
Abstract
Objectives:
Blood stasis is an important pathophysiologic concept in Traditional East Asian Medicine. It has been considered to be a pathogenic factor in chronic and incurable conditions such as pain, infertility, cancer, coronary heart disease, and others. The aim of this study was to investigate the effects of pain reduction by blood stasis treatment for blood stasis syndromes with traumatic injury.
Methods:
A single-center prospective pretest–post-test pilot study included 73 patients with a trauma that occurred within the past 2 weeks who were admitted into Jaseng Hospital of Korean Medicine from August 2015 through December 2015. Of the 50 patients analyzed in this study, 42 were women (mean age, 33.52). Triple Energizer-reinforcing Saam acupuncture set, herbal medicine (Dangkwisoo-san), and wet cupping on tender point, which are Korean medical therapies generally executed to treat post-traumatic pain, were performed. The patients had to receive at least six sessions of treatment during the 2 weeks, with subsequent treatment being performed within 3 ± 1 days after the previous treatment. Numeric rating scale (NRS) score and general pain severity indicator was measured as a primary outcome measure. The blood stasis questionnaire, oximetry, and patient's satisfaction were also measured.
Results:
The mean size of subcutaneous bleeding (width and length) and NRS score as a general pain indicator significantly decreased over the visits (all p < 0.01, visit 1 vs. visit 6). Among the blood stasis symptoms in the questionnaire, 11 blood stasis indicators significantly decreased (all p < 0.05). The patients showed significant improvement in the minimum and maximum value of peripheral perfusion index after the treatment (p = 0.011 and p = 0.15, respectively).
Conclusions:
This study reveals that blood stasis treatment may help improve the pain of patients with traumatic injury by enhancing the peripheral blood flow. The significant results observed in this study support some evidence of the theories of diagnosing blood stasis pattern and treatments of that pattern in Korean Medicine.
Introduction
Conventionally, the Traditional Chinese medical concept of blood stasis (also known as Oketsu in Japan and Xueyu Zheng in China) refers to stagnant blood in the body that does not flow through blood vessels or body fluid that has deviated from its original position. 1 –4 In Korean Medicine, blood stasis is considered a factor that induces diseases by obstructing the blood flow in the meridian system. 5,6 According to the report released by the Korea Center for Disease Control and Prevention, 7 of the top 10 causes of death in 2013 were chronic diseases. The cost to treat patients of chronic diseases, 38 trillion won ($32.06 billion), accounted for nearly 80% of the entire medical bills in 2013. 7 Chronic and intractable diseases such as pain, infertility, and cancer, as well as diseases caused by stress are the areas with which modern medicine struggles and are highly likely related to blood stasis. 8 –14
Since the traditional medical concept of blood stasis is currently physiologically ambiguous, the term should be clearly defined if it is to be identified with relevant diseases according to present diagnostic standards. 5,15 –18 Accordingly, studies on blood stasis are needed to investigate the scientific aspects of the traditional concept and reinterpret it from a modern perspective, ultimately to lay the groundwork for integrating Korean medical treatment into the treatment of chronic and intractable diseases. 5,18
In the study titled “Convergence research of the diagnostic technology for blood stasis (CORE-DITEC-BS),” which was conducted for 5 years from 2013 to 2017, the Korea Institute of Oriental Medicine (KIOM) proposed a standardization plan for blood stasis. It established a modern concept of blood stasis, developed diagnostic tools and diagnostic indices for blood stasis, and identified biological indices related to blood stasis. 18
As part of this project, KIOM conducted a follow-up study in 2015 on patients with traffic accident sequela and post-traumatic pain conditions related to blood stasis that are frequently treated with Korean Medicine. The aim of this study was to investigate the effects of pain reduction by blood stasis treatment for blood stasis syndromes with traumatic injury.
Methods and Analysis
Study design
This study is a community-based single-center prospective pretest–post-test pilot study.
Participants
A target sample of patients was recruited from the Jaseng Hospital of Korean Medicine, Seoul, South Korea, from August 2015 to December 2015. The study protocol was approved by the Institute Review Board of Jaseng Hospital of Korean Medicine, Seoul, Korea (KNJSIRB2015-14). Written informed consent was obtained from each participant before study participation. A total of 73 participants were recruited through doctor referrals from the hospital. This study was conducted according to the Standard Operation Procedures training for every practitioner to unify the diagnostic process. Table 1 shows the study procedure.
Study Design Schedule
●: Item has to be carried out for the visit in all participations.
