
Abstract
Background:
This study was conducted to test the hypothesis that prenatal yogic exercises are effective in alleviating labor pain and improving birth outcomes, by comparing pregnant women undertaking yoga with a control group.
Trial design:
Single blinded, parallel randomized control trial.
Methods:
Two hundred primigravid women of 30 weeks of gestation onward who met the inclusion criteria (primigravida, 20–35 years of age, gestational age of 30 weeks, no prior experience of yoga) were randomly assigned to study (n = 100) and control groups (n = 100) by using the minimized randomization program version 2.01. The study group received the intervention in the form of integrated yoga consisting of a series of 30-min practice sessions at the 30th, 32nd, 34th, 36th, 37th, 38th, and 39th weeks of gestational age. The matched control group did not perform yoga. The patients were followed till delivery for maternal comfort, alleviation of labor pain, and birth outcome. Alleviation of labor pain was assessed by using numerical pain intensity scale (NPIS), pain behavioral observational scale (PBOS), and maternal delivery comfort questionnaire. Only the assessors were blinded.
Results:
Two hundred patients were randomized into 100 each in case and control groups. Final analysis was done on 75 patients in each group after exclusion due to development of complications, loss to follow-up. The requirement of induction of labor and analgesics was significantly less in the study group (p < 0.044, p < 0.045). There was significantly more number of normal vaginal deliveries (p < 0.037) and less caesarean sections (p < 0.048), shorter first stage of labor (p < 0.0003) in the study group practicing yoga. The tolerance of pain was better in the study group as shown by NPIS (p < 0.001) and PBOS scores (p < 0.0001). Postpartum, the maternal comfort questionnaire score showed higher comfort in the study group (p < 0.032). The number of low birth weight babies was also significantly less in the study group (p < 0.042). There were no adverse effects attributed to yoga.
Conclusion:
The study has highlighted that yoga is a noninvasive, easy to learn mind-body medicine and complementary health practice, effective in alleviation of labor pain and possibly improving birth outcome.
Introduction
P
It is suggested to use a multidisciplinary approach to pain management in labor and incorporate both pharmacological and nonpharmacological approaches that can be tailored to individual preferences. 3
Yoga is an ancient system of mind-body practice that originated in India and is becoming increasingly recognized as a health practice for a variety of immunological, neuromuscular, psychological, and pain conditions. 4 The word yoga comes from a Sanskrit root yuj that means to yoke, to join, and to direct and concentrate one's attention. The practice and philosophy was first described by Patanjali in the classic text Yoga Sutras. 1 It is thought to alter nervous system regulation and physiological system functioning (e.g., immune, endocrine, neurotransmitter, and cardiovascular) and improve psychological wellbeing (e.g., frequency of positive mood states and optimism) and physical fitness (e.g., strength, flexibility, and endurance). 5
Improvement of comfort during labor pain through the integrated approach of yoga is achieved by the practice of deep relaxation at the somatic level in different postures (asanas), slow controlled breathing to decrease the respiratory rate (pranayama), and mind calming techniques such as meditation and chanting. It has been speculated that yoga can produce physiological changes that alter the pain experience by decreasing sympathetic nervous system activity (e.g., decreases in heart rate); reducing inflammatory markers (e.g., tumor necrosis factor, interleukin-II, CRP) and stress markers (e.g., cortisol); and increasing flexibility, strength, circulation, and cardiorespiratory capacity. 6,7 It indirectly acts on the HPA axis thereby improving birth weight, decreasing preterm labor and intrauterine growth restriction (IUGR). 1
