library, and four Chinese-language databases were China National Knowledge Infrastructure (CNKI) database, Chinese Science and Technology Periodical Database (VIP), Wanfang Database, and Sino-Med Database.
The English terms were used individually or combined: “acupoint injection,” “acupuncture point injection,” “hydro-acupuncture,” “pharmacoacupuncture,” “DPN,” “diabetic peripheral neuropathy,” “diabetic neuropathy,” “diabetic polyneuropathy,” and the Chinese searching terms were “xue wei zhu she (acupoint injection),” “shui zhen (acupoint injection),” “shu xue zhu she (acupoint injection),” “tang niao bing zhou wei shen jing bing bian (DPN),” “tangniaobingshenjingbingbian (DPN),” and “tangniaobingxingzhouweishenjingbingbian (DPN).” The search strategies for each database were adjusted according to the characteristics of each individual database, and are listed in Supplementary Data 1 (Supplementary Data are available online at
Inclusion criteria
RCTs on acupoint injection at ST36 were included for treatment of patients with DPN. The authors of this study did not limit the medications injected such as vitamin, conventional medication, Chinese herbal extracts, or combinations of these medications. Control interventions such as no intervention, placebo, or conventional medication (oral or injected at nonacupoint) were accepted. Cointerventions were permitted as long as they were applied in an identical fashion to all treatment groups, and any other TCM therapy such as acupuncture or Chinese herbal medicine was excluded. The primary outcomes were pain measured by a validated instrument such as visual analogue scale (VAS), 33 global symptom improvement measured by Toronto clinical scoring system (TCSS), 34,35 and quality of life measured by the 36-Item Short Form Health Survey (SF-36). Secondary outcomes were NCV, cost-effectiveness, and adverse effects.
Literature screening and study selection
Results from database searches were imported into NoteExpress software, and duplicate citations were removed. Then, two authors (L.Q.W. and Z.C.) independently screened titles and abstracts according to the inclusion criteria described above. Finally, full texts of the remaining citations were independently screened again to identify the trials meeting inclusion criteria by two authors (L.Q.W. and Z.C.), and any disagreement was resolved by discussion with a third author (J.-P.L.).
Data extraction
Two authors (L.Q.W. and Z.C.) independently extracted data using a predesigned form, and any disagreement was resolved by discussion with a third author (J.-P.L.). Data were collected on methodology, participant characteristics, and interventions in all groups, follow-ups, outcomes and adverse effects. The authors of all the included studies were contacted to acquire missing data. The authors of this study assessed missing data and dropouts/attrition for each included study, and discussed and assessed the extent to which the results and conclusions of the review could be altered by the missing data.
Quality assessment
Two authors (L.Q.W. and Z.C.) independently assessed methodological quality using the Cochrane risk of bias (ROB) tool. 36 The following seven items were assessed: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other bias such as baseline comparability.
The ROB in each item was judged as low, unclear, or high. The Consolidated Standards of Reporting Trials (CONSORT) statement 2010 37 was used to assess the reporting quality of the included RCTs. The Standards for Reporting Interventions in Controlled Trials of Acupuncture (STRICTA) checklist 2010 38 was used to assess the completeness and reporting quality of acupoint injection of the included RCTs. Based on characteristic of acupoint injection, the item 2f “Needle retention time” within STRICTA was changed to “Injected medicine and dosage.” No other changes to the STRICTA items were made.
Data analysis
Data not suitable for quantitative synthesis were analyzed descriptively by using RevMan 5.3 software. Mean difference (MD) with 95% confidence intervals (CIs) was used for continuous data, whereas relative risk (RR) with 95% CI was used for binary outcomes.
Results
Description of included studies
Results from the initial database search resulted in 724 citations. After deduplication, 264 were screened according to the inclusion criteria. A total of 71 references passed the screening phase, and full texts were retrieved for further assessment. Of these, a further 57 references were excluded because they did not meet the inclusion criteria. The reasons for exclusion are listed in Figure 1.