Inclusion and exclusion criteria
The participants who met all the following requirements were eligible for enrollment. The eligibility criteria were as follows: men or women between 20 and 70 years of age who gave their written informed consent to participate and agreed to comply with the study regulations; patients with a trauma that occurred within the past 2 weeks, bruising, and a pain score greater than a numeric rating scale (NRS) score of 7; individuals who consented to Korean medical treatment; and individuals who consented to blood sampling and the purpose of this study. The exclusion criteria were patients with any psychiatric condition that renders them unable to communicate; patients who were critically ill; pregnant women; or patients with any condition that could influence the study assessment.
Intervention
Acupuncture, herbal medicine, and wet cupping, which are Korean medical therapies generally performed to treat post-traumatic pain, were performed. No particular restrictions for the general Korean medical treatments were applied. Acupuncture for blood stasis syndrome was performed manually to the following points. Triple Energizer-reinforcing Saam acupuncture set: Zulinqi (GB41) with the reinforcing technique, Zhongzhu (TE3) with the reinforcing technique, Futonggu (KI20) with the reducing technique, Yemen (TE2) with the reducing technique, and Ashi points were mainly selected. 19 Dangkwisoo-san, which consists of nine commonly used herbal medicines (Angelicae Radix, Paeoniae Radix Rubra, Linderae Radix, Cyperi Rhizoma, Caesalpinia Lignum, Carthami Flos, Persicae Semen, Cinnamomi Ramulus, and Glycyrrhizae Radix), as herbal medicine treatment, and wet cupping on tender point (Ashi) were also performed. Patients who had a trauma within the past 2 weeks made a total of six visits during a period of 2 weeks, where the last visit was day 14 from the day of the first visit. The patients had to receive at least 6 sessions of treatment during the 2 weeks, with the subsequent treatment being performed within 3 ± 1 days after the previous treatment. Occasionally pro re nata clinical intervention was included in the study.
Outcomes
Tests for the following parameters were performed: trauma severity (bruise size and pain severity; NRS), the blood stasis questionnaire, oximetry, patient's satisfaction, and adverse events. Height, weight, and other demographic data were documented. Data regarding lifestyle factors, smoking, and alcohol consumption were also obtained.
Primary outcome
The primary outcomes of this study were the size of bruise (width and length in cm) and NRS score as pain severity indicator. Clinicians reported the size of bruise (width and length in cm) using the grid based on the largest and most severe bruise and attached a picture of bruise to the case report form (CRF). NRS is a segmented numeric version of the visual analog scale. In the NRS score, patients were asked to circle a number between 0 and 10 that fits best to their pain intensity (0 = no pain and 10 = severe pain).
Secondary outcomes
Oximeter measurement (SpO2, SpHb, PVI, SpOC, PR, SpMet, and PI)
Oximeter values were obtained using a multiwavelength Pulse CO Oximeter and adhesive sensor (Radical-7 Monitor and Rainbow Resposable Adhesive Sensor, Rev E; Masimo, Irvine, CA). Pulse oximetry is particularly convenient for noninvasive continuous measurement of blood oxygen saturation. It measured SpO2 (oxyhemoglobin), SpHb (total hemoglobin), PVI (pleth variability index), SpOC (oxygen content), PR (pulse rate), SpMet (methemoglobin), and PI (perfusion index). 20 Each patient's ring finger in the left hand should be attached fully to the detector so that there was no space between the finger and detector. The measure time was about 5 min and fixed values were reported when all the values were stabilized. The Min and Max values of PI were reported.
Blood stasis questionnaire
The questionnaires consist of various symptoms of blood stasis. 16,18 Each participant was seen independently by two experts from the same department, who completed the questionnaire. These assessments were conducted individually, with no discussion between the two experts, and were made on the same day without delay, to minimize the time difference between the two experts' diagnoses. Each variable was graded according to the following scores: 1 = very severe, 2 = severe, 3 = moderate, 4 = slight, and 5 = none. The average scores for the variables measured by two independent experts were calculated for statistical analysis, excluding data with a large discrepancy between scores reported by the two experts (i.e., |score difference| > 3) to control the quality of the data. It was performed twice, once each at the first and last visits.
Patient's satisfaction and degree of improvements
Patient's satisfaction was judged by items such as medical service and level of medical care, prompt response to inconveniences in the medical care process, and time of medical treatment.
The determination of the symptom improvement was based on the change of each item in the CRFs. Each variable was graded according to the following scores: 1 = very severe, 2 = severe, 3 = moderate, 4 = slight, and 5 = none. The physician's subjective opinion of the progress of the symptoms for 2 weeks was identified.
