
Abstract
Objectives:
Poor lifestyle choices play a significant role in the development and progression of preventable chronic diseases, including cancer. In this study, we evaluate the effectiveness of a comprehensive lifestyle medicine intervention on chronic disease risk factors and quality of life in breast cancer survivors.
Design:
This is a retrospective review of a clinical program from January 2016 to July 2017.
Settings/Location:
It includes seven 2-h group medical visits held every other week at an outpatient wellness facility.
Subjects:
Eligible participants are breast cancer survivors who have completed treatment, including those who remain on hormonal therapy.
Intervention:
Patients receive education and experience in nutrition, culinary medicine, physical activity, and stress relief practices.
Outcome measures:
Participants' weight, body mass index (BMI), body fat mass, lean body mass, and percent body fat were measured at visit 1 and visit 7. Standard validated questionnaires were used to measure perceived stress, depression, patient activation, physical and mental quality of life, dietary fat consumption, and dietary fruit, vegetable, and fiber consumption.
Results:
A total of 31 patients participated in the group visits. Pre–post comparison data were not available for 10 patients. More than three-quarters of the 21 breast cancer survivors who attended 5 or more of the 7 group visits and provided data at the first and the last group visit decreased their body weight. On average, patients lost 4.9 pounds (−2.6%, p < 0.01), and their BMI decreased by 0.8 kg/m2 (−2.5%, p < 0.01). Changes in psychosocial variables of perceived stress, depression, patient activation, and quality of life trended in a positive direction, but did not reach statistical significance. Patients reported a significant decrease in average weekly fat consumption (−31.5%, p < 0.01). Most patients found the program educational and enjoyable, and nearly half of them described it as life changing.
Conclusions:
Breast cancer survivors could employ the prescribed lifestyle modifications to produce clinically relevant health benefits. Interdisciplinary teams of health care professionals may help breast cancer survivors with chronic diseases implement evidence-based, individualized, and effective lifestyle prescription through group medical visits.
Introduction
Poor lifestyle choices are key in the development and progression of preventable chronic diseases, including cancers of the breast, colon, and prostate. 1 –5 Chronic conditions present at the time of cancer diagnosis, such as cardiovascular disease, obesity, and diabetes may also have substantial influence on survival. 6 –13 For example, obesity is associated with poor outcomes in women with breast cancer, especially for estrogen-receptor-positive breast cancer. 14 Furthermore, studies indicate that the leading cause of death among Medicare breast cancer survivors is cardiovascular disease, not breast cancer. 6,15,16
The importance of expanding cancer care to include the promotion of long-term health is emphasized by the Institute of Medicine's report on delivering quality oncology care 17 and is supported by both the American Cancer Society and the American Society of Clinical Oncology. 18 To achieve that goal, the development of partnerships between oncology providers, primary care providers, and experts in nutrition, exercise science, and behavior change has been strongly encouraged. 19 Unfortunately, programs to help positively orient cancer patients toward longer and healthier lives and assist them in applying healthy lifestyle behaviors in a sustainable way are rarely implemented in the current fee-for-service health care model.
In 2011, we reported that participation in a comprehensive therapeutic lifestyle intervention program, Lifestyle 180®, was beneficial to over 400 patients with multiple chronic diseases, including 58 cancer patients. 20 This intensive program consisting of 72 h of hands-on lifestyle intervention and education, distributed over 12 months, was not covered by insurance, and therefore patients paid entirely out of pocket to participate.
Over the past 2 years, we implemented a series of lifestyle medicine-focused shared medical appointments (SMAs) called “Living Well after Breast Cancer.” In accordance with current guidelines, these group visits address lifestyle modification in a comprehensive fashion and are reimbursed by the most third-party payers. They are designed to promote survivorship and improve quality of life in breast cancer patients posttreatment by helping them recognize and apply healthy self-care practices that have been shown to reduce the risk of breast cancer recurrence. These healthy self-care practices are also known to help reduce risk factors for cardiovascular disease and may additionally prevent the progression of other chronic conditions such as obesity, which are common in this population. 21 –25
In this study, we report preliminary outcomes for breast cancer survivors who, through participation in our “Living Well after Breast Cancer” clinical program, implemented beneficial lifestyle-related behavior changes as part of their usual posttreatment care.