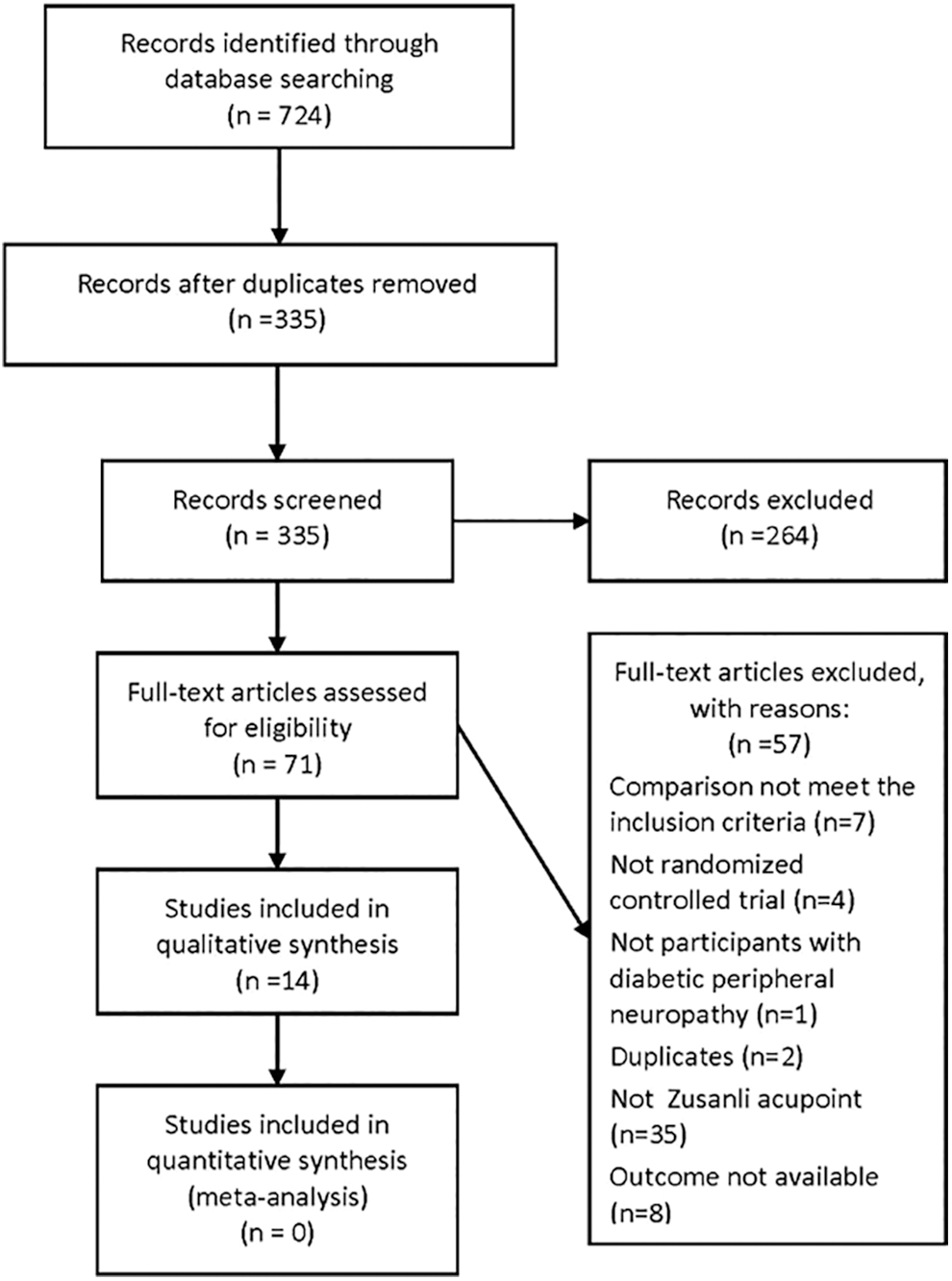
Flow chart of study selection.