Adverse events
The presence or absence of undesirable and unintended symptoms caused by prescription and acupuncture treatment was also recorded.
Safety evaluation
A blood test was conducted at baseline to confirm the safety before taking herbal medicine. The data to be collected were as follows: AST (aspartate aminotransferase), ALT (alanine aminotransferase), ALP (alkaline phosphatase), creatinine, and BUN (blood urea nitrogen).
Statistical analysis
Of the patients with trauma for <2 weeks, those who were confirmed to have blood stasis by two Korean medical doctors on the first visit were evaluated. Basic analysis, including test categories and blood indexes, was performed for both the blood stasis and nonblood stasis groups. Categorical variables were presented as n (%), whereas continuous variables were presented as mean ± standard deviation (SD) or mean ± standard error (SE). Flow-up outcomes were compared with baseline values using either paired t-tests or Wilcoxon signed-rank tests, depending on whether or not the data were normally distributed. The missing values caused by failed measurements after the first visit were replaced using the last observation carried forward method. Statistical significance was set at p < 0.05. All analyses were conducted using the SAS system for windows, version 9.4 (SAS Korea, Seoul, Korea).
Results
The general characteristics of the study subjects are shown in Table 2. After examining the 73 patients to exclude nonblood stasis patients, 50 patients with blood stasis were identified (Fig. 1).
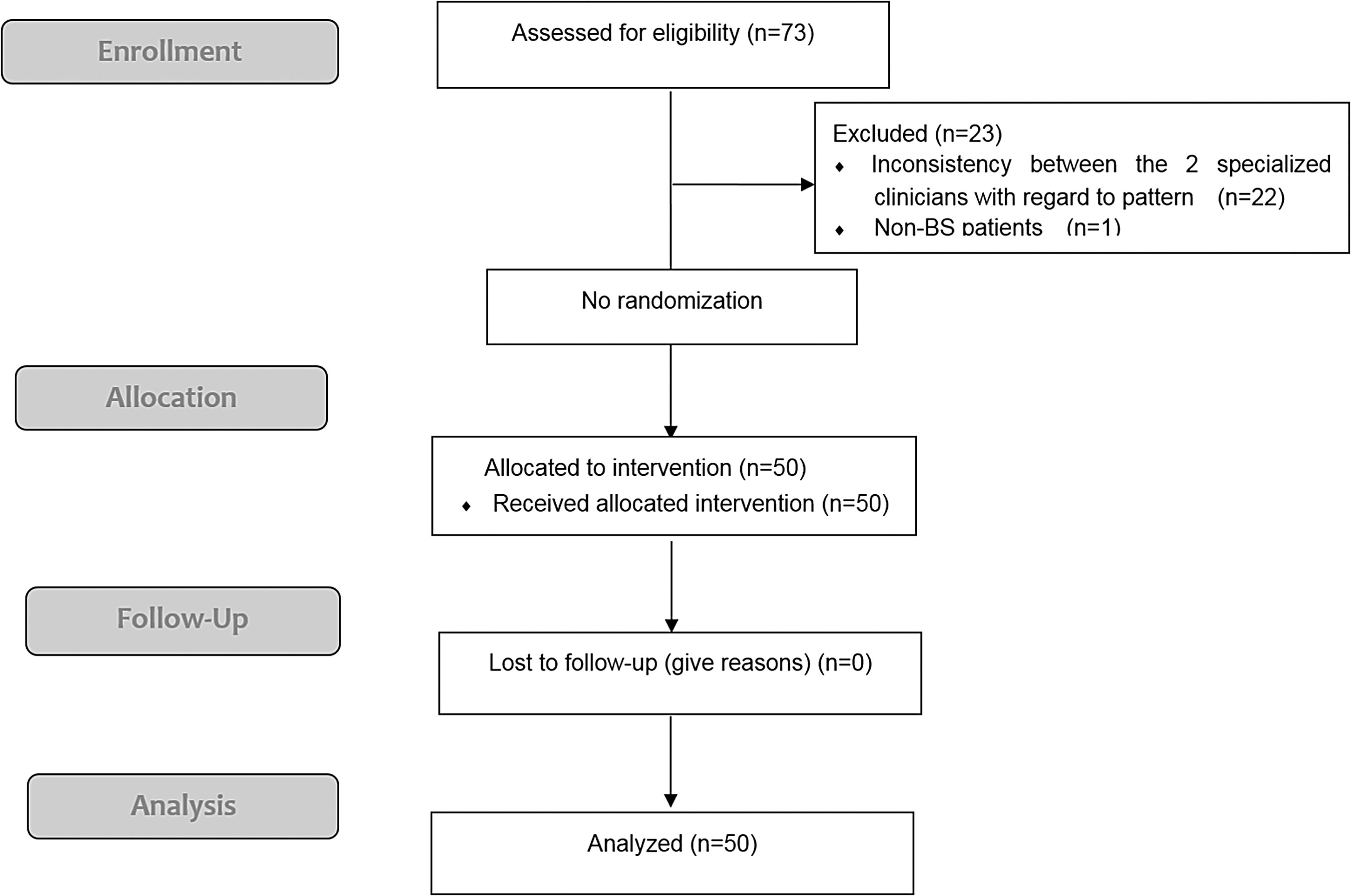
Flow chart of study design. non-BS, nonblood stasis.