Materials and Methods
Intervention
“Living Well after Breast Cancer” is a short, yet comprehensive lifestyle medicine intervention that includes both education and practical experience using group medical visits. It includes seven 2-h SMAs held every other week for a total duration of about 14 weeks. Under the guidance of a multidisciplinary lifestyle medicine team consisting of a physician, medical assistant, professional chef, yoga therapist, registered dietitian, and behavioral health specialist, patients engage in nutrition, culinary medicine, physical activity, and stress relief practices.
A physician and behavioral health coach are present for all visits, and each visit includes a physical exam and review of medications. In addition, each visit also includes a practitioner of a different therapeutic lifestyle modality. Visits 1 and 7 serve an introductory and wrap-up role, respectively. Visit 2 is facilitated by a dietitian who addresses patients' questions related to dietary choices for breast cancer survivors. Patients learn how to read nutrition labels; focus on eating more servings of unrefined, whole plant foods and less sugar, red and processed meats; and shop for healthy foods.
Visits 3 and 6 focus on culinary medicine, take place in a professional teaching kitchen, and are facilitated by our executive chef. Patients learn how to prepare delicious healthy meals with few ingredients through technique-driven demonstrations and education that focuses on how to achieve moisture without adding fat, sweetness without added sugars, flavor without added sodium, and savory density without meat. During each of these visits, patients observe the preparation of at least three healthy recipes and taste the demonstrated dishes.
Visit 4 includes discussions about the impact of unmanaged stress on health and focuses on providing patients with techniques to elicit the relaxation response. This visit, facilitated by the behavioral health coach, includes the practice of stress relief techniques, such as breathing exercises, guided imagery, meditation, as well as mindful sitting and eating. Physical activity is included in every visit, as patients are instructed on how to engage in walking and nonwalking aerobic exercises at their homes or workplaces. Strength exercises, modified to fit the fitness level and functional limitations of each individual, seated yoga poses, and breathing exercises, are demonstrated by a physician and practiced with patients during visits 2, 3, and 4.
Visit 5 is facilitated by our yoga therapist and includes the practice of yoga poses and breathing exercises, both seated and standing, to counteract chronic stress. At the end of each visit, patients are given a set of self-care practices reflecting the content and goals of the session and encouraged to integrate them into their daily lives for the next 2 weeks. The frequency, intensity, and duration of these lifestyle modifications progresses gradually over the course of the visits and is adjusted on an individual basis as part of a well-established path to help transition patients from the clinic to optimal self-care at home.
Population
All breast cancer survivors who have completed treatment, including those on hormonal therapy, are eligible to participate in these SMAs and are recruited primarily through the clinical practice of the authors listed. Before the first group visit, patients had a 1-h-long Lifestyle Medicine consultation at the Wellness Institute, during which the nature of SMAs was explained and questions answered. All patients were treated surgically and had other types of therapies as shown in Table 1.
Demographics for Breast Cancer Survivors Participating in Living Well After Breast Cancer Shared Medical Appointment
Individual Fisher tests for each comorbidity did not find statistically significant differences between groups (prediabetes was close; p = 0.07).
Wilcoxon testing for the total number of comorbidities did not find a statistically significant group difference.
BMI, body mass index.
Outcomes
To assess the effectiveness of Living Well after Breast Cancer, we summarized the biometric and psychosocial data collected during the first and last SMA visits (visit 1 and visit 7). As part of the clinical program, participants' weight, body mass index (BMI), body fat mass, lean body mass, and percent body fat were measured through the InBody720, a high-precision instrument that uses bioelectric impedance analysis to evaluate body composition. Psychosocial metrics included perceived stress, depression, patient activation, and physical and mental quality of life. In addition, participants reported dietary fat consumption and dietary fruit, vegetable, and fiber consumption. All patient-reported outcomes were measured using standard validated questionnaires.
