
Abstract
Background:
To address the side effects of anticancer treatments, the Clinic for Complementary Medicine and Diet in Oncology was opened, in collaboration with the oncology department, at the Hospital of Lucca (Italy) in 2013.
Aim:
To present the results of complementary medicine treatment targeted toward reducing the adverse effects of anticancer therapy and cancer symptoms, and improving patient quality of life. Dietary advice was aimed at the reduction of foods that promote inflammation in favor of those with antioxidant and anti-inflammatory properties.
Methods:
This is a retrospective observational study on 357 patients consecutively visited from September 2013 to December 2017. The intensity of symptoms was evaluated according to a grading system from G0 (absent) to G1 (slight), G2 (moderate), and G3 (strong). The severity of radiodermatitis was evaluated with the Radiation Therapy Oncology Group (RTOG) scale. Almost all the patients (91.6%) were receiving or had just finished some form of conventional anticancer therapy.
Results:
The main types of cancer were breast (57.1%), colon (7.3%), lung (5.0%), ovary (3.9%), stomach (2.5%), prostate (2.2%), and uterus (2.5%). Comparison of clinical conditions before and after treatment showed a significant amelioration of nausea, insomnia, depression, anxiety, fatigue, mucositis, hot flashes, joint pain, dysgeusia, neuropathy, and all symptoms. Moreover, in a subgroup of 17 patients in radiotherapy undergoing integrative treatment, the level of toxicities and the severity of radiodermatitis were much lower than in the 13 patients without integrative treatment. Twenty-one cancer patients (6.2%) either refused (18) or discontinued (3) conventional anticancer treatment against the recommendation of their oncologist; after the integrative oncology (IO) visit, 7 (41.2%) out of 17 patients with follow-up decided to accept standard oncologic treatments.
Conclusions:
An IO clinic may contribute to reducing the adverse effects of anticancer therapy and improving the quality of life of cancer patients.
Introduction
R
In Europe, recourse to CMs in cancer care varies greatly from country to country (15%–73%). Treatments most frequently used are homeopathy, herbal medicine, and spiritual therapy, as per a large number of published surveys. 5
The most recent survey, conducted in five Italian hospitals on 468 patients with different tumors, showed a 48.9% incidence of previous or recent use of CMs. Interestingly, the use of CMs mainly derived from self-prescription (67%), with most patients being unaware of the potential interactions and side effects. 2
In oncology settings, complementary therapies are generally used with the intent of enhancing wellness, improving quality of life, and relieving the symptoms of the disease and the side effects of standard care. This combination of CMs and conventional antitumor therapies is commonly referred to as “integrative oncology” (IO).
Aim
The aim of this study is to provide an overview and describe the results of evidence-based complementary and integrative treatments and dietary advice given to cancer patients at the Clinic for Complementary Medicine and Diet in Oncology at the public Campo di Marte Hospital in Lucca, Tuscany (Italy), for a 4-year period (September 2013–December 2017). Integrative treatment was aimed at reducing the adverse effects of anticancer therapy and the symptoms of cancer to improve patients' quality of life. Furthermore, dietary advice was aimed at reduction of foods that promote inflammatory processes (i.e., red and processed meat) in favor of those with antioxidant and anti-inflammatory properties such as vegetables and certain types of fruits.
Methods
Design
This is a retrospective observational study on 357 consecutive cancer patients visited at the Clinic for Complementary Medicine and Diet in Oncology from September 2013 to December 2017.
Setting
The setting for this study was the Clinic for Complementary Medicine and Diet in Oncology at the public Campo Di Marte Hospital in Lucca, Italy. This outpatient clinic is open 1 day a week and provides cancer patients with the opportunity to meet with a CM expert, together with an oncologist who collaborates in the evaluation of the state of the disease, the test results, the prognosis, and the results obtained. Patients receive integrative treatment with the goal of reducing the adverse effects of anticancer treatment and the symptoms of cancer, as well as dietary advice. All the IO visits within the public regional healthcare system are completely free of charge for all cancer patients.
Nearly all the patients are referred by their medical oncologists at the oncology department of Lucca, but self-referred patients can also book an appointment through the clinic's secretary. Average wait times for a visit are between 1 and 2 weeks. There are no specific eligibility criteria.
The diagnostic–therapeutic assistance path for IO patients is shown in Figure 1.