Participants
In total, 14 RCTs 39 –52 were included in this review involving 1,071 participants with DPN. The median sample size of the RCTs was 76 ranging from 40 to 140. All RCTs were conducted in China and published in Chinese. Five RCTs 44 –47,51 included inpatients, two RCTs 43,48 included outpatients, and three RCTs 39,40,50 included both outpatients and inpatients. The remaining four RCTs 41,42,49,52 did not specify whether participants were outpatients or inpatients. All of the 14 RCTs reported the diagnostic criteria used, seven 43,45,48 –52 of which used self-defined criteria such as patient with diabetes suffering from pain and numbness of limbs, ankle reflex abnormality, or decreased NCV. Of the 14 RCTs, 12 39 –41,43 –49,51,52 reported the baseline comparability between groups in terms of age, gender, and disease course, while the remaining two RCTs 42,50 did not clarify this (Table 1).
All randomized controlled trials reported incorporating additional treatments for diabetes such as diet control, exercise, oral insulin, or antidiabetic medications for all treatment groups.
C, control; I, intervention; NCV, nerve conduction velocity; NR, not reporting; TCSS, Toronto clinical scoring system.
Interventions
Twelve RCTs 39 –45,47,48,50 –52 included two treatment arms, whereas two RCTs 46,49 included three arms. No placebo-controlled trial was identified. All RCTs reported incorporating additional treatments for diabetes such as diet control, exercise, oral insulin, or antidiabetic medications in all treatment groups. One RCT 41 compared ST36 injection with no intervention, six RCTs 39,40,46,47,49,52 compared ST36 injection with intramuscular or intravenous (IV) injection of same conventional medication, three RCTs 43,45,48 compared ST36 injection with intramuscular injection of different medications, two RCTs 50,51 were ST36 injection of conventional medication with cointervention, and two RCTs 42,44,50,51 were ST36 injection of Chinese herbal extracts with cointervention.
In 11 RCTs, 39 –41,43,45 –47,49 –52 conventional medications including anisodamine (654-2, C17H23NO4), mecobalamin (coenzyme vitamin B12, C63H91CoN13O14P), cobamamide (coenzyme vitamins B12, C72H100CoN18O17P), cyanocobalamin (vitamin B12, C63H88CoN14O14P), or thiamine (vitamin B1) were injected at ST36. In another three RCTs, 42,44,48 Chinese herbal extracts including Fufang Danggui injection (extracts of Radix Angelicae Sinensis, Rhizoma Chuanxiong and Flos Carthami), Danshen injection (extracts of Radix Salviae Miltiorrhizae), and Danhong injection (extracts of Radix Salviae Miltiorrhizae and Flos Carthami) were injected. The median treatment duration was 4 weeks (ranging from 2 to 6 weeks), and post-treatment follow-up was not reported in the included RCTs (Table 1).
Outcome measures
Two RCTs 40,52 reported pain scores using a 4-point scale: 0 means no pain, 1, 2, and 3 represent light, moderate, and severe pain, respectively. 53 Four RCTs 44,48 –50 reported global symptom improvement measured by TCSS (in absolute scores or effectiveness rate defined by reduction of at least three points). For secondary outcomes, seven RCTs 39,41,42,44,46,47,52 reported NCV, including sensory nerve conduction velocity (SNCV) and motor nerve conduction velocity (MNCV). Four RCTs 40,43,45,51 reported monitoring adverse events, while none reported on cost-effectiveness (Table 1).
Methodological quality
Only one 44 of the 14 included RCTs reported the method of random sequence generation, which used a random number table. No trial stated allocation concealment. No placebo trial was identified, and all RCTs incorporated either conventional medication or no intervention as control; therefore, they were assessed as high ROB for blinding of participants and personnel. No trial mentioned blinding of outcome assessors. For incomplete outcome data, only one RCT 39 was assessed as being at low ROB as it reported that all randomized participants completed the study, and two RCTs 43,51 were assessed as being at high ROB since they did not interpret reasons for dropouts and results regarding the impact of missing data. For reporting bias, five RCTs 39,41,44,47,52 reported the outcomes in accordance with what had been described in the Methods section and were considered to be at low ROB. For the “other bias” domain, this was assessed as being at low ROB on account of baseline data comparability in 12 of the 14 RCTs. 39 –41,43 –49,51,52 In summary, the methodological quality of included RCTs was low (Fig. 2).

