
Abstract
Objectives:
The objectives of this study were to define dietary supplement (DS) use by cancer patients and to investigate factors associated with DS use during cancer treatment.
Methods:
A cross-sectional survey of adults diagnosed with breast, colorectal, lung, or prostate cancer in 2010–2012 at the University of North Carolina Comprehensive Cancer Center was conducted. Questionnaires were sent to 1794 patients. Phone calls were made to nonrespondents. The authors described type of DS use before, during, and after initial cancer treatment, source of advice on DS use, and used logistic regression to investigate the association of DS use during or after cancer treatment with clinical/sociodemographic characteristics and source of advice.
Results:
Six hundred and three (34%) patients completed the questionnaires. Nonvitamin nonmineral DS use during initial cancer treatments was common: any cancer treatment (49%), chemotherapy (52%), and radiation therapy (51%). Among patients seeking advice on DS use, 75% reported professional sources, 44% reported media sources, and 47% reported lay sources. DS use during cancer treatment was strongly predicted by prior DS use, followed by prior complementary therapies' use, receiving DS advice from a cancer care provider, being female, and higher education level.
Conclusion:
DS use is common and persists during cancer treatment. Among DS users during treatment, 18% used an herbal supplement, which are likely to carry greater risk of interaction with chemotherapy agents compared with vitamin, mineral, and other supplements. Although many respondents sought DS advice from professional sources, the use of nonprofessional sources remains high.
Introduction
D
Knowledge of cancer patients' DS use is important because of potential interactions between supplements and routine cancer treatments. 8 –18 However, cancer care providers often have little information of patients' DS use during their cancer treatments because: first, survey estimates of commonly used supplements among cancer patients during treatment are limited since most previous studies do not specify the time period of DS use in relation to cancer treatments 4,19,20 ; second, the communication on DS use between patients and providers is limited. 21,22
In addition, cancer care providers often have little training about the supplements themselves, and patients often seek or receive information on DS from both professional sources (e.g., primary and cancer care providers) and nonprofessional sources (e.g., mass media, family, friends). The role of information sources on patients' DS use during or after cancer treatment is not well understood. 3,20,23
Therefore, using a questionnaire-based survey, the authors sought to quantify DS use among adult cancer patients before, during, and after treatment, including vitamin, mineral, and nonvitamin nonmineral (NVNM) DSs. The associations between clinical/sociodemographic factors and DS use during cancer treatment, as well as between source of DS advice and use during cancer treatment were investigated.
Materials and Methods
Study population
A cross-sectional survey of adult cancer patients seeking care at the University of North Carolina (UNC) Lineberger Comprehensive Cancer Center (LCCC) between 2010 and 2012 was conducted. The authors have previously reported the survey results for general complementary and alternative medicine (CAM) use; this report will focus on DS use. 24 Briefly, eligible participants were English-speaking, 21 years or older, diagnosed with breast, colorectal, lung, or prostate cancer, and treated at the UNC LCCC. Complete details of the survey methods are previously described. 24 The UNC Institutional Review Board approved the research protocol, and all study participants gave informed consent.
Data collection
An introductory letter, questionnaire, and return postage envelope were mailed to 1794 patients. Respondents were asked about their use of DSs in the following four categories: vitamin, mineral, herbal, and other nonherbal NVNM supplements. For each category, respondents were asked to identify their DS use in three discreet periods: before cancer diagnosis, during primary cancer treatment (i.e., initial medical, radiation, and/or surgical treatment), and after primary treatment. In addition, participants were asked to report, by category, the specific supplements they used during their cancer treatment. To aid their recollection, commonly used DSs were listed, and if participants did not find their supplements listed, they were asked to record them in free text. Information on sources of advice, supplement use, and discussion of supplement use with oncology providers was also gathered. A tumor registry kept on all patients treated at the UNC LCCC provided demographic and clinical data, such as diagnosis date, tumor type and stage, and treatment history.