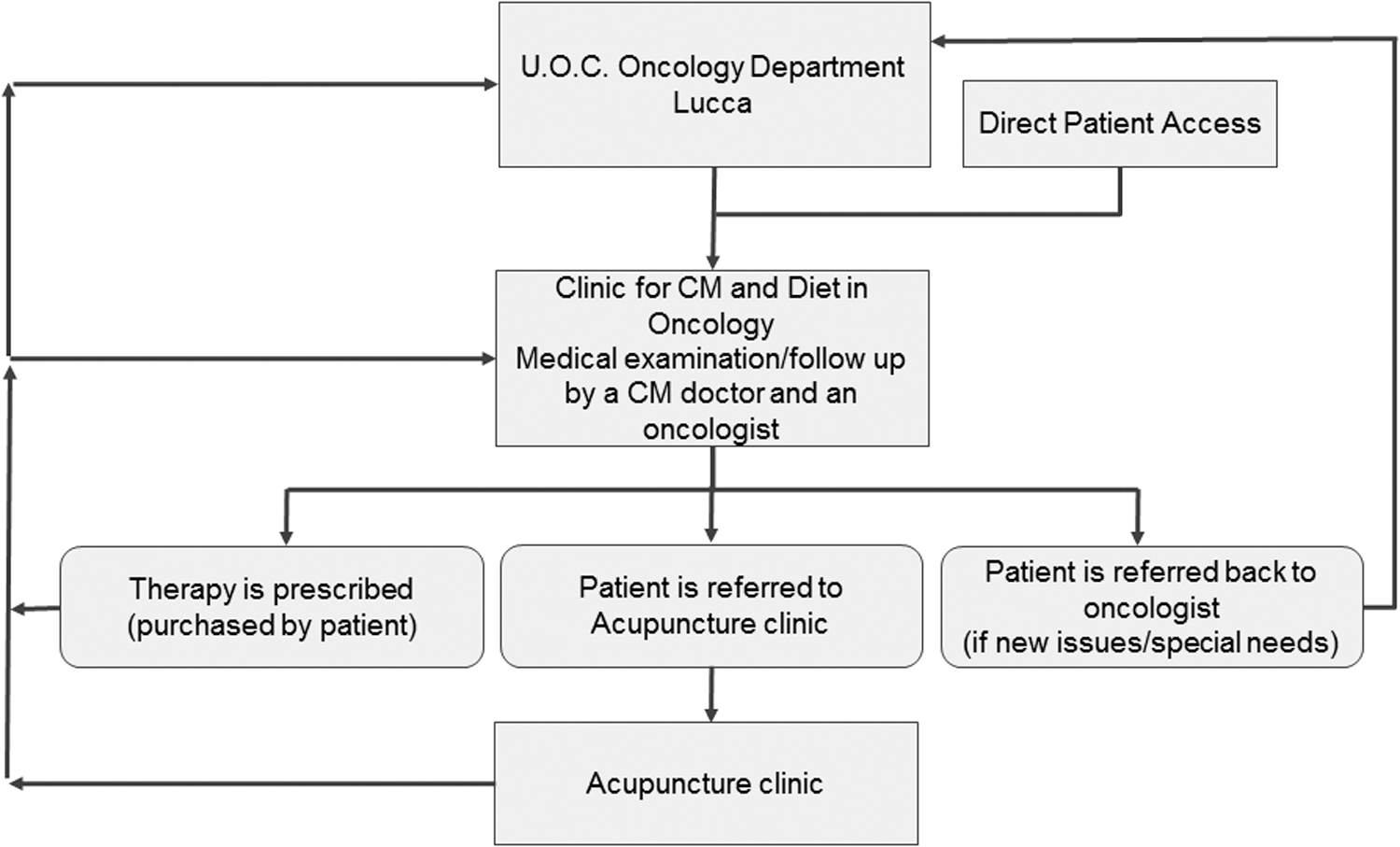
The DTAP for integrative oncology patients in Lucca. DTAP, diagnostic–therapeutic assistance path.
Informed consent
All the patients included in this study were asked to sign a privacy disclaimer and an informed consent form for treatment and the use of their data for future analysis. The informed consent form explicitly stated that any complementary therapies prescribed should not in any way substitute anticancer therapies prescribed by their referring oncologist. An individual identification number was assigned to each patient so that the data could be anonymized, collected, and stored in a database.
Patients
The sample was made up of 357 patients, 294 (82.5%) women, and 63 (17.5%) men, consecutively visiting the clinic from September 2013 to December 2017. Mean age was 56.5 years, with the mean age of men being higher than that of women, 61.1 versus 55.5 years, respectively (Table 1). As of the present writing, the clinic was not been asked to work with pediatric cancer.