Risk of bias graph. Color images available online at
The reporting quality assessment of 14 RCTs was conducted based on CONSORT 2010 and STRICTA 2010 statements. According to CONSORT 2010, few RCTs adequately reported the study methodology-related items such as randomization, blinding, and results-related items (Supplementary Table S1). For STRICTA 2010, most of the included RCTs had detailed descriptions on acupuncture rationale and treatment regimen. However, in domains regarding needling details such as other components of treatment, practitioner background, control or comparator interventions, most RCTs did not describe in detail (Supplementary Table S2).
Effects of interventions
The authors of this study did not perform any meta-analysis due to the heterogeneity of medications used for injections. Therefore, the results are presented descriptively in the subsequent sections.
ST36 injection of conventional medication versus no intervention
Nerve conduction velocity
One RCT 41 showed that ST36 injection of anisodamine (654-2) was more effective than no intervention on improvement of NCV at 2 weeks (SNCV in posterior tibial nerve: MD 3.10 m/s, 95% CI 1.86–4.34) (Table 2).
All randomized controlled trials reported incorporating additional treatments for diabetes such as diet control, exercise, oral insulin, or antidiabetic medications for all treatment groups.
CI, confidence intervals; MD, mean difference; MNCV, motor nerve conduction velocity; NCV, nerve conduction velocity; SNCV, sensory nerve conduction velocity; ST36, Zusanli.
ST36 injection versus intramuscular or intravenous injection of same conventional medication
Pain score
Two RCTs 40,52 reported pain score. Both RCTs showed that ST36 injection compared with intramuscular injection was more effective in reducing pain scores at 4 weeks. One RCT 40 compared ST36 injection of mecobalamin with intramuscular injection of mecobalamin (MD −0.31, 95% CI −0.57 to −0.05). Other RCT 52 compared ST36 injection of cobamamide with intramuscular injection of cobamamide (MD −0.36, 95% CI −0.60 to −0.12).
Global symptom improvement measured by TCSS
One RCT 49 showed that there were no significant differences between the ST36 injection of mecobalamin and intramuscular injection of mecobalamin groups in improving effectiveness rate (defined as TCSS scores reduced by three points or more) at 2 weeks (RR 1.92, 95% CI 0.85–4.32).
Nerve conduction velocity
Four RCTs 39,46,47,52 reported NCV. Three 39,47,52 of these four RCTs showed that ST36 injection was more effective than intramuscular or IV injection of same conventional medication on improvement of NCV. Of these three RCTs, one 39 compared ST36 injection of mecobalamin with intramuscular injection of mecobalamin at 2 weeks (SNCV in right superficial peroneal nerve: MD 7.83 m/s, 95% CI 5.02–10.64; MNCV in left tibial nerve: MD 9.40 m/s, 95% CI 6.19–12.61), one 52 compared ST36 injection of cobamamide with intramuscular injection of cobamamide at 4 weeks (MNCV in peroneal nerve: MD 4.01 m/s, 95% CI 1.39–6.63; SNCV in tibial nerve: MD 2.84 m/s, 95% CI 0.46–5.22), the other RCT 47 compared ST36 injection of mecobalamin with IV injection of mecobalamin at 2 weeks (NCV in peroneal nerve: MD 5.23 m/s, 95% CI 3.62–6.84; NCV in tibial nerve: MD 4.97 m/s, 95% CI 2.58–7.36).
The remaining RCT 46 did not show statistically significant improvements in NCV (MNCV in common peroneal nerve: MD 0.67 m/s, 95% CI −2.37 to 3.71; SNCV in common peroneal nerve: MD 1.43 m/s, 95% CI −1.41 to 4.27) when comparing ST36 injection with intramuscular injection of cobamamide at 4 weeks (Table 2).
