
Abstract
Objectives:
Many patients with cancer use complementary and alternative medicine (CAM), but the quality of CAM documentation in their electronic health records (EHRs) is unknown. The authors aimed to describe (i) the prevalence and types of CAM used after cancer diagnosis and the influence of oncologists on CAM use, as per patients' self-report, and (ii) the prevalence of CAM documentation in the EHR and its consistency with self-reported usage.
Design:
Patient and provider surveys and chart review.
Settings/Location:
Medical oncology practices at one institution.
Subjects:
Patients with cancer at oncologist visits.
Outcome measures:
Patient self-reported rate of 3-month postvisit CAM use; provider EHR documentation of CAM use or discussion and its concordance with patient self-report.
Results:
Among 327 patients enrolled, 248 responded to the 3-month postvisit survey. Of these, 158 reported CAM use after diagnosis (63.7%). CAM users were younger (p < 0.001) and had a higher percentage of women (p = 0.03) than nonusers. Modalities most commonly used were supplements (62.6%), special diets (38.6%), chiropractor (28.4%), and massage (28.4%). CAM was used to improve well-being (68.7%), manage adverse effects (35.5%), and fight cancer (22.9%). Oncologists suggested CAM in 22.5% of instances of use. CAM use/discussion was documented for 58.2% of self-reported CAM users. Of the documented modalities, EHR and self-report were concordant for only 8.2%. CAM documentation was associated with physician provider (p = 0.03), older patients (p = 0.01), and treatment with radiation (p = 0.03) or surgery (p = 0.001). After adjusting for other factors, patients with breast cancer or “other” tumor category were four times more likely than patients with gastrointestinal cancer to have CAM use documentation (odds ratio [95% confidence interval]: 4.41 [1.48–13.10]; 3.76 [1.42–9.99], respectively).
Conclusions:
Most patients with cancer use CAM after diagnosis, yet EHR documentation is complete for very few. Oncologists should inquire about, document, and discuss CAM benefits and harm or refer patients to CAM specialists.
Introduction
C
The electronic health record (EHR) functions as a record of treatments and provider interactions in conventional healthcare. Retrospective assessment of the EHR to determine whether CAM was discussed during cancer visits presupposes that content was documented and was accurate. Yet little is known about the prevalence and accuracy of documenting CAM in the EHR 10 and its relationship to patient self-reported use.
The purpose of this study was to examine the frequency of documentation of CAM use/discussion in the EHR among cancer patients who self-reported using CAM after their cancer diagnosis. The authors sought to understand factors associated with CAM documentation in the EHR.
Methods
Setting and population
This study was approved by the Mayo Clinic Institutional Review Board. Adult patients (age ≥18 years) seen at new or return visits to medical oncology practices at Mayo Clinic in Rochester, Minnesota were enrolled from June 2012 through April 2014. The patients represented most tumor types and a range of points on the cancer care continuum. This cohort was part of a multicenter study previously described. 11 Patients were enrolled in the study for 3 months after the observed oncology visit, at which time they completed a postvisit questionnaire that included self-reported CAM use.
Survey instruments
Paper surveys were administered to participants in person at the baseline visit (before and after provider encounter), and a 3-month postvisit patient survey was mailed, as described by Kimball et al. 11 The 3-month postvisit survey inquired about usage of 17 CAM modalities: acupuncture, biofeedback, chiropractic care, energy healer/healing touch/reiki, hypnotherapy, massage therapy, traditional healer, aromatherapy, guided imagery, herbal medicine, homeopathy, meditation, special diets, supplements/megavitamins, t'ai chi/qigong, yoga, and home remedy. For each CAM modality used, the following characteristics were queried: timing of use in relation to the cancer diagnosis (never, only before, only after, or both before and after), reasons for use (fight cancer, manage adverse effects, improve well-being, or other), whether the patient informed the clinician of CAM use after diagnosis (yes or no), and the role of the oncology clinician in patients' usage of CAM (no role, no opinion, suggested use, or cautioned against use). Instances of CAM use and documentation are reported as the total number of uses within a modality (i.e., number of patients reporting a modality) and a sum of all modalities for patients (i.e., number of modalities reported overall and by patient).
Patient demographics were gathered with a 25-question pre-encounter survey. A 23-item baseline questionnaire was administered to all clinicians—physicians and advanced practice nurses who were willing to participate—assessing sex, age, race and ethnicity, year of medical/nursing school graduation, and type of oncology practice by organ.