Among others: brain tumors, 1.5%; pancreas, 1.2%; kidney, 1.2%; esophagus, 0.9%; bladder, 0.9%.
Almost all the patients (327 or 91.6%) were receiving or had just finished some form of anticancer therapy: chemotherapy (CT) was the most used therapy (30% used it exclusively and 36.6% associated with other therapies); endocrine therapy (ET) was used exclusively in 8.7% of cases and associated with other therapies in 34.4%; and radiotherapy (RT) was used exclusively in 4.2%.
The number of patients not undergoing any therapy was low (30 or 8.4%). Of these, 21 (6.2%) refused or decided to discontinue conventional anticancer therapy for curable cancer, whereas 13 (3.6%) did not receive CT as it was not recommended because it was not indicated or not tolerated.
Integrative treatment
Integrative complementary treatment at the clinic uses different therapies such as homeopathic remedies, botanicals and other food supplements, and acupuncture, often with specific integrative protocols to prepare patients for RT, CT, and ET.
Table 2 shows the most frequently prescribed homeopathic, botanical, and other therapies in detail. In every prescription of botanicals, the risk of possible pharmacologic interference with anticancer therapies underway is evaluated and the use of botanicals such as Hypericum perforatum 6 or foods such as grapefruit is suspended, 7 which are known for their ability to interfere with different types of pharmaceuticals, including anticancer drugs. These are extremely important considerations 8 that often lead clinicians to avoid using these substances even when the risk of interference is minimal, if not absent. For this reason, the Lucca clinic applies the so-called reversed grading, whereby the principal level of evidence of possible interaction corresponds to the main level of the negative recommendation. 9 This method, suggested by the Tuscan Network of Integrative Medicine, aims at improving the interpretation of in vitro and/or in vivo interactions between medicinal plants and CT for clinical application. This classification also includes the positive interactions (synergies) between medicinal plants and drugs. For instance, H. perforatum has IA of reversed grading (I, quality of evidence and A, strength of recommendations) and, therefore, must not be prescribed during oncologic therapy; this herb is associated with laboratory evidence in vitro and in vivo and clinical reports of pharmacologic interference with a proven risk of reducing the effectiveness of anticancer therapy. In contrast, Curcuma longa, which has no toxicity, side effects, or negative interferences reported, and also has cumulative effects with gemcitabine and oxaliplatin, has VB grading (no evidence of negative interference and positive evidence of oncological therapy potentiation), which means that it can be used during oncologic therapy.
In the case of RT, the clinic utilizes a protocol that provides for homeopathic treatment with Radium bromatum before the therapy and Belladonna (or in some cases Apis mellifica or Cantharis), all given in low potencies, from 5CH to 9CH, accompanied by an alkalizing treatment based on citric acid and baking soda, followed by Calendula cream occasionally alternated with Aloe gel. 10
All patients are provided with dietary advice and, in some cases when needed, psychological counseling (psycho-oncology) and acupuncture (4.5% of patients).
No serious adverse reactions or drug interactions due to complementary therapies have been reported to date.
Dietary advice
To improve their clinical situation, cancer patients are given evidence-based dietary and lifestyle advice. 11 Patients are advised to eliminate or reduce (1) refined carbohydrates, in particular white sugar and flour, to reduce glycemic load and hyperinsulinemia; (2) red meat, including charcuterie, to reduce chronic inflammation; (3) harmful substances such as alcohol in large quantities and tobacco; and (4) foods for which there is a documented food intolerance.
Patients are also encouraged to consume (1) preferably small-sized and wild-caught fish, such as mackerel, anchovies, sardines, and mullet; (2) certain spices (turmeric, pepper, and ginger); (3) organic, whole wheat bread, and pasta and other grains (e.g., spelt, kamut, amaranth, and quinoa) and brown rice to promote intestinal motility; (4) a small amount of preferably organic sulfite-free red wine (one glass/day maximum); (5) cruciferous vegetables with antioxidant properties (e.g., cabbage, broccoli, and Brussels sprouts); (6) foods containing lignans for antiestrogenic activity (seeds or oils of flax, sesame, and/or Cruciferae); and (7) fruits containing ellagic acid such as apricots, berries (raspberries, blackberries, and currants), and pomegranate to inhibit cancer angiogenesis. 12
All patients have their blood levels of vitamin D checked and, when necessary, are advised to supplement it until normal levels are reached. 13,14 Finally, all cancer patients are asked to engage in at least 40 min of physical activity daily, if possible. 15
Study procedures
To assess the response to integrative treatments, patients who had at least one follow-up were re-examined. In general, the first follow-up measurement was taken within 1 or 2 months from the first visit and thereafter every 1, 2, or 3 months according to the clinical condition of the patient.