Sun et al. in 2010 did a nonrandomized controlled experiment in Taiwan to evaluate a yoga programme provided to primigravidas in the third trimester of pregnancy with the aim of decreasing the discomforts associated with pregnancy and increasing childbirth self-efficacy. The target population was primigravidas at 26–28 weeks of gestation with no high-risk, who had not engaged in regular exercise or yoga for at least 1 year. Women who took part in the prenatal yoga programme reported significantly fewer pregnancy discomforts than the control group (38.28 vs. 43.26, z = −2.58, p = 0.01) at 38–40 weeks of gestation and exhibited higher outcome and self-efficacy expectancies during the active stage of labor (104.13 vs. 83.53, t = 3.24, p = 0.002; 99.26 vs. 77.70, t = 3.99, p ≤ 0.001) and the second stage of labor (113.33 vs. 88.42, t = 3.33, p = 0.002; 102.19 vs. 79.40, t = 3.71, p ≤ 0.001) compared with the control group. 8
Narendran et al. studied the efficacy of yoga on pregnancy outcomes in 2005. Three hundred thirty-five were enrolled between 18 and 20 weeks of pregnancy in a prospective, matched, observational study; 169 women in the yoga group and 166 women in the control group. Yoga practices, including physical postures, breathing, and meditation were practiced by the yoga group 1 h daily, from the date of entry into the study until delivery. The control group walked 30 min twice a day during the study period. The number of babies with birth weight > or = 2500 g was significantly higher (p < 0.01) in the yoga group. Preterm labor was significantly lower (p < 0.0006) in the yoga group. Complications such as isolated IUGR (p < 0.003) and pregnancy-induced hypertension (PIH) with associated IUGR (p < 0.025) were also significantly lower in the yoga group. There were no significant adverse effects noted in the yoga group. 1
In another review Curtis et al. evaluated the existing literature on yoga for pregnancy. Yoga is used for a variety of immunological, neuromuscular, psychological, and pain conditions. Recent studies indicate that it may be effective in improving pregnancy, labor, and birth outcomes. They searched six databases using the terms “yoga AND pregnancy” and “yoga AND [post-natal OR post-partum].” Trials were considered if they were controlled and evaluated a yoga intervention. All studies were evaluated for methodological quality according to the Jadad scale and the Delphi List. Six trials were identified: three were randomized controlled trials (RCTs) and three were controlled trials (CTs). The methodological quality and reporting ranged from 0 to 5 on the Jadad scale and from 3 to 6 on the Delphi List. Findings from the RCT studies indicate that yoga may produce improvements in stress levels, quality of life, aspects of interpersonal relating, autonomic nervous system functioning, and labor parameters such as comfort, pain, and duration. They concluded that the findings suggest that yoga is well indicated for pregnant women and leads to improvements on a variety of pregnancy, labor, and birth outcomes. However, RCTs are needed to provide more information regarding the utility of yoga interventions for pregnancy. 4
A small RCT in 2008 in Thailand by Chuntharapat et al. examined the effects of a yoga programme in 74 healthy primigravidas during pregnancy with outcomes being assessed on 66 women, on aspects of the women's experiences related to comfort, labor pain, and birth outcomes. The women in the yoga group were invited to undertake six, 1-h sessions of yoga and were encouraged to practice at home too, during weeks 26th–28th to 37th–38th of gestation. Women in the control group had routine care at hospital visits lasting about 20–30 min. Labor variables such as maternal comfort, self-reported and experimenter-observed pain, length of labor, augmentation, use of medication, and birth outcomes, such as Apgar scores, were assessed in an RCT comparing an integrated yoga program to routine nursing care. The women doing yoga were found to have higher levels of comfort during labor and at 2 h after labor, and reported less labor pain than the women in the control group. The women doing yoga were also reported to have shorter labors (p < 0.05). 7
Yoga has been extensively evaluated but lacks a comprehensive systematic review. At present, there are no randomized trials or recommendations from professional organizations regarding the role of yoga during pregnancy.