Statistical analysis
Descriptive data (frequency, percent) for age, sex, cancer type and stage, and prevalence of supplement use before, during, and after initial cancer treatment were provided. Logistic regression was used to investigate associations between (1) DS use during cancer treatment, (2) NVNM DS use during cancer treatment, (3) DS use during or after cancer treatment, and variables such as clinical, sociodemographic characteristics, prior CAM uses, and receiving advice on DS from the following sources: CAM provider, conventional provider, and oncology provider.
Results
Demographics
Six hundred and three (33.6%) participants completed the questionnaires. Ninety-eight percent of respondents were non-Latino, 79% were white, and 62% were female (Table 1). Compared with nonrespondents, respondents were more likely to be female, white, at early cancer stage, and have breast cancer, but less likely to have lung or colorectal cancer. 24
Use of DSs
Before cancer treatment, 399 (66%) of all 603 respondents reported using vitamin supplements, 198 (33%) reported using mineral supplements, 101 (17%) reported using herbal supplements, and 163 (27%) reported using other supplements. Four hundred and twenty-eight (71%) respondents reported using at least one DS before cancer treatment, 354 (59%) reported using at least one DS during cancer treatment, and 416 (69%) reported using at least one DS after cancer treatment (Fig. 1). Two hundred and thirteen (35%) respondents received chemotherapy, and 128 (60%) respondents who received chemotherapy reported using at least one DS during treatment. Two hundred and seventy (45%) respondents underwent radiation treatment, and 166 (61%) respondents who received radiation reported using at least one DS during radiation (Table 2). Three hundred and twenty-five (54%) participants reported using vitamin supplements during cancer treatment, where the most common vitamin supplements were multivitamin (313, 52%), vitamin D (88, 15%), vitamin B12 (39, 6%), vitamin C (34, 6%), and folic acid (18, 3%). A total of 171 (28%) reported using mineral supplements during cancer treatment, where the most common mineral supplement was calcium (208, 34%). Although vitamin and mineral supplement use was most commonly reported (56% during initial treatment), the NVNM supplement use (e.g., herbals, omega-3 fatty acids, probiotic, glucosamine) was also commonly reported (25% during treatment). Among participants reporting DS use during treatment (n = 354), 64 (18%) specifically reported using an herbal supplement during cancer treatment.