The mean number of follow-up visits for each patient was 3.6 ± 2.4; the interval between the first and the last follow-up visit was 215.4 ± 263.1 days. For the outcome results of this study, it is necessary to differentiate between short-term symptoms of adverse effects of CT or RT, which appear on the same day of treatment and persist for a few days, and long-term symptoms caused by anticancer treatments (e.g., lymphedema after surgery or radiation) or by the disease itself, persisting for at least 3 months, and by long-term therapies, such as hot flashes due to ET lasting at least 5 years: In the case of symptoms due to adverse effects from CT or RT that appear immediately or within a few days after the anticancer treatment (short-term symptoms), the patients' description of the intensity of the symptoms during the treatment, collected at the most recent follow-up visit after the last session of the round of the treatment, was used: 7.7 ± 6.1 days (8.1 days after CT and 7.5 days after RT). Some data were not derived from in-person visits but from telephone follow-up interviews generally with the patients who could not come for the checkup because of their poor health condition, but also during or immediately after the anticancer treatment to check the patient's conditions and possibly to update the integrative therapy. In case of long-term symptoms, namely symptoms due to anticancer therapy or to the cancer lasting for at least 3 months without benefit from conventional therapies or spontaneous resolution, or symptoms apparently not related to the cancer (comorbidities), the appointment for the follow-up visit is done after nearly 2 months, and, therefore, the mean time between the first visit and the first follow-up was 52 ± 36 days.
Long-term symptoms most frequently seen among patients at the clinic were anxiety, depression, lymphedema, irritable bowel syndrome, abscess, articular pain, fatigue, headache, insomnia, and mucositis.
Data collection
Data collected included patient demographic data, history, and oncologic diagnoses according to ICD 10 coding (International Statistical Classification of Diseases, Injuries, and Causes of Death 16 ); the conventional anticancer treatment and integrative therapy prescribed; and the dietary advice provided. The data were recorded on paper and inserted into the computerized clinical record WinCHIP (Computerized Homeopathic Investigation Program 17 ) and updated after each follow-up visit.
Each patient was assigned a numerical identification code for the anonymous treatment of data, and signed a privacy disclaimer and the informed consent form. At the first consultation, personal data (age and sex), the current state of health (cancer recurrence, metastasis, localization of cancer, type of cancer therapy, and possible reasons for not undergoing a therapy, including when refused by the patient), and the severity of each symptom were recorded in detail as well as the type of homeopathic and/or herbal treatment.
For patients seen for follow-up, the effect of the therapies in relation to the main complaints (the object of the request for intervention) was assessed. The main data on the patients' clinical situation and the results obtained were then summarized in an Excel database. These data were then processed by an external professional who was not a member of the clinical team that handled the visits and prescriptions for the cancer patients (blind analysis).
Outcome parameters
The intensity of each symptom before and after the integrative treatment is evaluated by the patient in conjunction with the doctor during the visits after a detailed analysis of his or her clinical condition related to the conventional anticancer therapy and then reported according to a simple grading system from G0 (absence of symptoms) to G1 (slight), G2 (moderate), and G3 (strong).
For each symptom, the most probable cause was hypothesized (cancer treatment, concomitant effect, and the cancer itself).
In the case of radiodermatitis, the number of RT sessions was also divided into four groups (“to be started,” “from 1 to 9,” “from 10 to 19,” and “from 20 to 29”).
The severity of radiodermatitis was evaluated according to the Radiation Therapy Oncology Group (RTOG) scale: G1 toxicity corresponding to light and/or painless erythema, epilation, desquamation, and/or dryness; G2 to sensitive and/or intense erythema, desquamation, partial sweating, and/or moderate edema; G3 to desquamation, widespread sweating, and/or marked edema; G4 to ulceration, hemorrhage, or necrosis. 18
Statistical analysis
Data entry, screening, encoding, and data analysis were performed at the Lucca Hospital Homeopathic Clinic. Statistical analyses were performed through the statistical software package PASW (release 18.1 of SPSS, Statistical Package for Social Sciences).