Materials and Methods
The study was conducted in the antenatal outpatient department, labor room of department of Obstetrics and Gynaecology in Lady Hardinge Medical College and Associated hospitals, New Delhi. Ethical clearance was given by the ethical board of the medical college hospital and the university. It was an parallel, single blinded RCT, conducted from November 2012 to March 2014 that enrolled pregnant women of 30 weeks gestation and above after taking informed consent. After ethical approval, they were randomized by using the minimized randomization program version 2.01
9
into Study group: undertaking prenatal yoga Control group: who do not undertake yoga
The inclusion criteria: primigravida, 20–35 years, gestational age of 30 weeks, no prior experience of yoga. The exclusion criteria: maternal skeletal abnormalities/physical disabilities; medical complications: diabetes, hypertension, asthma, and heart disease; obstetric complications: multiple pregnancy, PIH, antepartum hemorrhage (APH), IUGR, premature rupture of membranes (PROM), oligohydramnios, polyhydramnios, and major fetal congenital malformations.
In the control group, 25 women were excluded along the course of the study as 5 developed PIH, 2-GDM, 4-IUGR, 3-PROM,1-severe anemia, 4-Oligohydramnios, 2-APH, and four patients were lost to follow-up. In the study group also, 25 women were excluded (2 developed PIH, 1-GDM, 2-IUGR, 3-PROM, 1-severe anemia, 2-oligohydramnios, and 2-APH; 7 patients discontinued doing yoga and 5 were lost to follow-up). Final analysis was done on 75 patients of study and 75 of control group (Fig. 1).
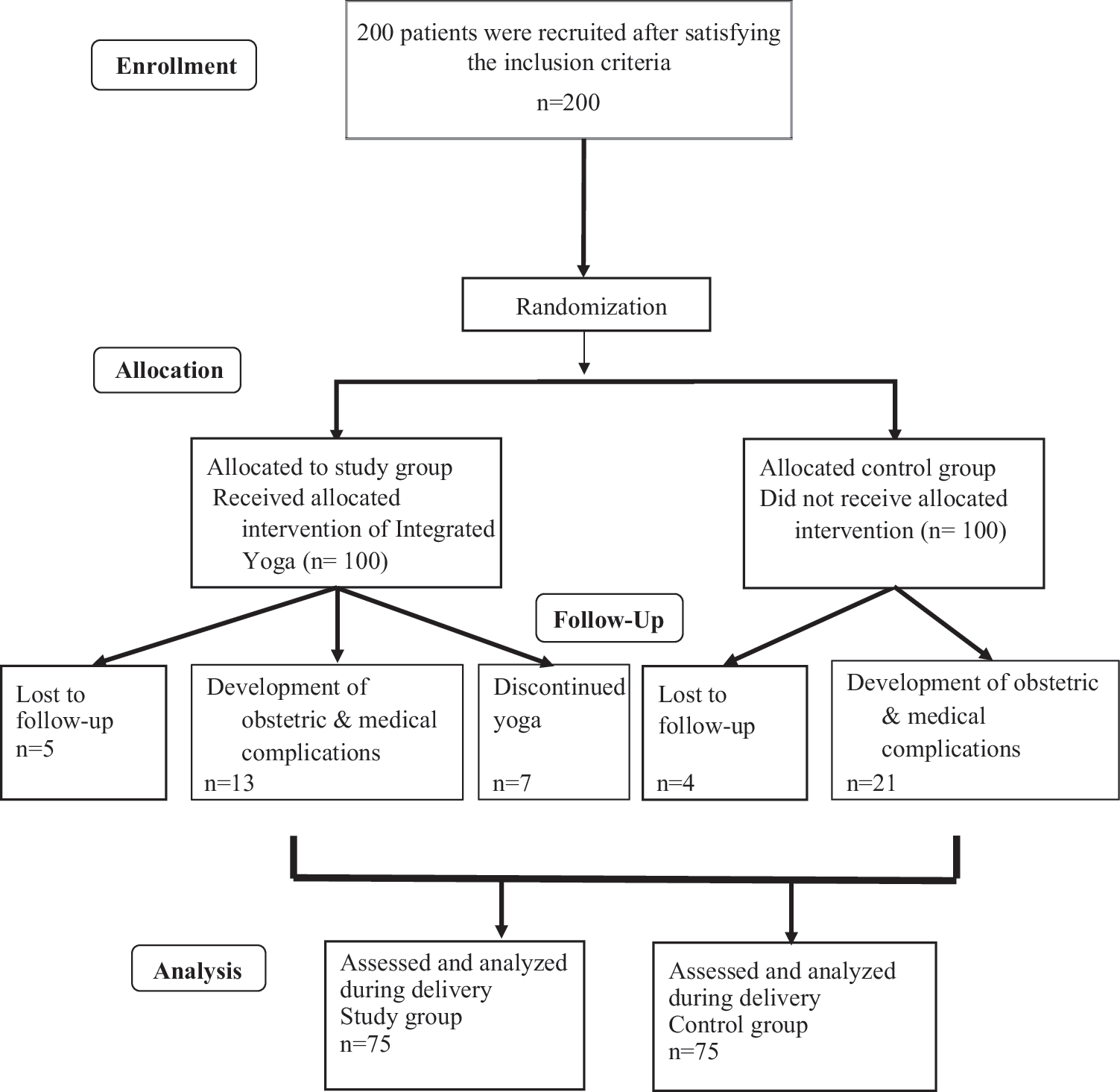
Participant flow diagram.
