
Abstract
Objectives:
To compare the effectiveness of yoga added to standard care (SC) versus SC only, in women with breast cancer during chemotherapy.
Design:
A multicenter pragmatic, randomized controlled study.
Settings/Location:
Three hospitals in the Netherlands.
Subjects:
Women with stage I–III breast cancer undergoing chemotherapy.
Interventions:
Women were randomized either to a program based on Dru Yoga, once a week yoga sessions for 12 weeks (N = 47), or SC only (N = 36).
Outcome measures:
Primary outcome fatigue (Multidimensional Fatigue Inventory [MFI]; general fatigue) and secondary outcomes fatigue (MFI, Fatigue Quality List [FQL]), quality of life (30-item Quality of Life Questionnaire-C of the European Organization for Research and Treatment of Cancer [EORTC-QLQ-C-30]) and psychological distress (Hospital Anxiety Depression Scale [HADS], Impact of Events Scale [IES]) were measured at baseline (T0), 3 months (T1), and 6 months (T2) and analyzed on observed cases. Other outcomes were adequate relief, reintegration to work, and adverse events.
Results:
No significant differences were found in general fatigue at T1 (MFI: yoga; 14.6 ± 4.5 vs. SC; 14.2 ± 4.2, p = 0.987). Similar findings were observed for other fatigue (sub)scales of MFI and FQL and functional domains of EORTC. With respect to EORTCs symptom scales, women in the yoga group reported significantly less nausea and vomiting compared with SC at T2 (p = 0.004), but not at T1 (p = 0.807). Depressive symptoms were significantly lower with yoga at T1 (HADS: yoga; 4.7 ± 4.1 vs. SC; 5.1 ± 4.2, p = 0.031). More women in the yoga group experienced adequate relief compared with SC at T1 (yoga; 51% vs. SC; 19%) and had returned to work at T2 (yoga; 53% vs. SC; 23%). No adverse events were reported with yoga.
Conclusions:
A Dru-based yoga program failed to demonstrate a significant beneficial effect on fatigue. Possible favorable effects of the yoga program on nausea and vomiting and early return to work in breast cancer survivors warrant further research.
Introduction
A
Several cross-sectional studies 6 –8 and longitudinal studies 9,10 have reported greater fatigue among breast cancer survivors who received chemotherapy compared with those who received no adjuvant chemotherapy. In addition to fatigue arising as a consequence of the cancer itself and the treatment women receive, psychological distress, such as depression, somatization, anxiety, and sleep disturbances can also contribute to fatigue during cancer treatment. 11 Chemotherapy-related fatigue does not diminish over a 3-year follow-up period, 12 and can last up to 10 years after treatment. 13
Persistent fatigue has a negative impact on daily activities, social relationships, and work, and causes significant impairment in the overall quality of life among breast cancer survivors. 6,14,15 It is therefore of utmost importance to investigate effective strategies that can prevent or reduce the prolonged impact on fatigue in breast cancer survivors.
Despite the high prevalence of cancer-related fatigue, there is limited evidence for interventions to manage this symptom. A Cochrane review concluded that there is no solid evidence for the effectiveness of psychosocial interventions in reducing fatigue during cancer treatment, due to the heterogeneity of the published studies. 16 Although there is growing evidence that physical exercise has positive effects on fatigue, 17 cancer survivors are often unable to exercise because of their severe fatigue condition itself. 18 Therefore, yoga was proposed as a possible promising intervention to reduce fatigue in women with breast cancer, since it involves soft movements to develop strength, flexibility, and relaxation of the body and mind. 19 Cramer et al. 20 conducted a systematic review and reported that yoga, either during or after cancer treatment, may have beneficial effects on fatigue in breast cancer survivors, but that risk of publication bias could not be ruled out.
At the initiation of the current study, only two pilot studies were published that reported positive effects of yoga during chemotherapy on fatigue in women with breast cancer. Reduction of fatigue was observed in a small single-arm study in women with breast or ovarian cancer. 21 Another pilot study demonstrated a significant reduction in fatigue in women with breast cancer, but only upon within-group analysis (yoga group) and not in between-group analysis (yoga vs. control group). 22 Accordingly, although there is some evidence supporting the beneficial effects of yoga on fatigue in women with breast cancer during chemotherapy, additional randomized controlled trials (RCTs) with yoga interventions are needed to confirm its effectiveness.
The present study was initiated to investigate the effects of a yoga program during chemotherapy on fatigue and quality of life in women with breast cancer when added to standard care (SC) compared with SC only. To the best of our knowledge, this is the first RCT in the Netherlands that investigated the effectiveness of yoga on fatigue and quality of life in women with breast cancer.
Materials and Methods
Study design and participants
A multicenter pragmatic, randomized controlled study with two parallel groups was performed in three hospitals in the Netherlands: St Jansdal Hospital (Harderwijk), Alexander Monro Hospital (Bilthoven), and Flevo Hospital (Almere). Women between 18 and 70 years with stage I–III breast cancer who were scheduled for (neo) adjuvant chemotherapy were eligible for the study. They had to understand and speak the Dutch language and have access to phone and internet. Written informed consent was obtained before inclusion in to the study. Women who had received previous treatment with cytostatics were excluded from the study. Other exclusion criteria were: presence of metastasis or other malignancies, irresectable tumors, deafness, serious psychiatric or cognitive problems, or participating in other yoga or stress-reduction programs at the time.