ST36 injection versus intramuscular injection with different medications
Global symptom improvement measured by TCSS
One RCT 48 showed that ST36 injection of Fufang Danggui was more effective than intramuscular injection of vitamin B12 on improving effectiveness rate (defined as TCSS scores reduced by three points or more) at 6 weeks (RR 3.01, 95% CI 1.83–4.94).
ST36 injection of conventional medication with cointervention
Global symptom improvement measured by TCSS
One RCT 50 reported TCSS scores as an effectiveness rate, defined as TCSS scores reduced by three points or more. In this study, ST36 injection of mecobalamin with cointervention (improving circulation and trophic nerve) compared with cointervention alone showed a statistically significant effect on improving effectiveness rate at 6 weeks (RR 1.13, 95% CI 1.03–1.24).
ST36 injection of Chinese herbal extracts with cointervention
Global symptom improvement measured by TCSS
One RCT 44 reported change in TCSS scores. In this study, ST36 injection of Danhong plus intramuscular injection of mecobalamin compared with intramuscular injection of mecobalamin alone demonstrated a statistically significant reduction in TCSS scores at 4 weeks (MD −3.30, 95% CI −3.98 to −2.62).
Nerve conduction velocity
Two RCTs 42,44 reported NCV, and both showed that ST36 injection of Chinese herbal extracts with cointervention compared with cointervention alone has a statistically significant improvement of NCV.
Of these two RCTs, one RCT 42 compared ST36 injection of Danshen plus IV injection of thioctic acid with IV injection of thioctic acid alone at 4 weeks (NCV in left median nerve: MD 10.44 m/s, 95% CI 4.86–16.02; NCV in right median nerve: MD 11.90 m/s, 95% CI 6.10–17.70; NCV in left common peroneal nerve: MD 6.01 m/s, 95% CI 0.56–11.46; NCV in right common peroneal nerve: MD 5.89 m/s, 95% CI 0.39–11.39), the other RCT 44 compared ST36 injection of Danhong plus intramuscular injection of mecobalamin with intramuscular injection of mecobalamin alone at 4 weeks (MNCV in median nerve: MD 3.63 m/s, 95% CI 1.94–5.32; MNCV in common peroneal nerve: MD 4.68 m/s, 95% CI 2.93–6.43; SNCV in median nerve: MD 3.24 m/s, 95% CI 2.06–4.42; SNCV in common peroneal nerve: MD 4.45 m/s, 95% CI 2.95–5.95) (Table 2).
Safety
Four RCTs 40,43,45,51 reported monitoring adverse events, in which medications injected were mecobalamin, vitamin B1, or vitamin B12. No serious adverse events were reported in any of the four RCTs. There were no significant differences between ST36 injection and control groups in the incidence rate of adverse events (RR 1.86, 95% CI 0.20–17.24, 4 trials, 267 participants). The details of safety and adverse events are listed in Table 3.
CI, confidence intervals; RR, relative risk; ST36, Zusanli.
Additional analysis
Due to insufficient number of trials, a meaningful sensitivity analysis or funnel plot analysis could not be performed.
Discussion
Summary of findings
The effect of healthcare interventions should be evaluated based on rigorously designed trials, since poor quality studies have the potential to overestimate the effect of interventions. 54 –56 This review identified some limited evidence on the effectiveness of ST36 injection of conventional medications or Chinese herbal extracts in patients with DPN. ST36 injection of conventional medications was more effective in improving NCV than no intervention. ST36 injection of conventional medication was more effective in reducing pain score and improving NCV than intramuscular injection with the same medications except one RCT. ST36 injection of conventional medications with cointervention was more effective than cointervention alone in reducing TCSS. ST36 injection of Chinese herbal extracts with cointervention was more effective than cointervention alone in reducing TCSS and improving NCV.
These findings suggest that ST36 injection may have a magnifying effect of the medication administered through acupoint stimulation. Due to the characteristics of acupoint injection, it was supposed that the beneficial effects of the ST36 injection of conventional medication, Chinese herbal extracts, or vitamins result from both medications and stimulation to ST36.