EHR abstraction
Two reviewers (D.L.S. and D.L.W.-R.) independently abstracted patients' available EHR data about documented CAM use, during all medical encounters (not restricted to oncology clinicians), from the diagnosis of cancer until 3 months after the baseline visit. Abstracted data included date of cancer diagnosis, organ of primary cancer, stage, cancer treatment (surgery, cancer-related drugs, and radiotherapy), referral to the integrative medicine clinic, and CAM modalities documented in the EHR as being used or discussed (same CAM modalities investigated in the patients' survey).
Concordance grading
CAM modalities documented in the EHR as being used or discussed were compared independently with the modalities used after cancer diagnosis as indicated by self-report in the 3-month postvisit survey. Use “after” diagnosis included patients who reported use “only after” and use “both before and after” diagnosis. Each instance of self-reported CAM use was rated in comparison to the EHR documentation as concordant, incomplete, discordant, or absent. Concordant meant a perfect match between self-report and documentation. Incomplete meant a less-than-perfect match (e.g., the EHR only captured part of the modalities self-reported as used by the patient). Discordant meant self-reported use but the documentation did not match at all (e.g., the EHR contained CAM modalities that were different from those listed by the patient as being used). Absent meant no mention of CAM use in the EHR. Both reviewers assessed concordance and resolved discrepancies by consensus.
Statistical analysis
Initial study data were collected and managed using REDCap electronic data capture tools hosted at Mayo Clinic in Rochester, Minnesota. 12 Additional data were collected through chart review.
Self-reported CAM use and CAM documentation were compared among categorical patient and clinician characteristics with a chi-square (χ 2 ) test. Similar comparisons for continuous variables were made using Wilcoxon rank sum or Kruskal–Wallis test, as appropriate. The authors conducted a hierarchical generalized linear model with CAM documentation as the outcome to assess level of associations with independent variables. Because clinician factors may affect documentation, the authors clustered the model on the clinician. Distributions for continuous variables were checked and approximated as normal. The multivariate model of CAM documentation was adjusted by factors shown to be statistically relevant univariately at p-values <0.15. A sensitivity analysis was conducted on remaining factors to determine whether results changed if the model was adjusted by each factor separately. The authors did this by comparing the Akaike information criterion values of the model with and without the factor (patient sex, patient education level, treatment with cancer drugs, clinician sex, and clinician age) and by assessing the effect of estimates, the standard error, and significance. This led us to include treatment with cancer drugs in the final model. Statistical analysis was performed using SAS software, version 9.4 for Unix (SAS Institute, Inc.) and Stata (StataCorp 2015 Stata Statistical Software: Release 14).
Results
Factors associated with self-reported CAM use
Of 375 patients approached to participate, 336 agreed and 327 were enrolled. Of these, 248 returned the 3-month follow-up survey. Among these 248 patients, 158 (63.7%) reported CAM use after the cancer diagnosis. Comparison of patient, disease, and clinician characteristics between those with and without self-reported CAM use is shown in Table 1. CAM use was associated with younger age (mean, 59.9 vs. 67.1 years; p < 0.001) and female sex (p = 0.03). There was no correlation between CAM use and clinician characteristics (age, sex, medical doctor vs. advanced practitioner) or disease characteristics (stage IV vs. others, treatments received, organ of primary cancer). Race was statistically significant when categorized as white versus other with regard to CAM use (p = 0.04).
Values are no. of persons (%), unless otherwise indicated.
Wilcoxon rank sum test for continuous comparisons; χ 2 test (or Fisher exact text for n < 5) for categorical comparisons.
CAM, complementary and alternative medicine; MD, medical doctor; SD, standard deviation.
CAM modalities used, reason for use, and role of the oncology clinician
The 158 patients self-reporting use of CAM after the cancer diagnosis often affirmed using multiple CAM modalities (median, 2; range, 1–14 modalities), for a total of 561 instances of CAM used (85 “only before,” 172 “only after,” and 304 “both before and after” diagnosis). The most commonly used modalities were supplements (62.6%), special diets (38.6%), chiropractor (28.4%), massage therapy (28.4%), and meditation (25.3%) (Fig. 1).

Use of various CAM modalities by self-report among those who reported using CAM (n = 158). CAM, complementary and alternative medicine.
On the basis of data from 79 patients who reported details of their supplement use (20 participants taking supplements did not elaborate), the most commonly taken supplements were fish oil (52%), multivitamins (32%), glucosamine (28%), vitamin C (22%), and vitamin B complex (19%).