Both the groups received standard antenatal care. Integrated approach of yoga therapy was taught by a well-trained yoga therapist in groups of 10 pregnant women. They received a series of 30 min practice sessions at the 30th, 32nd, 34th, 36th, 37th, 38th, and 39th week of gestational age. Subsequently, they were asked to practice at home at least thrice a week. A booklet for self-study use, which explained the principles and benefits of yoga was provided. Compliance in both groups was ensured by making frequent telephone calls and ensuring maintenance of a strict record in a diary.
The Yoga Program had a combination of educational activities giving a brief description of basic anatomical structures related to pregnancy, labor, and concepts of yoga. Intention to treat approach was used when any of the participants developed any of the medical or obstetric complications during the course of the study. The yoga practices included Nadisudhan Pranayam (Anulom-Vilom), and Bramhari, Asanas to strengthen the pelvic muscles: Gentle butterfly-Baddha Konasana, Chakki chalanasana; Asanas to strengthen the back and leg muscles, spine twisting exercises, Vakrasana/Ardha matsyendrasana (modified), Marjari asana, Konasana, and Pavanamuktasana, Others—loosening of wrist and fingers, shoulder rotation, hands stretch breathing, neck loosening exercises, Dhyana—meditation and Yoga nidhra. Care was taken to avoid practices that were contraindicated. 10
Patients were meticulously monitored. All the assessment and recording of outcomes and results were done by a blinded assessor in a separate file, while the provider of care was a different person. The duration of each stage of labor was assessed. Intensity of pain was assessed using numerical pain intensity scale (NPIS) at 3–4 and 8–10 cm cervical dilatation. The responses were recorded using a 11-point scale (0 is no pain and 10 is the worst pain imaginable).
Pain behavioral observation scale—consists of five aspects in the observation of vocalization expressed, body movement, breathing control, facial expression, and communication. Each part uses a three-point Likert scale. Low scores indicate severe pain. It was measured from the beginning of uterine contraction until relaxation. This scale was administered at the end of first stage when pain was maximum.
Three different scales were combined to assess comfort and pain during labor so that a comprehensive assessment of pain could be done including intensity, sensory and affective dimensions.
Injection tramadol was given for analgesia on request. The number of injections given was noted. Delivery was conducted meticulously. Instrumental delivery, caesarean section was performed when the need arose.
Two hours postpartum, the maternal delivery comfort questionnaire, a modification from The General Comfort Questionnaire was administered. The items were presented with a Likert-type format, ranging from “strongly agree” (5) to “strongly disagree” (1), the higher scores indicating higher comfort.
The comfort of the mother in breast feeding was noted and compared. The neonates' birth weight, APGAR score at 1, 5, and 10 min, respiratory distress, admission to NICU, and duration of admission was noted.