The 4-item Perceived Stress Scale (PSS-4) measures a person's perception of and response to daily hassles and stress, resulting in a total score of 0 (best) to 16 (worst). 26 The 10-item Center for Epidemiological Studies-Depression survey (CES-D 10) asks respondents to rate how often over the past week they experienced symptoms associated with depression, such as sleep difficulties and feeling lonely. Scores range from 0 to 30 with higher scores indicating more symptomatology. 27 The Patient Activation Measure (PAM) assesses one's ability and willingness to manage his or her health. Scores range from 0 to 100 with higher scores indicating greater activation. 28
Quality of life was measured using a 10-item global health assessment tool called the Patient-Reported Outcomes Measurement Information System (PROMIS-10) questionnaire. Scores on this survey range from 0 to 100, with higher scores indicative of greater physical and mental quality of life. 29 The Block Dietary Fat Screener and Block Dietary Fruit, Vegetable, Fiber, and Screener were used to measure weekly intake of fat and weekly intake of fruits, vegetables, and fiber. Scores range from 0 to 68 and from 0 to 50, respectively, with higher scores reflecting increased consumption. 30
In addition to these metrics, participants were also given an end-of-program survey in which they were asked to describe the Living Well after Breast Cancer SMAs using a physician-generated list of responses, including life-changing, educational, exciting, enjoyable, boring, and a waste of time. Participants were asked to mark all responses that apply.
Statistical analyses
Only participants who had data from both visit 1 and visit 7 were included in the statistical analysis. All data were analyzed using paired two-sample t-tests. Continuous variables were presented as mean ± standard deviation and categorical variables as n (%). Analyses were performed in R version 3.3.2 and GraphPad Prism 5 software.
Results
Four cohorts totaling 31 breast cancer survivors had participated in our Living Well after Breast Cancer SMAs. Of those, 21 SMA patients were included in this analysis. They attended at least five of the seven SMA visits and fully completed the surveys. For 10 patients we did not have pre–post data. Although three of them attended five or six group visits, they did not attend the last group visit. The remaining seven patients had poor attendance, one for medical, two for personal, and four for unknown reasons.
Table 1 summarizes the cohort demographics for both groups at baseline, showing an average age of 56 years for both. In addition to the diagnosis of breast cancer, other comorbidities in our population included prediabetes, type II diabetes, hypertension, hyperlipidemia, overweight, obesity, depression, and chronic pain. Most breast cancer patients suffered from a high burden of chronic disease, with nearly 76% having two, three, or four of the aforementioned comorbid diagnoses. There were no significant differences in breast cancer stages, previous treatments, and their burden of comorbid conditions between the group of 21 patients with evaluable data and those without such data (the group of 10 patients).
The majority of patients trended in the direction of positive health across outcomes. The magnitude of these changes is summarized in Table 2 (biometric variables) and Table 3 (participant-reported variables).
Biometric Outcomes for Breast Cancer Survivors Participating in Living Well After Breast Cancer Shared Medical Appointment
SD, standard deviation.
Patient-Reported Outcomes for Breast Cancer Survivors Participating in Living Well After Breast Cancer Shared Medical Appointment
SD, standard deviation.
At 14 weeks, breast cancer survivors significantly improved their weight and BMI. Patients lost an average of 4.9 pounds (−2.6%, p < 0.01, Table 2, individual data in Fig. 1), and their BMI decreased by an average of 0.8 kg/m2 (−2.5%, p < 0.01). Although both, body fat mass and lean body mass, decreased by an average of 2.6 pounds (−3.2%, p < 0.05) and 2.3 pounds (−2.1%, p < 0.01), respectively, no statistically significant changes were shown for the percent body fat. We were unable to detect differences in the psychosocial variables of perceived stress, depression, patient activation, and quality of life. Patients reported a significant decrease in average weekly fat consumption score (−31.5%, p < 0.01, Table 3, individual data in Fig. 2) and no detectable difference in average weekly fruit, vegetable, and fiber consumption (+3.3%, p = 0.62).