Patients often affirmed using CAM modalities for multiple reasons. Reasons for use of CAM were to improve well-being (327, 68.7%) followed by managing adverse effects (169, 35.5%) and fighting cancer (109, 22.9%). The most common modality used to improve well-being was supplements. Reasons for use of individual CAM modalities are shown in Figure 2.

Reasons for CAM use by modality. CAM, complementary and alternative medicine.
In 96% of CAM use instances (n = 457), the participants reported informing their oncology clinician about their CAM use. Yet for most instances of CAM use, patients reported that the oncologist had no role in the usage (249 instances, 52.3%). The reported CAM usage was suggested by the oncology clinician in 107 instances (22.5%). Per patient self-report, the oncology clinician had no opinion of the CAM use in 75 instances (15.8%) and was opposed to the CAM use in only 12 instances (2.5%). Among the 107 instances in which patients said clinicians suggested CAM usage, the most commonly suggested were supplements (31, 29.0%), special diets (25, 23.4%), massage (10, 9.4%), and acupuncture (10, 9.4%).
Prevalence and quality of EHR documentation of CAM use/discussion
Of the 158 CAM users, 92 (58.2%) had some sort of EHR documentation of CAM use/discussion between the cancer diagnosis and up to the 3-month poststudy visit; some had more than one modality documented, for a total of 167 instances of CAM documentation. Thus, 41.7% of patients using CAM had no documentation of it in the EHR. When reported, modalities most frequently documented among 158 patients were supplements (69, 43.7%), massage (23, 14.6%), herbal remedies (21, 13.3%), chiropractor (21, 13.3%), acupuncture (9, 5.7%), and yoga (8, 5.1%). Among CAM-using patients based on self-report, the EHR documentation of CAM was concordant with patient self-report in just 13 patients (8.2%), incomplete in 53 (33.5%), discordant in 25 (15.8%), and absent in 66 (41.7%). By modality, the most accurate documentation was for supplements (49 of 99 patients, 49.5% concordance), acupuncture (7 of 22 patients, 31.8% concordance), and herbal remedies (9 of 29 patients, 31.0% concordance) (Fig. 3). Ten of the 158 CAM users (6.3%) were referred to CAM/integrative medicine specialists.
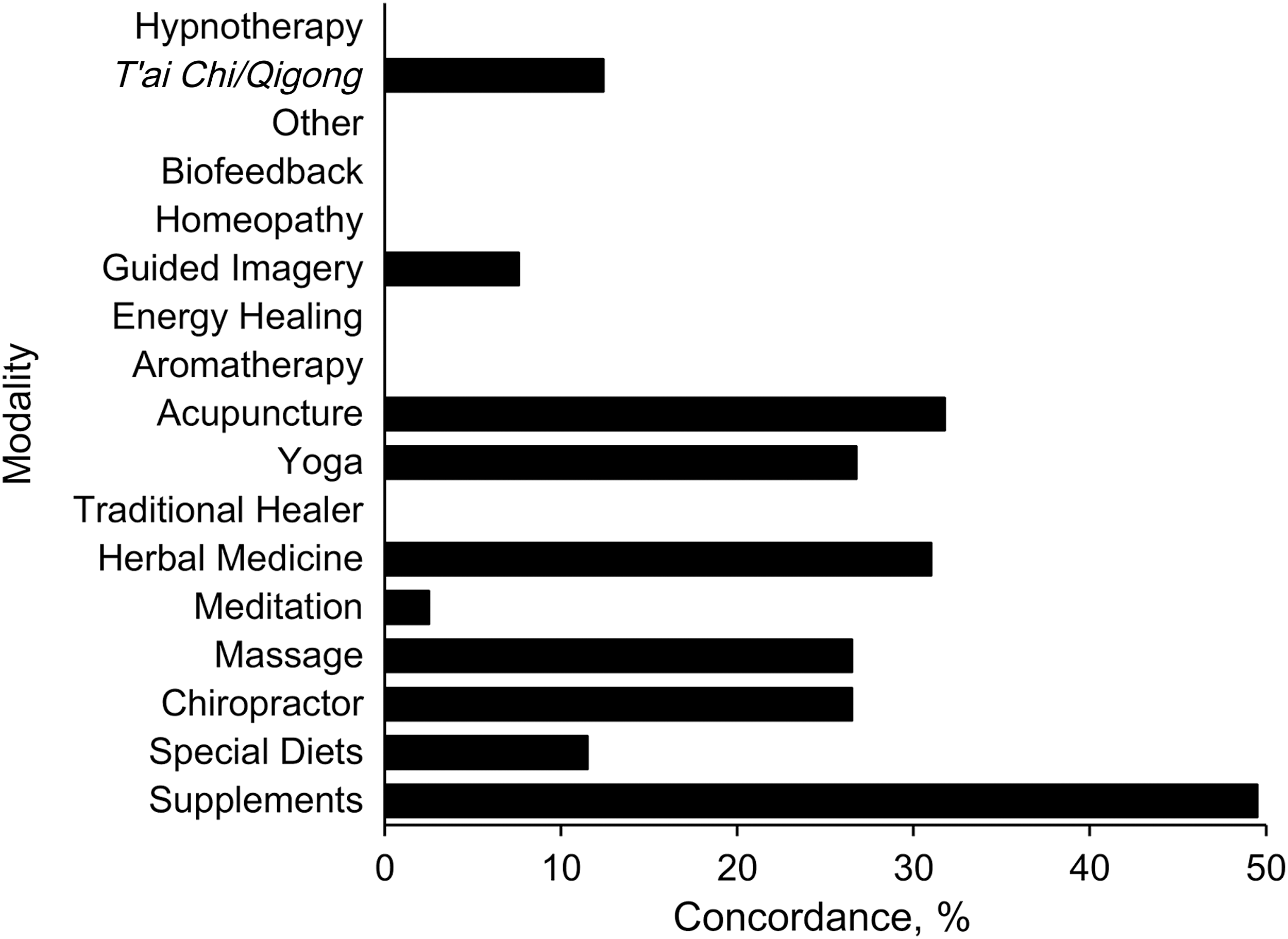
Concordance of self-reported CAM use with electronic health record documentation by modality. CAM, complementary and alternative medicine.
Characteristics associated with EHR documentation of CAM use/discussion in self-reported CAM users
Characteristics associated with the presence of any documentation (vs. no documentation) were tumor type (with breast cancer and “other” being more likely to have CAM documented than gastrointestinal cancer; p = 0.01), being seen by a physician provider (92.4% vs. 78.8%; p = 0.03), and older patient age (62 vs. 57 years; p = 0.01) (Table 2). Patients treated with surgery (p = 0.001) or radiation (p = 0.03) were more likely to have EHR documentation of CAM.