Results of study were tabulated and analyzed using standard statistical methods such as SPSS software, version 20. Gaussian distribution of data was tested using Kolmogorov–Smirnov test. Nonparametric data were analyzed using Chi-square test and parametric data using mean, standard deviation, and Student's t test. Adjusted odds ratio (AOR) was calculated using multinominal logistic regression (mode of delivery, analgesics) and ordinal regression (NPIS and pain behavioral observational scale [PBOS]). p < 0.05 was taken as significant.
Results
The demographic and clinical parameters of both the groups were comparable (Table 1). The requirement for induction of labor was less in the study group practicing yoga compared with control group (p < 0.044). Though the requirement of oxytocin augmentation in the study group was less, it was not statistically significant (p < 0.070). Significant reduction in requirement of intravenous analgesic was noted in the study group (p < 0.045). The requirement of multiple doses of analgesic did not differ in patients' whose labor was induced (AOR = 1.198, 95% confidence interval [CI]: 0.451–3.18, p = 0.717). There was significantly more number of normal vaginal deliveries (p < 0.037) and less requirement of caesarean sections (p < 0.048) in the study group practicing yoga. Induction of labor did not influence the mode of delivery significantly (AOR = 1.147, 95% CI: 0.433–3.036, p = 0.783). The operative vaginal delivery rate showed no difference (p < 0.547). The duration of first stage of labor and the total duration of labor showed significant shortening in the study group when compared with the control group (p < 0.001) (Table 2).
BMI, body mass index.
Bold indicates significance at p < 0.05.
AOR = 1.198, 95% CI: 0.451–3.18, p = 0.717.
AOR = 1.147, 95% CI: 0.433–3.036, p = 0.783.
AOR, adjusted odds ratio; CI, confidence interval; LSCS, lower segment cesarean section.
The mean NPIS score at the onset of second stage of labor was significantly less in the study group when compared with the control group (p < 0.001). There was no significant difference noted between patients who had spontaneous or induced labor, with respect to the NPIS score at onset of active stage (AOR = 1.54, 95% CI: −0.322 to 1.192, p = 0.26). At the end of second stage of labor, it was less in the study group, but did not reach statistical significance (p < 0.089). There was statistically significant difference in the Pain Behavioral Observation scores between the two groups (p < 0.001). PBOS scores were not affected by induction of labor (AOR = 4.39, 95% CI: −0.881 to 0.585, p = 0.692). Hence, the tolerance of pain was better in the study group who practiced yoga (Table 3).
Bold indicates significance at p < 0.05.
AOR = 1.54, 95% CI: −0.322 to 1.192, p = 0.26.
AOR = 4.39, 95% CI: −0.881 to 0.585, p = 0.692.
AOR, adjusted odds ratio; CI, confidence interval.
Regarding the maternal comfort questionnaire score, there were fewer patients in the study group in the lower comfort score range (bottom 25% of the score range). Higher number of patients in the study group had scores within the top 25% of the range (32–34), which indicates better comfort (p < 0.032). Thus, the study group practicing yoga had a better comfort level when compared with control group (Table 4).
Bold indicates significance at p < 0.05.
The number of preterm deliveries did show a fall in study group, although statistical significance was not found (p < 0.785). There was no statistical significance observed with respect to comfort in initiation of lactation and neonatal morbidity. The number of low birth weight babies was also significantly less in the study group (p < 0.042) (Table 5).
Bold indicates significance at p < 0.05.
Discussion
Childbirth can be a stressful experience in which self-efficacy plays an important role in the ability to cope. Thus, yoga can help to strengthen themselves to bear the pain, transform stress, and anxiety to energy. 8 Therefore, the purpose of this study was to investigate the effects of using a yoga program during pregnancy on enhancing maternal comfort and reducing pain during labor, and improving birth outcomes.
Demographic and clinical parameters
In this study, all patients were between 20 and 35 years, which was comparable to studies by Narendran et al. 1 and Chuntharapat et al. 7 Only primigravid women were included in this study, which was not a criterion in the other studies.