According to TCM theory, the direct stimulation of ST36 replenishes the qi and nourishes blood, clears and activates meridians and collaterals, and nourishes the channels. 26,27 Upon research on experimental animals, it was found that the direct stimulation of ST36 can significantly reduce blood viscosity and increase blood flow of nerve tissue. 28,29 Medications administered in acupoints, through the meridians, are thought to play a synergistic effect with acupoint stimulation, and are thought to have a more sustained effect than traditional acupuncture needling or simple intramuscular injection. 57 It might be one of the underlying mechanisms of ST36 injection for the improvements observed in pain scores, TCSS, and NCV.
Four of 14 trials reported monitoring adverse events, and found no significant differences in incidence rates between acupoint injection and intramuscular or IV injection groups. Although it suggests that ST36 injection is likely to be safe for treatment of DPN, it is important to remember that the majority of these 14 RCTs did not report monitoring adverse events, and the possibility of reporting bias for this reason cannot be excluded. Furthermore, based on the ROB tool and the CONSORT 2010 37 and STRICTA 2010, 38 the study assessments indicated that the methodological and reporting quality of the included RCTs was low. It is therefore impossible to make firm conclusions about ST36 injection for the treatment of DPN with the current evidence to date.
Comparison of the previous studies
There are three relevant systematic reviews published previously in English. The first review 58 included 13 RCTs evaluating acupuncture for peripheral neuropathy, 4 of which involved patients with peripheral neuropathy caused by diabetes. This review found that acupuncture was superior to conventional therapies such as oral thiamine plus intramuscular injection of vitamin B12, IV injection of vitamin B12, oral mecobalamin, and oral inositol on improving sensory and motor nerve for DPN.
The second review 14 involving 25 RCTs with 1,649 participants compared manual acupuncture with mecobalamin, vitamin B1, B12, and no intervention for DPN, and showed that manual acupuncture was superior in improving global symptom and NCV. Similarly, this review also found that ST36 injection may have an additional effect in improving NCV compared with no intervention or conventional therapies such as intramuscular or IV injection of mecobalamin, vitamin B1, or vitamin B12. Moreover, this review found that ST36 injection of conventional medication was more effective in reducing pain scores compared with intramuscular injection of same medications, and ST36 injection of Chinese herbal extracts with cointervention was superior in reducing TCSS. These findings indicated that acupoint stimulation appears to be effective for the treatment of DPN.
However, the above two reviews also identified multiple methodological problems and failed to make conclusive conclusions. In addition, one study 15 published in 2012 evaluated reporting quality of 75 RCTs on acupuncture for DPN according to CONSORT 2010 and STRICTA 2010 statements, and found that the included studies had low-to-moderate reporting quality. Similarly, the included RCTs in this review were assessed as having low reporting quality based on the CONSORT 2010 37 and STRICTA 2010. 38 Hence, more attention should be paid to improving the methodological and reporting quality of clinical trials on acupoint injection by future researchers.
The third review 18 involving 30 RCTs with 2,967 participants compared the ST36 acupoint injection of conventional medication with no intervention, usual care, or intramuscular injection for prevention of postoperative ileus. It showed that ST36 acupoint injection was more effective than intramuscular injection of same vitamin in reducing time to first flatus, time to bowel sounds recovery and first defecation. However, the safety of ST36 injection remained unclear as few of included trials reported adverse events information in this review.
Similarly, this review also found that ST36 injection was more effective than intramuscular injection of same conventional medications in reducing pain scores and improving NCV. These findings indicated that ST36 injection may magnify the effect of acupoint stimulation on ST36 and the medication injected. Meanwhile, this review also found that ST36 injection of conventional medications or vitamins was safe and may lead to a little local pain, but there is limited evidence.
Limitations
This review has several limitations. First, there were many different medications injected in the included trials, with a limited number of trials testing the same medication. Second, the heterogeneity of NCVs on points for measurement makes it impossible to synthesize the data into meta-analyses. Third, included trials did not provide data on the effect of ST36 injection on the quality of life or long-term effectiveness of DPN patients. Furthermore, this review only considered ST36 injection and excluded RCTs that applied acupoint injection at other acupoints, and did not compare the effects of using the same interventions acupoint injection at different other acupoints. Finally, the limited number of included trials with small sample size and poor methodological quality reduced confidence in the findings.