Values are no. of persons (%), unless otherwise indicated.
Wilcoxon rank sum test.
χ 2 test.
Generalized linear model.
CAM, complementary and alternative medicine; MD, medical doctor; SD, standard deviation.
Multivariate model of characteristics associated with CAM documentation
After accounting for cancer stage (IV vs. other), radiation treatment, surgery, and the type of clinician, older patients were more likely to have CAM documentation. Each year of age increased the likelihood of documentation by ∼4% (odds ratio [OR], 1.03; 95% confidence interval [CI], 1.01–1.06; p = 0.02). After adjusting for other factors, patients with breast cancer or “other” tumor category were four times more likely than patients with gastrointestinal cancer to have CAM use documentation (OR [95% CI]; 4.41 [1.48–13.10]; 3.76 [1.42–9.99], respectively). Documentation was not affected by treatment with radiation or surgery, stage of cancer, or type of clinician in the multivariate model. The intraclass correlation coefficient was 0.08 (95% CI, 0.0–0.21), which showed the presence of a weak clustering effect by clinician (Table 3).
Per 1-year increase in age.
CAM, complementary and alternative medicine; CI, confidence interval; MD, medical doctor; Ref, reference.
Discussion
Their study found that a high percentage of cancer patients use CAM after their cancer diagnosis (63.7%), and a vast majority of CAM usage (96%) was reported to their oncology care team. Only half of CAM users, however, had any CAM use documented in the EHR, and this documentation, when present, was rarely concordant with patients' self-report (8%). Very few patients who reported CAM use since receiving a cancer diagnosis (6%) received consultative support from integrative medicine experts.
Of the instances of CAM modalities used by their participants, 22.5% were suggested by the oncologist, per patient report; the modalities were most frequently supplements, special diets, massage, and acupuncture. During treatment of a life-threatening disease, discussing CAM may seem less crucial to conventionally trained clinicians. Indeed, the literature suggests that few oncologists initiate discussions of CAM therapy, except in the palliative setting. 13 However, CAM specialists are increasingly common at academic centers and available at most National Cancer Institute—designated comprehensive cancer centers, which suggest that the supportive needs of patients can be met in multiple ways. Because many patients believe that their oncologist is not well informed about CAM (84%), 14 patients may embrace a referral to a CAM expert. These experts may be especially helpful in reviewing harms posed by possible interactions of supplements with conventional medicines but also can discuss broader topics related to survivorship, including nutrition, fatigue, and stress management.