We enrolled patients at 30 weeks of gestation, a similar finding in study by Chuntharapat et al. 7 But Beddoe et al. 11 and Narendran et al. 1 recruited patients in the second trimester. The gestational age criterion was selected because women are usually well established in their prenatal care by the third trimester, adequate time would be available for practicing and performing yoga for further 10–12 weeks. First-time pregnant women in the first two trimesters were not included to avoid the anxiety associated with pregnancy loss in early gestation.
Intervention
A similar regimen was followed by Chuntharapat et al. in their study but the session lasted longer (1 h). 7 In a study in Bengaluru, yoga was practiced for 1 h daily from the date of entry into the study till delivery. Sun et al. had three sessions per week. 8
Progress of labor
The requirement of labor induction was significantly less in the study group in our study. In contrast Kim et al. did not report any difference. 12
Though the requirement of augmentation in the study group was less, it was not statistically significant (p < 0.070). Similar findings were noted by Kim et al. 12 and Chuntharapat et al. 7
A significant reduction in the duration of first stage of labor was estimated in the study group (p < 0.0003). Second stage was comparable. There was significant reduction in the total duration of labor as the first stage formed the major part of total duration of labor.
Comparable findings were estimated in a similar study by Chuntharapat et al., 519.88 ± 185.68 min in the study group and 659.79 ± 272.79 in the control group (p < 0.05). 7 Kim et al. did not report any significant decrease. 12
Shortening of duration of labor was also observed in the study by Hawrelak et al. 13
Pain during labor
The mechanism that has been most frequently used to explain massage therapy effects on pain syndromes, the Gate theory, might also pertain to yoga inasmuch as yoga is a form of self-massage, as in limbs rubbing against limbs and against the floor and stimulating pressure receptors. According to the gate theory, pain stimulates shorter and less myelinated (or less insulated) nerve fibers so that the pain signal takes longer to reach the brain than the pressure signal, which is carried by nerve fibers that are more insulated and longer and therefore able to transmit the stimulus faster. The message from the pressure stimulation reaches the brain prior to the pain message and “closes the gate” to the pain stimulus.