Basic Characteristics of Study Participants
All data are presented as mean ± SD for continuous variables and as frequencies for categorical variables.
ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index; BUN, blood urea nitrogen; DBP, diastolic blood pressure; SBP, systolic blood pressure; SD, standard deviation.
Of the 50 patients analyzed in this study, 42 were women and 8 were men. They were mostly young adults (average age: 33.52 years, SD = 11.23 years). The proportion of patients diagnosed with blood stasis decreased 45% (n = 27) in the sixth visit after treatment (Fig. 2).
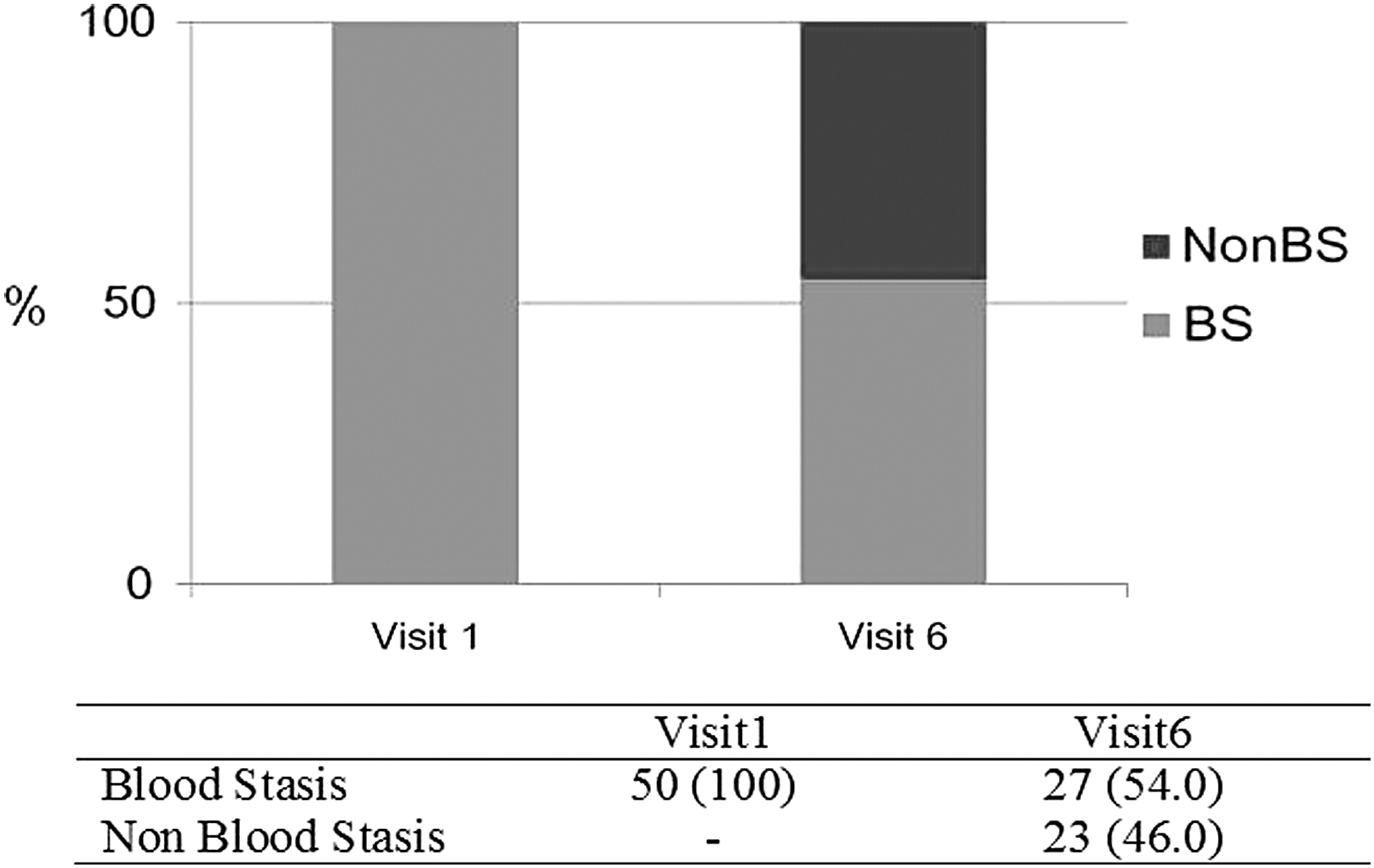
Changes in blood stasis distribution across visits. The proportion of patients with blood stasis decreased from 50 cases in the first visit to 45% (n = 27) in the sixth visit. BS, blood stasis; non-BS, nonblood stasis.