For each variable of the research, the frequency distribution in the sample was calculated. The outcome evaluation for the symptoms was conducted comparing G values at the first visit with G values at the follow-up visit, as previously described under the Study procedures section (Wilcoxon's test applied to matched-pair samples).
In evaluating the severity of radiodermatitis, the Mann–Whitney U test was applied to independent samples both associated with a two-tailed significance test.
Results
The most frequent tumors out of 357 cancer patients were those of the breast: 204 patients (57.1%) followed by cancers of colon (26 or 7.3%), lung (18 or 5%), and ovaries (14 or 3.9%). Hematologic cancers (leukemia, lymphoma, and myeloma) were rarer: (10 or 3.0%) (Table 1).
The prevalence of patients (women) with breast cancer is in part not only due to the widespread nature of the pathology but also due to referrals coming to us from the oncology department of Lucca, which is renowned for excellence in the treatment of breast cancer. However, cancer cases included in this study were not limited to those in the initial stages: 123 (34.5%) had reached a stage that involved the local/regional lymph nodes or had distant metastasis; 33 (9.2%) had a cancer recurrence (local and distant) and 9.5% of patients had a previous history of cancer. At least one follow-up visit was performed on 184 patients, 51.5% of the total.
Table 3 illustrates the main symptoms reported by the patients at the IO clinic of Lucca and the conventional anticancer treatments that may have caused them. Asthenia and nausea/vomiting were the main effects of CT. The main symptoms related to the cancer itself were depression, anxiety, and asthenia. As expected, hot flashes and joint pain were the symptoms most frequently connected with ET. Lymphedema was mainly related to surgery (particularly in breast cancer) and dermatitis to RT.
ET, endocrine therapy; RT, radiotherapy.
Table 4 shows an analysis of treatment results. Because this was conducted without access to an adequate control group, the intensity of symptoms was compared, measured from G0 to G3, as outlined in the Methods section, before and after the integrative treatment, and evaluated that is very soon after the end of the round of the anticancer treatment and sometimes also during the treatment to update the integrative therapy and then reported at the moment of the follow-up visit.
Significance at Wilcoxon test for paired samples.
Comparing clinical conditions before and after treatment, a significant amelioration was observed, obtained using the Wilcoxon test for paired samples: hot flashes (p ≤ 0.01), nausea (p ≤ 0.01), depression (p ≤ 0.001), anxiety (p ≤ 0.001), insomnia (p ≤ 0.001), fatigue (p ≤ 0.001), joint pain (p ≤ 0.05), mucositis (p ≤ 0.05), dysgeusia (p ≤ 0.05), neuropathy (p ≤ 0.05), and all symptoms (p < 0.001).
Radiodermatitis from RT deserves a separate discussion. In this case, generally the patient requires an integrative treatment before the start of RT or in its initial phases, inasmuch as radiodermatitis worsens in the final phases of RT series (generally 28 or 30 sessions). Therefore, the severity of radiodermatitis was assessed in a group of 30 consecutive patients undergoing RT, evaluated at the beginning and the end of the RT, according to the RTOG scale. 18 Seventeen patients undergoing an integrative RT protocol were compared with a control group of 13 patients without integrative therapy. Among those with integrative treatment, 15 had G1, 1 patient had G2, and 1 patient had G3 toxicity, whereas in the group without integrative treatment, only 5 patients had G1, 2 had G2, 3 had G3, and 3 had G4 (Mann–Whitney U test: two-tailed significance: p ≤ 0.01).
Finally, Table 5 shows preliminary data concerning 21 (6.2%) patients with curable cancer who either refused (18 patients) or decided to discontinue (3 patients) conventional anticancer treatment against the recommendation of their oncologist. All of these patients were women with a mean age of 56.3 years (39–79); five (23.8%) had a previous history of cancer, two (9.5%) had a cancer recurrence, and nine (42.8%) already had a metastasis. Five (23.8%) requested nonconventional treatment as an “alternative” to standard care, which was obviously not provided by the clinic. The other patients asked only for a “natural” treatment to control cancer symptoms (joint pain, hot flashes, anxiety, depression, digestive disturbances, panic attacks, etc.).
CT, chemotherapy.
Among those who refused or discontinued treatment, 17 (80.1%) had a follow-up, 9 (53%) passed away, 7 (41.2%) are currently in good health, and 1 (5.9%) is in a state of progressive decline. After their IO visit, 7 out of the 17 (41.2%) patients with follow-up accepted the standard oncologic treatment, 4 of these were in good condition, and 3 passed away possibly because the decision to undergo or resume standard treatment came at a disease stage that was too advanced.