Another theory that is commonly referenced is the deep sleep theory. In deep sleep, less substance P is emitted and therefore less pain occurs because substance P causes pain.
Still another theory is that less pain results from increased serotonin levels, serotonin being the body's natural antipain chemical. Serotonin also decreases cortisol and depression, which are also important effects of massage therapy. And, serotonin is also noted to decrease substance P and other pain-causing chemicals, highlighting the complex interaction between massage therapy's effects on biochemistry. Future yoga studies might use multiple physiological and biochemical measures to enhance our understanding of the mechanisms underlying the pain reduction effects of yoga. 3
Refer Figure 2 for an illustration showing potential underlying mechanisms for yoga reducing pain.
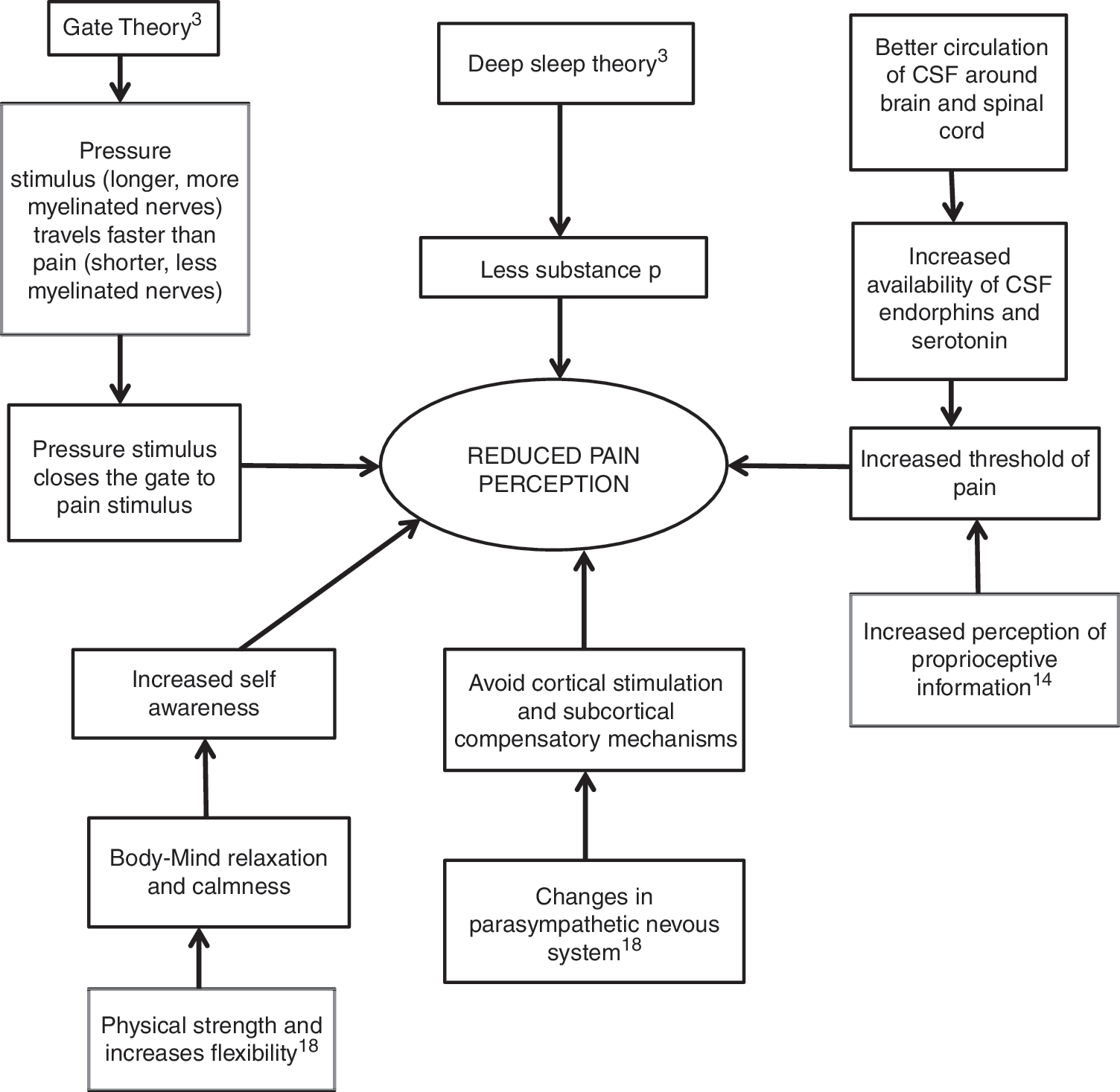
Illustration showing potential underlying mechanisms for yoga reducing pain.
Using the NPIS, the perception of pain was significantly less in the study (p < 0.001) at the onset of active stage but comparable at the end of active stage (p < 0.089).
Chuntharapat et al. 7 used VASPS (visual analogue sensation of pain scale), a scale similar to NPIS. This scale was administered at 3–4 cm cervical dilatation and at the end of 2 h, twice in the active stage. The mean scores were significant at time 1, 2 and 3 (p < 0.05). 7 Thus, both the studies showed that patients practicing yoga perceived less pain during active stage of labor.
Pain behavioral observation scale was administered at the end of first stage when pain was maximum and a statistically significant difference was found (p < 0.0001).
The PBOS was applied at time 1, 2, and 3 similar to VASPS in a study by Chuntharapat et al., which were statistically significant (p < 0.05). 7
Hence, significantly better tolerance of labor pain in the study group involved in regular yogic exercises was inferred by both the studies.
In a review involving six trials by Curtis et al., it was found that yoga had a definitive role in decreasing adverse maternal and fetal response to pain. 4
Mode of delivery
The rate of normal vaginal deliveries in this study was 82.66% in the study group when compared to 68% in the control group (p < 0.037). Hence patients practicing yoga had significantly more vaginal deliveries and less lower segment cesarean section.