Changes in trauma severity across visits
In visit 1, mean ± SE values of NRS and size of subcutaneous bleeding (width and length in cm) were 7.45 ± 0.13, 4.26 ± 0.52, and 5.73 ± 0.60, respectively. In visit 6, mean ± SE values of NRS and size of subcutaneous bleeding (width and length in cm) were 1.36 ± 0.31, 1.32 ± 0.36, and 1.66 ± 0.54 (all, p < 0.01 compared with visit 1), respectively. The mean size of subcutaneous bleeding (width and length in cm) and NRS score as a general pain indicator significantly decreased over the visits (all p < 0.01, visit 1 vs. visit 6) (Fig. 3 and Supplementary Table S1.
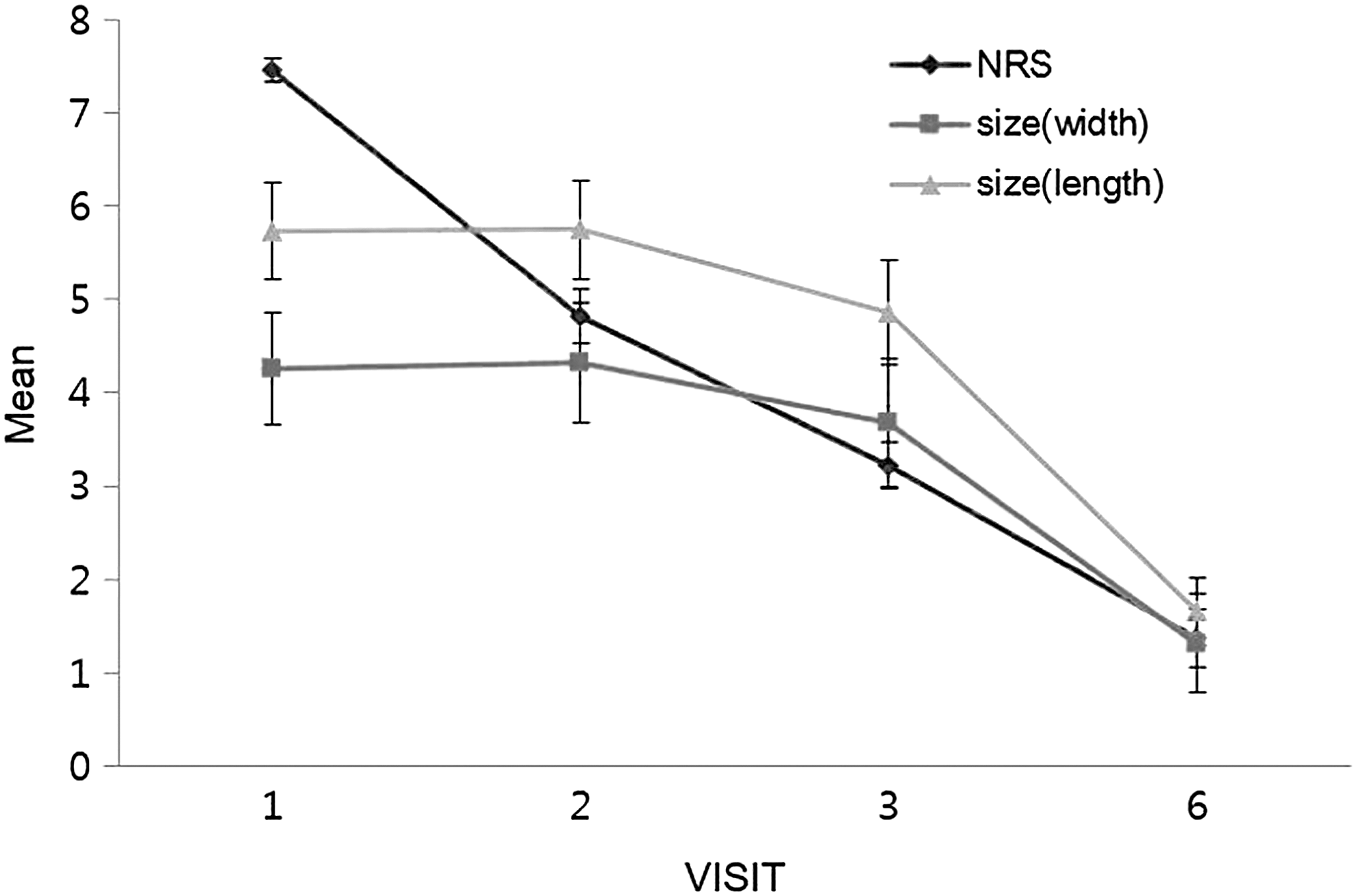
Changes in trauma severity across visits. In visit 1, mean ± SE values of NRS and size of subcutaneous bleeding (horizontal, vertical in cm) are 7.45 ± 0.13, 4.26 ± 0.52, and 5.73 ± 0.60, respectively. In visit 2, mean ± SE values of NRS and size of subcutaneous bleeding (horizontal, vertical in cm) are 4.82 ± 0.29 (p < 0.01 compared with visit 1), 4.32 ± 0.53, and 5.75 ± 0.64, respectively. In visit 3, mean ± SE values of NRS and size of subcutaneous bleeding (horizontal, vertical in cm) are 3.23 ± 0.24 (p < 0.01 compared with visit 1), 3.67 ± 0.56 (p < 0.05 compared with visit 1), and 4.86 ± 0.70 (p < 0.05 compared with visit 1), respectively. In visit 6, mean ± SE values of NRS and size of subcutaneous bleeding (horizontal, vertical in cm) are 1.36 ± 0.31, 1.32 ± 0.36, and 1.66 ± 0.54 (all, p < 0.01 compared with visit 1), respectively. NRS, numeric rating scale; SE, standard error.
Changes in the clinical indicators of blood stasis across visits
Changes in the clinical indicators of blood stasis were examined in 50 patients with blood stasis. The following traumatic pain indicators significantly decreased over the visits: “symptom (bruise, pain) from recent injury such as falling down or being involved in a traffic accident,” “painful ankle, wrist, and back sprain,” and “tends to bruise easily.” In addition, the following nonspecific