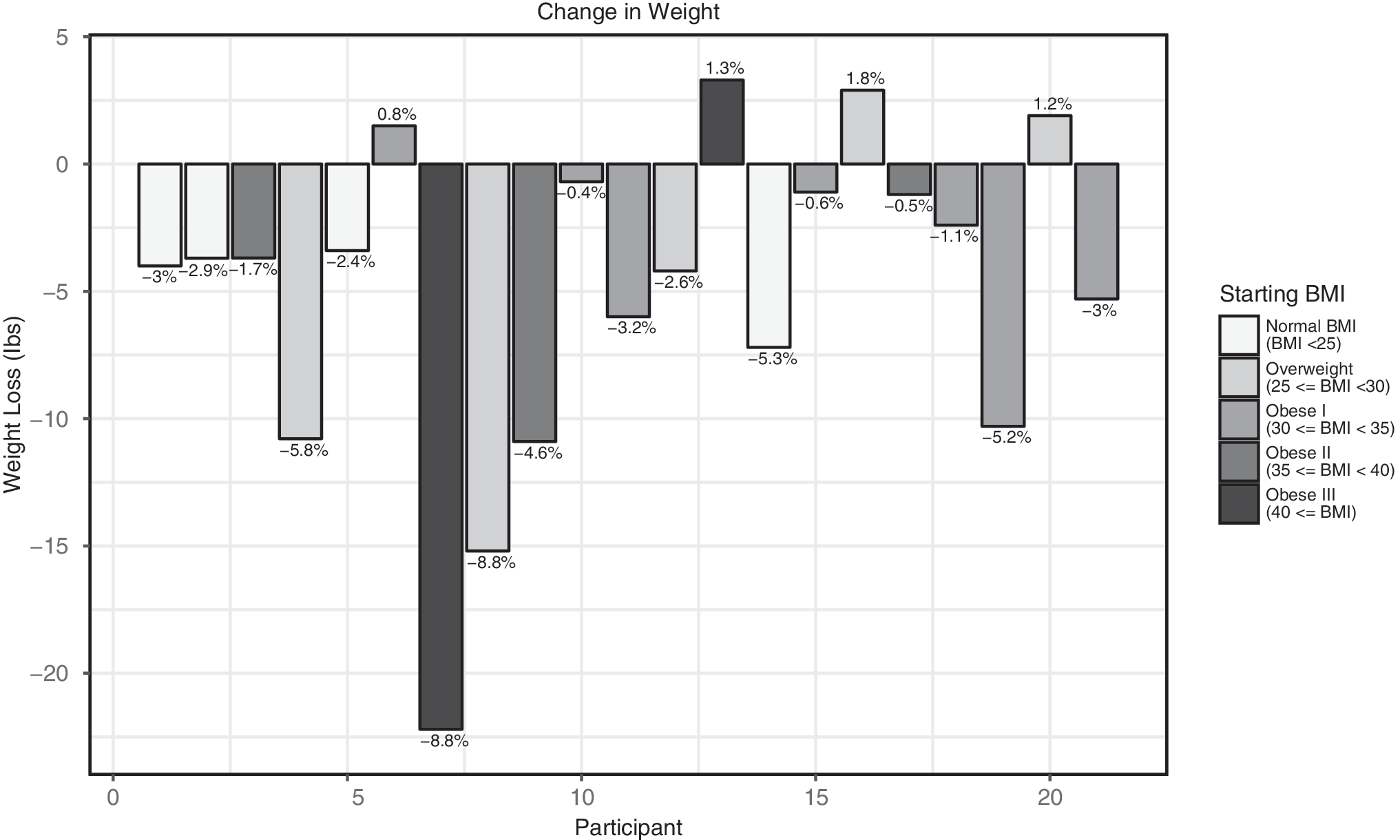
Individual changes in weight for breast cancer survivors participating in Living Well after Breast Cancer SMA. BMI, body mass index; SMA, shared medical appointment.