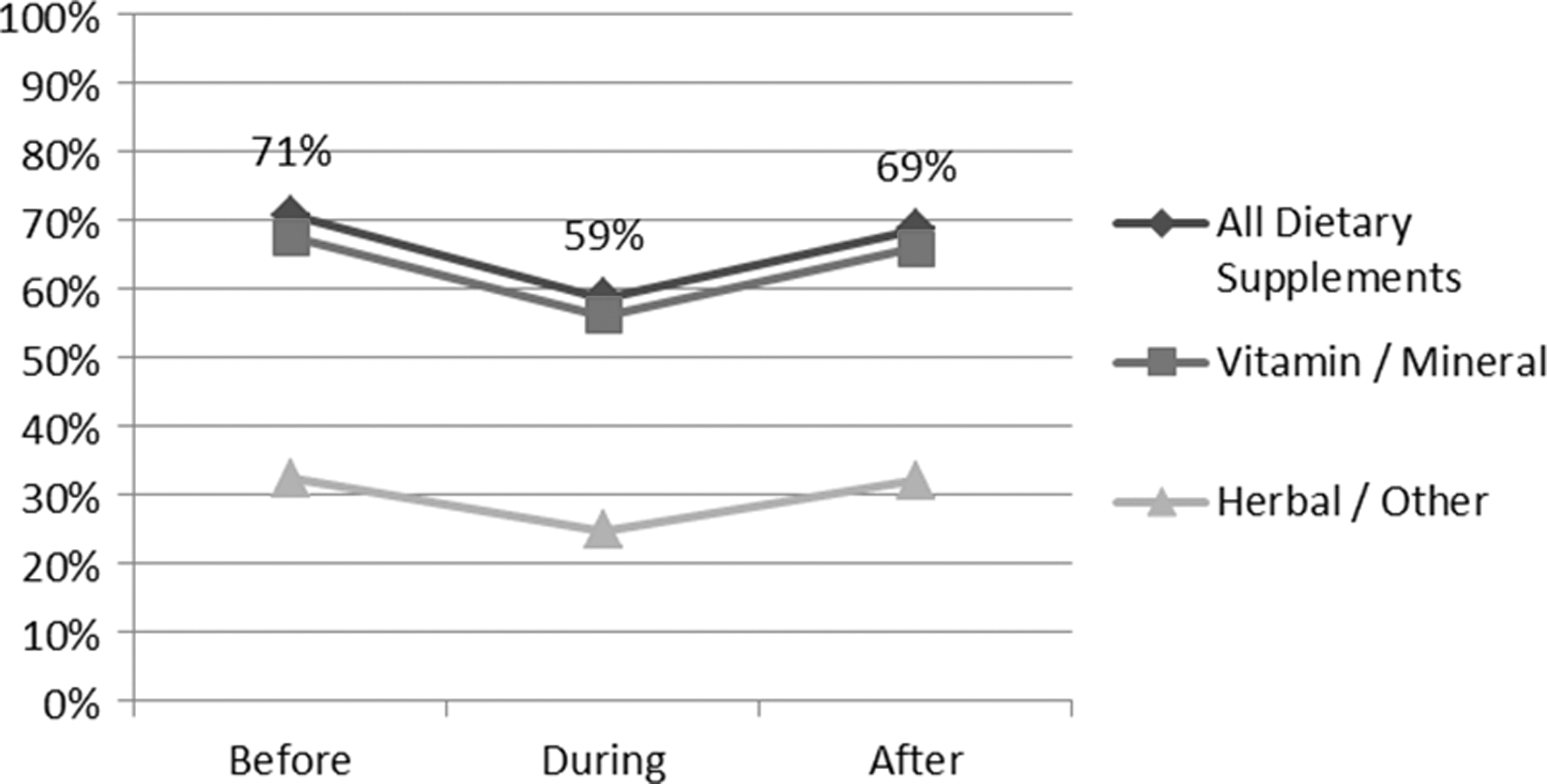
Proportion of respondents (N = 603) reporting dietary supplement use before cancer diagnosis, during treatment, and after cessation of primary treatment. Black line represents any supplement use; dark gray line represents any vitamin or mineral supplement use; light gray line represents any nonvitamin nonmineral supplement use. Treatment periods were defined as before diagnosis (before); during primary oncology treatment including initial surgery, chemotherapy, and/or radiation treatments (during); and after cessation of any initial oncology treatment (after).
Many patients reported using more than one category of DS.
Number of respondents reported using at least one category of DS (vitamin, mineral, and NVNM) during cancer treatment.
Total respondents undergoing any treatment (N = 603), chemotherapy (N = 213), and radiation (N = 270).
DS, dietary supplement; NVNM, nonvitamin nonmineral.
The most frequently reported NVNM supplements used during any initial cancer treatment, chemotherapy, or radiation were omega-3 fatty acids and green tea (Table 3), which were also the most frequently used supplements as monotherapy. Among respondents who reported NVNM DS use during treatment, most respondents (191/298, 64%) reported using more than one herbal or other supplements (range 1–30) during treatment, but few respondents reported using more than five supplements simultaneously (11%). Common combinations included omega-3 fatty acids with green tea, CoQ10, probiotic, antioxidant formulation, or glucosamine.
Many patients reported using more than one supplement.
Counts for the following were reported <5 times: Acai juice, Arnica gel, Astragalus, Biotin, Cat's claw, Chlorophyll, Dandelion root, DIM, Dragon's blood, Ginger, Glutamine, Hawthorn, Lecithin, Parsley, Peppermint oil, Pomegranate, Protein supplement, Quercetin, St. John's wort, and Tart cherry.
Total respondents undergoing any treatment (N = 603), chemotherapy (N = 213), and radiation (N = 270).
DS, dietary supplement; NVNM, nonvitamin nonmineral.
Sources of advice on DS use
When seeking advice on DS use, respondents most often cited professional sources (75%), such as their primary care provider or oncologist. However, media (44%) and lay sources (47%), such as friends, family, or support groups, were also commonly mentioned. Among professional sources, primary care providers (51%) were more frequently consulted than oncologists (35%), while CAM providers (10%), pharmacists (8%), other conventional providers (3%), and nutritionists (2%) were uncommonly consulted.