symptom-related traumatic pain indicators showed significant improvement over the visits: “dark red lips,” “sublingual varicosities,” “dizziness,” “amnesia,” and “chronic pain in joints/palsies and numbness.” In addition, the female indicators “menstrual pains,” “dark menstrual blood,” and “dark lumps in menstrual blood” significantly decreased (Table 3). No other significant results were obtained, but 16 indicators showed a decreasing trend after treatment (Supplementary Table S2).
Results of Changes in Blood Stasis Index Between Visit 1 and Visit 6
Data are presented as mean ± SD; p-value by paired t-test.
Only women.
SD, standard deviation.
Changes in oximeter values across visits
Changes in oximeter values across the visits were examined in 50 patients with blood stasis, and the patients showed significant improvements in the Min and Max values of peripheral PI after the treatment (p = 0.011 and p = 0.15, respectively) (Table 4).
Results of Changes in Oximeter Values Between Visit 1 and Visit 6
Bold indicates significance at p < 0.05.
Data are presented as mean ± SD; p-value by paired t-test.
PI, perfusion index; PR, pulse rate; PVI, pleth variability index; SD, standard deviation; SpHb, total hemoglobin; SpMet, methemoglobin; SpO2, oxyhemoglobin; SpOC, oxygen content.
Patient satisfaction and improvement across visits/side effects and adverse events
In visit 1, mean ± SE values of patient satisfaction and improvement by physician's diagnoses were 3.04 ± 0.03 and 3.0 ± 0.0, respectively. In visit 6, mean ± SE values of patient satisfaction and improvement by physician's diagnoses were 4.70 ± 0.07 and 4.8 ± 0.06, respectively. And over the visits, the patients' satisfaction with treatment and improvement of symptoms significantly increased (all p < 0.01, visit 1 vs. visit 6) (Fig. 4 and Supplementary Table 3). With regard to the side effects and adverse events, one patient developed rashes on both arms and another patient had an abnormal vaginal bleeding before menstruation.