But a study by Narendran et al. did not find any statistical significance (p < 0.08) in the mode of delivery. 1
Bastani et al. in their study reported significant reduction in caesarean section and instrumental extraction in the study group due to 7-week applied relaxation training in anxious Iranian women. 14
Maternal comfort questionnaire score
A higher comfort level was observed in the study group practicing yoga when compared with control group (p < 0.032).
Chuntharapat et al. used a similar maternal comfort questionnaire (consisting of 35 questions) 2 h postdelivery. The mean scores were 155.70 ± 13.43 in the study group and 150.36 ± 11.70 in the control group. The mean difference was 6.34 (t = 0.045, p < 0.05). 7
The study group of Sun et al. in Taiwan exhibited higher comfort during active stage of labor (p < 0.001). 8
All three studies estimated higher comfort in the yoga group during delivery.
Fetal outcome
The number of preterm deliveries in both the groups were comparable (p < 0.691). Barakat et al. in their study evaluating possible cause-effect relationship between regular exercise and gestational age at delivery, did not find any difference in preterm birth rates. 15
But significant reduction in preterm births in the yoga group was found in a study by Narendran et al. 1 A similar result was seen by Rakhshani et al. 5 (p < 0.04). In a study on women with preterm labor by Chuang et al. in Taiwan, relaxation training program was found effective in significantly prolonging pregnancy in the study group when compared with the control group (p < 0.048). 16 Juhl et al. 17 also showed that physical exercise reduced the risk of preterm birth in 40% of the women.
Thus, healthy gravidae with singleton gestation can safely engage in moderate, supervised exercise programs without the risk of preterm births.
In the present study, the number of low birth weight babies was less in study group with statistical significance (p < 0.042). Two other studies by Narendran et al. 1 and Bastani et al. 14 also showed yoga to be effective in reducing the birth of low birth weight babies.
Low APGAR score at 5 min in the control and study groups did not show any statistical significance (p < 0.988) in our study. This is comparable to the findings of Kim et al. 12 and Chuntharapat et al. 7 However, Rakhshani et al. 5 showed significant differences between the number of babies with low APGAR scores at 1 min and 5 min in the study and control group (p < 0.01 and 0.04, respectively). 5
Limitations
This study excluded high risk pregnancies. It could raise a question that whether the results of this study would apply to the general population.
A demographic limitation was that most of the women were at grade 12 or lower of education. Additional variables such as socioeconomic status, motivation, and lifestyle to determine the effect of environmental factors have not been used here.
Frequency of home practice of yoga was based on subjective self-reports from each participants.
Further studies are necessary to replicate the beneficial findings of this yoga program in larger populations and to better elucidate physiological mechanisms underlying pain relief during labor and delivery.
Recommendations for future studies
The results can be used to power a larger cohort follow-up study, which may not only confirm these results but also allow meaningful statistical analysis.
A study that starts the yoga interventions much earlier in the first trimester or before conception could shed some light on the role of yoga in placentation and oxidative stress.
Further research is required to explore benefits of yoga in diverse groups of pregnant women including those with high risk pregnancies.
Conclusion
Prenatal yoga program results in benefits during pregnancy and throughout labor. It is well suited to pregnancy without any adverse effects when practiced under training and supervision.
The study has highlighted that yoga is a noninvasive, easy to learn mind-body medicine and complementary health practice, effective in alleviation of labor pain and possibly improving birth outcome.
There was considerable reduction in pain perception, better tolerance and behavior during the severe pain of active stage of labor. It also facilitated shortening of labor, improvement of comfort, allowed spontaneous normal vaginal deliveries, fewer caesarean sections, and low birth weight babies. Thus, yoga could give mothers the opportunity to enjoy pregnancy and childbirth to the fullest. These results, however, need to be verified on a larger pregnant women population by randomized control trials.
Footnotes
Acknowledgments
The first author acknowledges all the co-authors for their valuable support and inputs during the study. The trial was not registered in the national clinical trial register as it was done as a part of dissertation for obtaining postgraduation degree.
Author Disclosure Statement
No competing financial interests exist.