Use of DSs during cancer treatment and related factors
Seventy-six percent (325/427) of respondents who used supplements before cancer treatment continued to take a DS during treatment. Bivariate analyses show that while prior use of a variety of CAM therapies (e.g., mind–body therapies, body-based therapies) was associated with DS use during treatment, prior use of DSs specifically was most strongly associated with supplement use during treatment (odds ratio [OR] 16.2, 95% confidence interval [CI]: 10.2–25.5) (Table 4).
Includes vitamin, mineral, herbal, and other supplements together.
Includes herbal and other supplements only (no vitamin or mineral supplements).
DS, dietary supplement; CI, confidence interval; NVNM, nonvitamin nonmineral; OR, odds ratio.
Compared with respondents with breast cancer, those with lung (OR 0.56, 95% CI: 0.33–0.96) or prostate (OR 0.66, 95% CI: 0.44–0.97) cancer were less likely to use a supplement during treatment (Table 4). Supplement use did not appear to be associated with cancer stage. Notably, after adjusting for education, cancer type, and cancer stage, receiving advice on DS use from a CAM provider was associated with supplement use during treatment (adjusted OR [AOR] 3.6, 95% CI: 1.1–12.3) compared with advice from any conventional provider type (AOR 1.6, 95% CI: 0.97–2.48) or specifically an oncology provider (AOR 1.6, 95% CI: 0.87–2.80).
Discussion
This study described the DS use among cancer patients and investigated the factors associated with DS use during and after initial cancer treatment. Data were collected on DS use before, during, and after initial cancer treatment, sources of advice, and sociodemographic characteristics using a cancer patient sample at the UNC Cancer Hospital (LCCC). These data allows us to examine DS use during cancer treatment, the time period that is most critical for potential supplement–drug interaction.
DS use was found to be common throughout all time periods in this study population. Vitamin and mineral supplements were most commonly reported, but NVNM DS use was also common. This is consistent with findings from previous studies. 3 –7 For example, a survey conducted in Connecticut in a similar setting found 69% DS use after cancer diagnosis. 3 A systematic review on vitamin and mineral use among U.S. adults after cancer diagnosis found that 64%–81% of cancer survivors reported using any vitamin or mineral supplements and 26%–77% reported using any multivitamins. 7
During initial cancer treatment, more than half of patients reported use of vitamin and mineral supplements. This common vitamin and mineral supplement use needs to be noted because certain vitamin and mineral intake may interact with cancer therapy or carry potential benefits or harms for cancer survivorship. 25 For example, a randomized trial of antioxidant vitamins to prevent second primary cancers in patients with head and neck cancer, conducted in France, found that α-tocopherol supplementation produced unexpected adverse effects on the occurrence of second primary cancers and on cancer-free survival. 26 A review of vitamin and mineral supplement use in relation to cancer progression or mortality reported that vitamin D at higher than standard doses may improve cancer-specific and overall survival for several cancer types and that excessive folic acid in patients with established cancer may be harmful. 25 In light of the high prevalence of vitamin and mineral supplement use in cancer patients throughout all stages of treatment, providers should be knowledgeable concerning the general risks of benefit and harms for these supplements.
In contrast, only 12% (62/503) of “ever” DS users reported taking an herbal supplement during initial cancer treatment; 7% (14/213) of all patients who underwent chemotherapy used herbal supplements during chemotherapy; 9% (25/270) of all patients who had radiation therapy used herbal supplements during radiation therapy. Findings of this study for herbal supplement use are lower than previously reported (e.g., 21% prevalence of herbal preparation among cancer survivors in a similar setting, 44% of herbal supplements during chemotherapy in breast cancer patients). 6,27 The estimates may be lower for a couple of reasons. First, this study population was different. Hann et al.'s 27 study was conducted among 166 breast cancer survivors; all were female and 83% were white. Miller et al.'s 6 study population was also predominantly female and white (94%). Both being white and female and having breast cancer have been associated with DS use, which may explain the higher prevalence in those studies. 3,6,28 Second, the questions were asked differently. In the questionnaire of this study, the respondents were questioned about DS use before, during, and after cancer treatment, for which the responses were either yes or no, and then, a list of supplements was provided, and respondents were asked to report their DS use during cancer treatment. Hann et al., in comparison, asked open-ended questions and then recoded their answers. 27 In short, specific herbal supplement use may vary considerably based on cancer type.