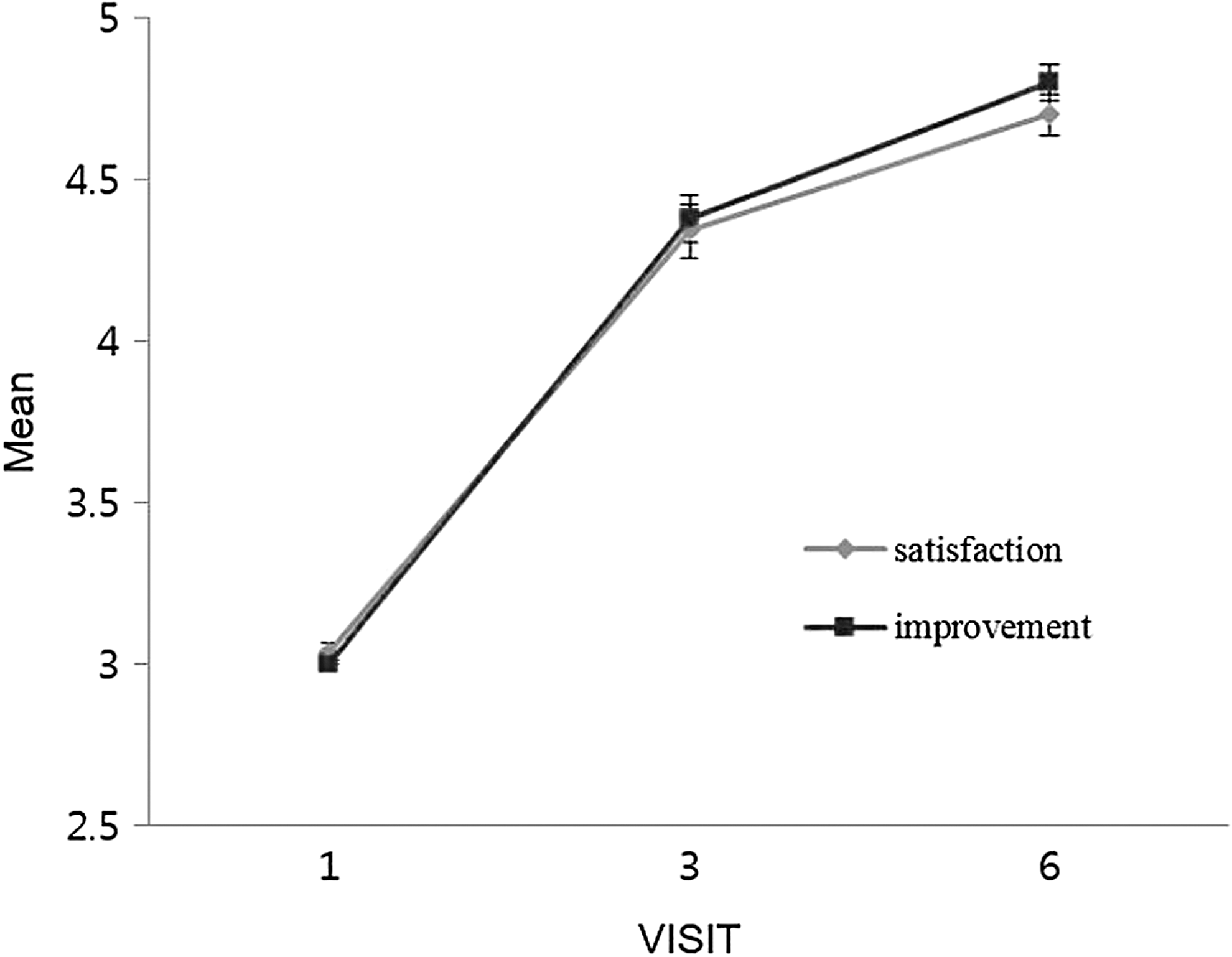
Changes in patient satisfaction and improvement across visit. Over the visits, the patients' satisfaction with treatment and improvements of symptoms significantly increased. In visit 1, mean ± SE values of patient satisfaction and improvement by physician's diagnoses were 3.04 ± 0.03 and 3.0 ± 0.0, respectively. In visit 3, mean ± SE values of patient satisfaction and improvement by physician's diagnoses were 4.34 ± 0.08 and 4.38 ± 0.07, respectively. In visit 6, mean ± SE values of patient satisfaction and improvement by physician's diagnoses were 4.70 ± 0.07 and 4.8 ± 0.06, respectively. SE, standard error.