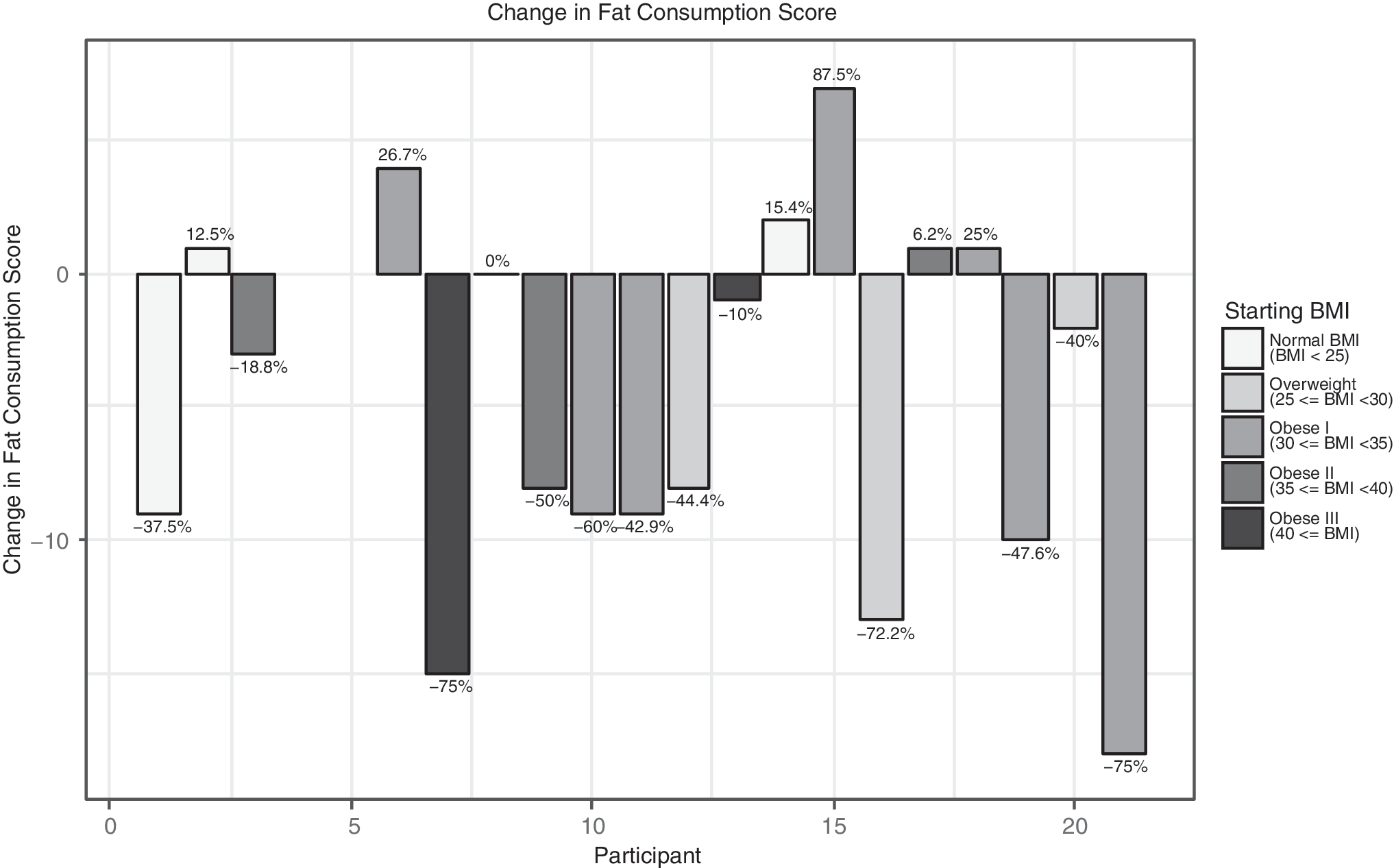
Individual changes in weekly dietary fat consumption for breast cancer survivors participating in Living Well after Breast Cancer SMA. BMI, body mass index; SMA, shared medical appointment.
End-of-program surveys indicated that the majority of respondents described the Living Well after Breast Cancer SMAs in a positive way. Only one individual believed that the intervention was boring, and no one found it to be a waste of time. Seventy-three percent of respondents found the clinical program educational and 74% found it enjoyable. Over one-third of respondents (36%) reported the program was exciting, and nearly half of all respondents described the Living Well after Breast Cancer SMAs as life changing (46%).