Despite a high rate of CAM use being reported to the oncologists in their study, the rate of EHR documentation was much lower and had very low concordance with self-report. The highest concordance rate was for supplement use (49.5%), which likely reflects the medication reconciliation process, which includes supplement use, taking place at their institution. Despite this process, the rate of capture of supplement use is less than perfect, which suggests that patients' disclosure of supplement use is incomplete, that the thoroughness of the reconciliation process is less than desired, or that patients' understanding of a “supplement” differs from that of the medical community.
The literature indicates that patients are reluctant to disclose use of CAM to their clinician and that supplement use is rarely documented. 15 –18 Their findings may challenge these generalizations. Most CAM documentation data come from studies of dietary supplements in geriatric populations with chronic diseases and polypharmacy. One such study among older adults, which compared the use of supplements, vitamins, and antiaging medications by self-report versus chart documentation by physicians, reported an overall documentation rate of 35%. 10 The highest rate was for supplements (50%), similar to their study. A study of 558 inpatients that assessed concordance between self-report and EHR documentation of supplement use reported that, although 38% had EHR documentation, only 20% were asked about supplement use and 18% disclosed use to clinician, and only 6% had concordant EHR documentation. 17
These data suggest a substantial gap remaining in the practice patterns of the U.S. Healthcare system to elicit and then competently document CAM use by patients. Models for doing so exist. Integrating a pharmacist into a geriatric oncology team has been shown to improve documentation of supplement use and possible drug interactions. 19
In their study, patients with breast cancer, older patients, and those who had surgery or radiotherapy as a treatment modality were more likely to have EHR documentation of CAM use or discussion. Breast cancer patients are far more consistent CAM users 20 and tend to be more active in seeking CAM information, 21 than patients with tumors at other sites. The reason for this may be that a great majority of those with breast cancer are women, and women have higher rates of CAM use than men. 22,23 Given this attitude, coupled with the high incidence of breast cancer compared with other cancers, the oncologists treating these patients might be more in tune to the risks and benefits of CAM modalities in this patient population, which might explain the more frequent EHR documentation. In older patients, the more frequent documentation of CAM might be explained by the concern about medication–supplement interactions, although the authors did not specifically examine which CAM modality was more commonly documented by age group.
Given the consistently high rates of CAM use and the challenges of oncology care teams in meeting patients' needs on this topic, system solutions to address those needs could be devised. These might include defaults for annual integrative health visits that include reviewing supplements by trained pharmacists or nurse practitioners as part of survivorship care planning. Other models might include having quick available resources such as interaction grids or question prompt lists available at the point of care to at least initiate a conversation about herb–drug interactions, arguably the most important safety-related issue in cancer patients' CAM use.
Patient-centered survivorship care presupposes systems and highly functioning care contexts with workflows to accommodate patient needs and questions. The authors posit that improving documentation of CAM in oncology practices is a necessary antecedent to the ability to demonstrate benefits (or harms) of CAM services and should be part of a team-based, whole-person approach to cancer care.
This study has several limitations. The data are cross-sectional and self-reported, with retrospective chart review. Incomplete ascertainment from the EHR is possible, and causality cannot be established from their study design. It is possible that the limited documentation concordance the authors found results from unsupportive systems that make documentation of CAM difficult. Just because something was not documented, does not mean patients were harmed. The results of this study are limited to one academic medical center and may not be generalizable or able to be extrapolated to other contexts such as community oncology practices. Nevertheless, the authors believe that the state of CAM documentation in their center could represent a best-case scenario because CAM service delivery in community practices may be even more fragmented. Such practices may lack systems to document and track CAM use, and EHRs may be less common. Although unlikely, documentation of CAM use may have been present in the EHR of patients not endorsing CAM use after cancer diagnosis. The authors did not review the EHR for these patients, so some of the discrepancies between self-report and documentation of CAM use may have been missed. The authors also could not distinguish whether CAM documented in the EHR represented an instance of CAM use, a discussion, or an active recommendation by the provider.
In summary, this study demonstrates that a large proportion of oncology patients who use CAM as an adjunct to their oncology treatment report sharing this with their oncologist, but the systems for documenting that use and referring patients to consultative resources with the capacity to help answer their questions are still very flawed.
Footnotes
Acknowledgments
This publication was made possible by the Mayo Clinic CTSA through grant number UL1 TR000135 from the National Center for Advancing Translational Sciences (NCATS), a component of the National Institutes of Health (NIH) and the AT006515 from the National Center for Complementary and Integrative Health.
Author Disclosure Statement
No competing financial interests exist.