Herbal supplements, however, are likely to carry greater risk of pharmacokinetic (PK) interaction with chemotherapy agents compared with vitamin, mineral, and other supplements, which less commonly cause PK interactions. 8,11,13 –17,29 –31 For example, green tea, the most common herbal DS found in this study, is a P-gp inhibitor, as well as an inhibitor of the transporters OATP1A1 and 1A2, with evidence for interaction with treatment agents such as imatinib (Gleevac). 32 Such interactions can result in either decreased chemotherapy exposure, potentially resulting in decreased treatment efficacy or increased chemotherapy levels, which can cause excess adverse events. Importantly, PK interactions can sometimes be mediated by altering medication dosages. 32 Therefore, the approach to counseling patients about concurrent supplement–drug use may differ depending on the specific supplement–drug combination or type of interaction. Furthermore, many potential PK interactions have not been borne out in clinical trials; therefore, an evidence-informed discussion concerning important supplement–drug interactions should focus on interaction risks, the extent to which those risks are known, and patient values such as their risk tolerance and acceptance of the range of potential treatment outcomes.
Although many respondents sought advice from professional sources (75%), the use of nonprofessional sources (media: 44%, lay sources: 47%) remains high. Attitude toward DS, perception of its risks, and pattern of communication of DS can vary greatly between conventional healthcare providers and complementary care providers. 33 –37 With that in mind, in this study, providers were encouraged to discuss DS use with their patients in an open and nonjudgmental manner to facilitate patient-centered communication and participatory patient decision-making. 38 When providers lack sufficient knowledge of specific DSs, referral to a pharmacist or clinical pharmacologist may facilitate evidence-based decision-making. Patients were also encouraged to discuss their DS use openly with their providers and seek advice on DS from professional sources rather than from nonprofessional sources to make an informed decision. 33,39
Although few participants reported visits to a CAM provider (10%), discussion of DS use with a CAM provider was associated with DS use during treatment, whereas discussion with other provider types was not associated with use during treatment. It is possible that patients who choose to speak to providers about supplement use may already be motivated to use supplements, and patients interested to speak to CAM providers were even more interested in using supplements, which may explain the larger association between CAM providers and DS use. It could also be that CAM providers may be more likely to recommend DS use during treatment, whereas other providers may make no recommendation or recommend against DS use. It should be noted, however, that the authors did not ask patients to describe the content of those discussions. Also, there was no information on whether patients chose to use a supplement before the discussion or only after discussion with their providers.
Limitations
The response rate was modest (33.6%) and may not fully represent all cancer patients who use DSs. However, the distribution of clinical characteristics of respondents, such as cancer type, cancer stage, age, and sex, only slightly differ from those of nonrespondents. 24 Furthermore, the estimated DS use rate during and after cancer treatment is largely consistent with previous findings on DS use since cancer diagnosis.
This study only surveyed patients with breast, colorectal, lung, or prostate cancer, and supplement use among patients with other cancer types may be different. Importantly, the specific supplements used by patients with different cancer types may vary widely, which may carry vastly different risks for supplement–drug interactions.
Conclusion
The use of DS before cancer treatment was common in this study population and persisted during cancer treatment. Among DS users during active cancer treatment, 18% used an herbal supplement, which are likely to carry greater risk of interaction with chemotherapy agents compared with vitamin, mineral, and other supplements. Although many respondents sought DS advice from professional sources, the use of nonprofessional sources remains high.
Footnotes
Acknowledgments
The authors thank Dionne Apple, Neha Verma, and Gavriella Hecht for their help in administering the survey and the UNC Odum Institute for their contribution to the creation and testing of the questionnaire. Funding for this research was provided by the North Carolina University Cancer Research Fund and the UNC Department of Family Medicine Small Grants Fund.
Author Disclosure Statement.
No competing financial interests exist.