Discussion
Studies of cancer survivors suggest that individuals who are diagnosed with cancer have good intentions to make changes in behaviors they believe put them at increased risk for disease progression and are motivated to engage in practices they view as protective against future cancer-related issues. There are, however, several barriers to implementing healthy lifestyle changes. Self-efficacy may be low and knowledge may be lacking, as survivors are challenged to find the resources, support, or reinforcement required to achieve and sustain healthy lifestyles because they are not disseminated as standard of care. 31,32 The prevalence of conversations focused on lifestyle modifications with oncologists is low because of time constraints, inadequate reimbursement by insurers, perception that patients are not interested in such conversations, and even which provider should be responsible for such discussions. 33,34
It is, therefore, not surprising that during the past decade, the percentage of cancer survivors who engage in a combination of healthy lifestyle practices as per the guidelines remains below 10%. 35,36 This poses a significant threat to public health, as advances in early detection and treatment as well as a growing and aging population are contributing to a rapidly increasing number of cancer survivors, especially those with breast cancer. With a current 5-year survival rate at nearly 90% for all stages combined, breast cancer survivors are the most prevalent cancer survivor group, 37 and therefore research into effective approaches that promote the sustainable integration of therapeutic lifestyle-related behavior changes into the standard posttreatment care of breast cancer survivors is sorely needed.
In this study, we report preliminary findings that a multidisciplinary lifestyle medicine intervention through group medical visits is feasible and clinically beneficial to breast cancer survivors posttreatment. We suggest that group visits that are focused on addressing questions of survivors' lifestyle choices in a comprehensive and integrative fashion by a team of lifestyle medicine professionals may represent one way to overcome the existing gap between what is needed and what is currently being done.
Running a lifestyle medicine-focused clinical program as a series of group medical visits is economically feasible, as the payments by participants' medical insurance were sufficient to cover program costs. Depending on their insurance, some patients were responsible for a copay, and every patient paid $55 to cover the cost of a binder containing 40+ recipes, a meditation CD, a book, and copies of materials, flyers, and pertinent studies that were shared with patients during the visits.
SMA visits were well attended, and participants reported adherence to their individually prescribed health behaviors while at home. More than 80% (17 of 21) of breast cancer survivors who attended 5 or more of the 7 group visits lost weight during the program. On average this cohort lost a significant amount of weight, which is clinically relevant because weight gain is associated with poor prognosis, 14,23,24 and many breast cancer patients gain weight both during and in the years following treatment. 25,38,39
In addition, our weight loss results occurred in a relatively short timeframe (14 weeks), as the vast majority of weight loss-specific trials in breast cancer patients have reported losses of up to 5% of initial body weight within a 1-year time frame. The 2.6% average decrease in body weight reported in this study is approaching the American Heart Association's 3% threshold associated with a clinically meaningful reduction in cardiovascular risk factors also over a 1-year time period. 40
Although more than half of patients decreased their percent body fat, three quarters of them also experienced undesired loss of lean body mass. It is likely that this may be associated with the limitations patients had postsurgery in performing strength exercises for the upper body and trunk. In addition, the emphasis during the SMAs was on increasing walking and interrupting long periods of sitting as well as practicing gentle yoga poses rather than engaging in more formal resistance training. This fact coupled with the decreased intake of high-calorie dense foods is most likely responsible for the decrease in lean body mass.
When people consume fewer calories without increasing physical activity, especially resistance training, they lose both body fat mass and lean body mass. One weight loss study of obese subjects showed that after 6 months, participants lost 5.7 pounds body fat mass and 6.2 pounds lean body mass, almost a 1:1 ratio. 41 Our study, although of shorter duration, found a similar ratio, with women losing 2.6 pounds body fat mass and 2.3 pounds lean body mass.
Looking at our patient-reported outcomes at visit 1, it is evident that our population began the Living Well after Breast Cancer program with low levels of perceived stress (score of 4.4) when compared with the general population (scores ranging from 4.7 to 6.1) 42,43 leaving little room for further reduction. The CES-D 10 depression score of our patients decreased from 6.2 to 5.1, to the value reported for the general population, 44 but it did not reach statistical significance.
Visit 1 levels of patient activation were relatively high, revealing that participants already felt they had the key facts and were more focused on building self-management skills. Even still, 3 of the 19 patients reported an increase from this level of activation to the highest health engagement level and the whole group increased the score by 3.9 points (p < 0.10) indicating that they tend to have adopted new behaviors and are focused on healthy lifestyle maintenance. 6,45,46 Physical and Mental Health scores were reflective of the average scores for the general population and did not change significantly from visit 1 to visit 7.