Discussion
Blood stasis syndrome is one of the major syndromes in Traditional East Asian Medicine. 1 –4 In Korean Medicine, blood stasis is considered an important factor that induces diseases by obstructing the blood flow in the meridian system. If blood stasis occurs within the body, characteristic symptoms such as pain at fixed area, nyctalgia, dark-purple coloring of the face, tongue, sublingual varicosities, and blood spots under the skin or tongue can manifest. 5–6 In clinical practice, chronic and intractable diseases such as pain, infertility, and cancer, as well as diseases caused by stress are highly likely related to blood stasis. 6,7 –14
In the results, the proportion of patients with blood stasis decreased to 45% of the total patients in the sixth visit. In addition, the size of subcutaneous bleeding and NRS score as a general pain indicator significantly decreased over the visits. Among the blood stasis symptoms in the questionnaire, 11 blood stasis indicators significantly decreased or showed decreasing trends over the visits.
To make informed patient management decisions, physicians need to be aware of changes in peripheral perfusion/circulatory status, especially in patients who are in critical condition. 21 In Korean Medicine research, to objectively verify the effect of Korean Medicine, there are studies to observe the change of the evaluation index measured by instruments after Korean Medicine treatment. In these studies, cerebral blood flow enhancement and peripheral blood flow enhancement have been associated with improved symptoms of paralysis. 22 –25 There have also been similar studies in China. 26,27 Changes in oximeter values across the visits were examined in 50 patients with blood stasis, and the patients showed significant improvements in the peripheral PI after the treatment. The PI is the ratio of the pulsatile blood flow to the nonpulsatile or static blood in peripheral tissue. 19,28 PI can be seen to represent a noninvasive measure of peripheral perfusion that can be continuously and noninvasively obtained from a pulse oximeter. 28 –30 According to previous studies, 31,32 PI has been measured for evaluating pain, and the higher value means that pain would have decreased. In addition, PI will be a useful diagnostic tool to assess pain related to blood stasis.
In recent decades, many clinical studies for blood stasis have been conducted to reveal the correlation of blood stasis with diseases or physiopathology. 2,6 Many herbal formulas and many other herbs were shown to be significantly effective for various diseases, including traumatic conditions. 33 –36
In this research, there were no particular restrictions for the general Korean medical treatments for post-traumatic pain and all patients were prescribed with Dangkwisoo-san. Dangkwisoo-san, which consists of nine commonly used herbal medicines, is one of the most frequently prescribed herbal medicine for blood stasis syndrome patients in Korea. 34,35 It is effective to promote blood circulation and reduce pain caused by traffic accidents or injuries in clinic. 33 –36
There are some limitations in this study. This study design was a one-group pre–post-trial design and sample size was small. The one-group pretest–post-test design has been widely criticized, 37 but it can assess equivalency of groups with small sample size, and can be used to select participants for experiment. Second, there was no control group to confirm effects of blood treatment therapy. This study cannot ascribe changes of the blood stasis signs/symptoms/severity to the treatments that were given without a control group. To establish causal relationship, further study would probably be needed to include the following groups: an untreated control group, a blood stasis specifically treated group, and a nonblood stasis-treated control group. Third, contusions/bruises typically resolve without treatment for a >2 week period. The changes in size of the contusions may represent that phenomenon. Therefore, without a control group, there is no way to know the effect of blood stasis treatment on resolution of subcutaneous lesions. Despite the mentioned limitations, the findings of this study should be interpreted within the context of its limitations, and might not be appropriate for extrapolation to the general population. The significant results observed in this study support some evidence of the theories of diagnosing blood stasis pattern and treatments of that pattern in Korean Medicine.
Conclusions
Blood stasis syndrome is one of the major syndromes in Traditional East Asian Medicine. It has been considered to be a pathogenic factor in chronic and incurable conditions. In this study, the proportion of patients with blood stasis decreased after treatment. In addition, the size of subcutaneous bleeding and NRS score as a general pain indicator significantly decreased over the visits. Changes in oximeter values across the visits showed significant improvements in the peripheral PI after treatment. The study reveals that blood stasis treatment for traumatic injury may help improve reduction of pain. The significant results observed in this study support some evidence of the theories of diagnosing blood stasis pattern and treatments of that pattern in Korean Medicine.
Footnotes
Acknowledgments
This research was supported by a Grant from the Korea Institute of Oriental Medicine (K18191 and K18192). The authors thank the Gangnam and Daejeon branches of Jaseng Oriental Medicinal Hospital for this study.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.