Implications for clinicians
In this systematic review, it was found that the conventional medications, especially mecobalamin, were most commonly used among the trials on ST36 injection for DPN, and were effective in improving pain and NCV. Dosages of these medications used in ST36 injection are basically the same as intramuscular injection at a standard dose. Hence, this review suggests that the benefits of administering mecobalamin in improving pain and NCV for DPN may be further improved by injecting the standard dose of 0.5 mg at ST36, once daily for 4 weeks. However, due to lack of strong evidence, the implications for clinical use are very limited. Meanwhile, ST36 injection of Chinese herbal extracts (Fufang Danggui, Danshen, or Danhong injection) with cointervention used among the trials for DPN was superior in reducing TCSS and NCV; however, safety was unclear. Hence, the safety of Chinese herbal extracts used among ST36 injection needs further understanding.
Implications for further research
It was suggested that future trials consider exploring the relationship between the severity of DPN and the response to ST36 injection in treating DPN-related symptoms. It is also important to note that further rigorous RCTs are conducted to provide stronger evidence regarding the effects of ST36 injection of mecobalamin for DPN. Future RCTs evaluating ST36 injection for DPN are recommended to include relevant outcomes such as global symptom improvement measured by a validated instrument, pain measured by VAS, quality of life, and safety. A follow-up period of 6 months is necessary to evaluate the long-term effect of ST36 injection for DPN. 5
Multicenter, large sample, placebo-controlled randomized trials with rigorous methodological quality are required to define the extent of benefit from ST36 injection before this treatment can be recommended for clinical use. The reporting of RCTs using ST36 injection should be in accordance with the standards of CONSORT 2010 and STRICTA 2010. 37,38 When assessing the reporting quality of acupoint injection using STRICTA 2010, it was suggested that “Needle retention time” is changed to “Injected medicine and dosage” based on characteristic of acupoint injection.
Conclusion
Limited evidence suggests that ST36 injection appears to be safe, and ST36 injection of conventional medications is potentially more effective than intramuscular injection with same medications in reducing pain score and improving NCV in patients with DPN. Meanwhile, ST36 injection of conventional medication or Chinese herbal extracts with or without cointervention is superior in reducing TCSS and improving NCV. However, included RCTs in this review had small sample sizes, with poor methodological and reporting quality, which reduced confidence in the findings. The authors of this study recommend further rigorously designed, large-scale RCTs to test the effect of pain and quality of life and monitor adverse events. The CONSORT and STRICTA statements should be utilized to improve the methodological and reporting quality of trials.
Footnotes
Acknowledgments
The authors thank George Lewith from the Centre for Complementary Medicine Research, University of Southampton, and Huijuan Cao, and Wei Chen from the Center for Evidence-Based Chinese Medicine, Beijing University of Chinese Medicine for their professional advice. This work was partly supported by the project for capacity building in evidence-based Chinese medicine and internationalization (1000061020008). L.Q.W. was supported by the Independent Research Project from Beijing University of Chinese Medicine (2017-JYB-XS-022). J.-P.L. was partially funded by Grant No. R24 AT001293 from the National Center for Complementary and Alternative Medicine (NCCAM) of the U.S. National Institutes of Health.
Disclaimer
The contents of this article are solely the responsibility of the authors and do not necessarily represent the official views of the NCCAM or the National Institutes of Health.
Authors' Contributions
L.Q.W. conceived and designed the review. Z.C. and L.Q.W. were responsible for the searching, screening, and selecting studies. L.Q.W. and Z.C. undertook data extraction and assessment of the methodological quality. L.Q.W. and K.Z. contributed to performing data analysis and drafting the manuscript. J.-P.L., L.L., L.Q.W., G.Y.Y., K.Z., and N.L. were involved in critically revising the manuscript. All authors read and approved the final article.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.