Bias
This study reports on clinical activity carried out since 2013 and, therefore, it was not possible to compare results of CM treatment in cancer patients with the results from a control group. In the future, prospective randomized and controlled studies, if possible compared with placebo, must be carried out.
Another potential bias is that a very general nonspecific method of evaluation—one without specific systems of symptom evaluation—was used to calculate outcomes. More appropriate criteria were employed to evaluate the severity of radiodermatitis symptoms, 16 which were also compared with those of a group of nontreated patients that was not randomized.
Discussion
Reducing adverse reactions to anticancer therapies can be the common goal of both oncologists and CM practitioners. CMs can be used to decrease the adverse effects of anticancer therapy without causing additional or cumulative drug toxicity. In fact, no serious adverse reactions or drug interactions due to complementary therapies have been reported to date in the authors' clinical experience.
In this context medical doctors who are experts in CMs may play a relevant role, as they can explore whether cancer patients are using CMs, ask about their perceptions of its potential benefits, and provide information about possible unrecognized interactions between conventional medication and CM treatments. All these data, together with a patient's psychological distress evaluation, can be discussed with the oncologic staff during regular meetings, creating a positive experience and the basis for a truly integrative medicine.
At the Lucca hospital, the Clinic for Complementary Medicine and Diet in Oncology works side by side with the medical oncology department and psycho-oncologists. The majority of cancer patients are seeking advice on reducing the adverse effects of CT and RT and asking for CM treatments for hot flashes due to ET.
Approximately 6% of patients come to the clinic with the intention of refusing or interrupting conventional anticancer care despite their oncologist's recommendation and request an “alternative” treatment for their illness. Most of these patients are not under professional care with either a CM expert or an oncologist and gathered information through the Internet or word of mouth.
In Italy, this growing phenomenon of self-care and the rejection of conventional therapies are bound to be permanent rather than passing, 19 even though it has been established that the use of “alternative” therapies for curable cancers not associated with conventional anticancer treatments could increase the mortality rate. 20,21 This has been recently confirmed by Johnson et al. 22 who observed that cancer patients using CMs had higher refusal rates for surgery, CT, RT, and ET. Use of CM was associated with a poorer 5-year overall survival than patients not using CM, and it was independently associated with higher risk of death. 22
For these reasons, it would be desirable for the oncology departments to start defining policies to deal with this issue.
In the clinic, CM experts are able to promote a dialogue with these patients who are typically quite diffident toward classical oncology. In addition to introducing this role of a medical doctor who is authoritative and competent in CMs, they can convey the possible serious consequences of self-help solutions and nonprofessional, Internet-sourced, and word-of-mouth advice. In fact, ∼40% of these patients in this study accepted conventional treatments after having spoken with a CM physician. These data correspond more or less with reports in the literature. 23
Moreover, integrative therapy also seemed to play a positive role in preventing skin damage from RT, which is already documented in the literature. 10,24 In fact, a simple therapeutic protocol based on the oral and topical administration of homeopathic remedies and herbal ointment before and after exposure to RT seems to be capable of preventing the degree of skin damage in the majority of patients compared with a nontreated group.
It is necessary to confirm these observations through additional controlled randomized studies, which can make use of specific affordable methods of evaluation, at least for the more frequently observed symptoms. These preliminary results are nevertheless encouraging, particularly if it is considered that this approach is affordable, sustainable, and quite simple in its application.
Conclusions
The integration of evidence-based complementary treatments seems to provide an effective response to cancer patients' demand for a reduction of the adverse effects of anticancer treatments and the symptoms of cancer itself, thus improving patient's quality of life and combining safety and equity of access within public healthcare systems. It is, therefore, necessary for physicians (primarily oncologists) and other healthcare professionals in this field to be appropriately informed about the potential benefits of CMs.
Footnotes
Acknowledgments
The authors would like to thank Drs. Editta Baldini, Lucia Tanganelli, and Simona Giovannelli of the Lucca Oncology Department for their collaboration in the clinical activities, as well as Drs. Stefania Tocchini and Lucia Da Valle, psycho-oncologists, and Dr. Aroldo Marconi, surgeon at the Breast Unit of Lucca, for their support. All the costs for this study were supported by the public healthcare system of the Region of Tuscany.
Author Disclosure Statement
No competing financial interests exist.