In addition to the validated Block food consumption surveys completed by patients at visits 1 and 7, patients also reported the types of dishes they prepared at home during each SMA visit. While those dishes included more vegetables and legumes, this was not reflected in the weekly dietary fruit, vegetable, and fiber consumption surveys at visit 7. We suspect that the visit 1 fruit, vegetable, and fiber intake scores were inflated because of the well-known, noncontroversial and socially desirable health benefits of these foods. In the future, we need to increase the completeness of the culinary medicine data collected during the SMA visits as a way to better evaluate patients' food choices.
Other limitations include a lack of evaluation of the changes in patient fitness using a validated questionnaire. Patients were provided with a daily diary sheet at every visit to record their self-care practices at home during the 2 weeks in between SMAs. Patients recorded their minutes of walking and often the number of steps taken if they owned a pedometer, but the possible associations with increased physical activity and weight loss was not performed for this report.
The patients who routinely completed the daily diaries believed them to be a key motivating factor in implementing lifestyle changes because it gave them more accountability. Previous work such as that of Dr. Dean Ornish's group showed that patients who engaged more into their self-care had a greater degree of coronary artery disease reversal than those who engaged less enthusiastically. 47 In the future, we plan to better capture self-reported data on our patients' physical activity to evaluate the dose–response of exercise and other lifestyle self-care practices to health outcomes.
It is important to note that our SMAs are not a clinical trial with prescribed diet and physical activity, but rather clinical practice in which we meet patients where they are and work with them to improve their food choices and physical activity levels. For example, the dietary targets for the Women's Health Initiative Dietary Modification Trial (WHI) 48 included reducing energy from fat to 20%, increasing the intake of fruits and vegetables to at least five servings per day, and increasing the intake of grains to at least six servings per day. Our approach is broader, advising participants to eat more whole, unrefined, unprocessed foods of plant origin than what they are currently consuming.
This is also different than the stricter dietary prescription seen in Dr. Dean Ornish's program, a whole foods plant-based diet with no added oils. While we would be pleased if our patients chose such a diet and we encouraged them to strive to achieve that goal, we allowed them some flexibility based on their job, family situations, food preferences, and other circumstances. In general we advised patients to limit, and ideally eliminate the consumption of red and processed meats, all sugars, and refined grain products. Most of the recipes provided and demonstrated during the culinary medicine visits were plant-based, and we taught our patients how to prepare such meals without adding oils or sugars. By the end of the group visits, most patients ate a predominantly plant-based diet with fish, poultry, or dairy being the only foods of animal origin.
For all outcomes reviewed in this analysis, a larger sample size and longer follow-up are necessary to determine if essential self-care practices are sustainable. Many of the patients who participated in the Living Well after Breast Cancer SMAs attend routine follow-up appointments in 3-month intervals at the Lifestyle Medicine clinic. Including data from these appointments may help us determine whether participants have deeply embedded healthy lifestyle practices into their daily lives.
Conclusions
Preliminary results of the Living Well after Breast Cancer SMAs indicate that breast cancer survivors could incorporate the prescribed lifestyle modifications into their lives to a degree that produced clinically relevant health and quality-of-life benefits. Because of the small number of patients, several outcomes trended in a positive direction, but did not reach statistical significance. Our SMA model, with its emphasis on facilitating self-care, is expected to provide much-needed longitudinal support leading to successful healthy lifestyle behavior change. In the current transition to value-based health care, this type of intervention may represent an optimal way for an interdisciplinary team of health care professionals to help patients with chronic diseases implement evidence-based, individualized, and effective lifestyle prescription.
Footnotes
Acknowledgments
This study was internally funded by the Cleveland Clinic. All work was performed at the Cleveland Clinic. The authors are grateful to all of the personnel involved in the Living Well after Breast Cancer SMAs, including Robin Houston (scheduling), Danielle Riedel (SMA coordinator), the patient service representatives and medical assistants, as well as those listed below. Nutrition: Kristin Kirkpatrick, MS, RDN; Beth Bluestone, RD; Culinary Medicine: Jim Perko, CEC, AAC; Behavioral Health: Jane Ehrman, MEd, CHES, CHT; Yoga: Judi Bar, CYT, E-RYT 500.
Author Disclosure Statement
No competing financial interests exist.