Intervention
Women were randomized to either SC (control group) or SC plus the yoga program. SC was provided according to the hospital guidelines. This was an individual mixture of (neo) adjuvant chemotherapy, surgery (mastectomy or lumpectomy), radiotherapy, and/or immunotherapy, as well as support from oncology nurses throughout the process. The yoga program consisted of weekly sessions of 75 min at the hospital over a period of 12 weeks. Women entered the yoga program 1–2 weeks before the start of chemotherapy. The program was based on Dru Yoga 23 and specifically designed for women with breast cancer to reduce fatigue and improve quality of life. Dru Yoga is a style of yoga that is commonly practiced in the Netherlands as well as the United Kingdom. The content of the yoga program is summarized in Table 1.
In addition to the weekly sessions, women were provided with a CD or MP3 download with 20 min breathing and relaxation exercises to practice at home. Women were encouraged to practice at home daily with a minimum of 5 min. The yoga program was developed and provided by yoga instructors of the Clyms Institute in Harderwijk, the Netherlands. The instructors were certified in Dru Yoga and had more than 5 years of experience in working with cancer patients. Women in the SC group were offered to participate in the yoga program after the study.
Randomization
Women were assigned to one of the following four strata, mastectomy, lumpectomy, neoadjuvant chemotherapy, or adjuvant chemotherapy, taking into account prognostic factors which may interfere with therapy outcome. 12,16 They were subsequently randomized using separate randomization lists for each study center, as generated by the computerized Random Allocation Software Program with a random block size of 10 to guarantee balanced allocation. The study monitor was blinded for allocation sequence and assigned subjects to the groups.
Outcome measures
Outcomes were measured at baseline (T0), 3 months (T1), and at 6 months (T2) follow-up. Primary outcome was the general fatigue scale at T1, measured by the 20-item Multidimensional Fatigue Inventory (MFI), which also measured physical and mental fatigue. 24 Another more qualitative fatigue measurement used was the 18-item Fatigue Quality List (FQL) assessing women's perception and appraisal of experienced fatigue. 25 Another secondary outcome was health-related quality of life measured using the 30-item Quality of Life Questionnaire-C of the European Organization for Research and Treatment of Cancer (EORTC-QLQ-C-30), 26 adjusted with the 23-item breast cancer-specific module: EORTC QLQ-BR23. 27 Other secondary outcomes were psychological distress as measured by the 14-item Hospital Anxiety Depression Scale (HADS), 28 the 22-item Impact of Events Scale (IES), 29 and treatment expectations measured by the Participants Expectations questionnaire. 30 Adequate relief of fatigue (yes/no) and return to work were assessed in semistructured telephone interview carried out by the research physician. In addition, the occurrence of study-related adverse events was monitored.
Sample size
Calculation of the sample size was powered to a 21% point difference between the control and yoga group with respect to the primary outcome of self-reported fatigue (MFI: general fatigue) at 3 months follow-up. This assumption was based on results from two previous studies investigating the effects of yoga on fatigue in breast cancer survivors. 31,32 A sample size of 43 women per group provided 80% power assuming a significance level of 0.05. To control for an estimated 20% dropout rate, the total number of women required per group was calculated to be 52, and 104 women in total.
Statistical analyses
Main statistical analyses were per-protocol (PP) analysis, based on observed data from women who were randomized and followed-up for 3 and 6 months in the study. Baseline demographic and clinical characteristics were calculated using t-tests for continuous and ordinal variables. Chi-square tests were used to compare nominal variables.
Within-group analyses were performed to estimate the effects of the intervention after 3 and 6 months compared with baseline using t-tests or Mann–Whitney U tests if the variables were not normally distributed.
Between-group analyses were performed using t-tests or Mann–Whitney U tests for the individual time points. Analysis of covariances (ANCOVAs) was used to test for intervention effects over time, controlling for baseline differences, interaction effects between baseline and intervention, and age. Effect sizes were given as eta squared (η2). Differences in adequate relief between the groups were calculated using the chi-square test. Further subgroup analyses with respect to tumor type and surgery method were performed for the primary outcome measures only. For each time point between-group analyses (SC vs. yoga) were conducted using t-tests.
Ethical and legal considerations
All procedures performed in the study were in accordance with the national regulation, the Helsinki declaration, and the International Conference on Harmonization guideline for Good Clinical Practice. Medical ethical approval was obtained from the METOPP Tilburg (Study No. NL 41230.028.12; M490). Trial Registration Number was NTR 3701, 24 November 2012 (
Results
Study population
The time needed to recruit the calculated number of 104 women in the study was originally estimated at 2 years and recruitment was planned at one hospital only (St. Jansdal). Two years after the start of the study, only half (n = 52) of the required number of women were recruited. In 2015 it was therefore decided to start recruitment at two additional centers, the Alexander Monro Hospital and Flevo Hospital. Despite this effort, recruitment remained at a lower than anticipated rate. As shown in Figure 1, a total of 239 women were assessed for eligibility, of which 156 were excluded.
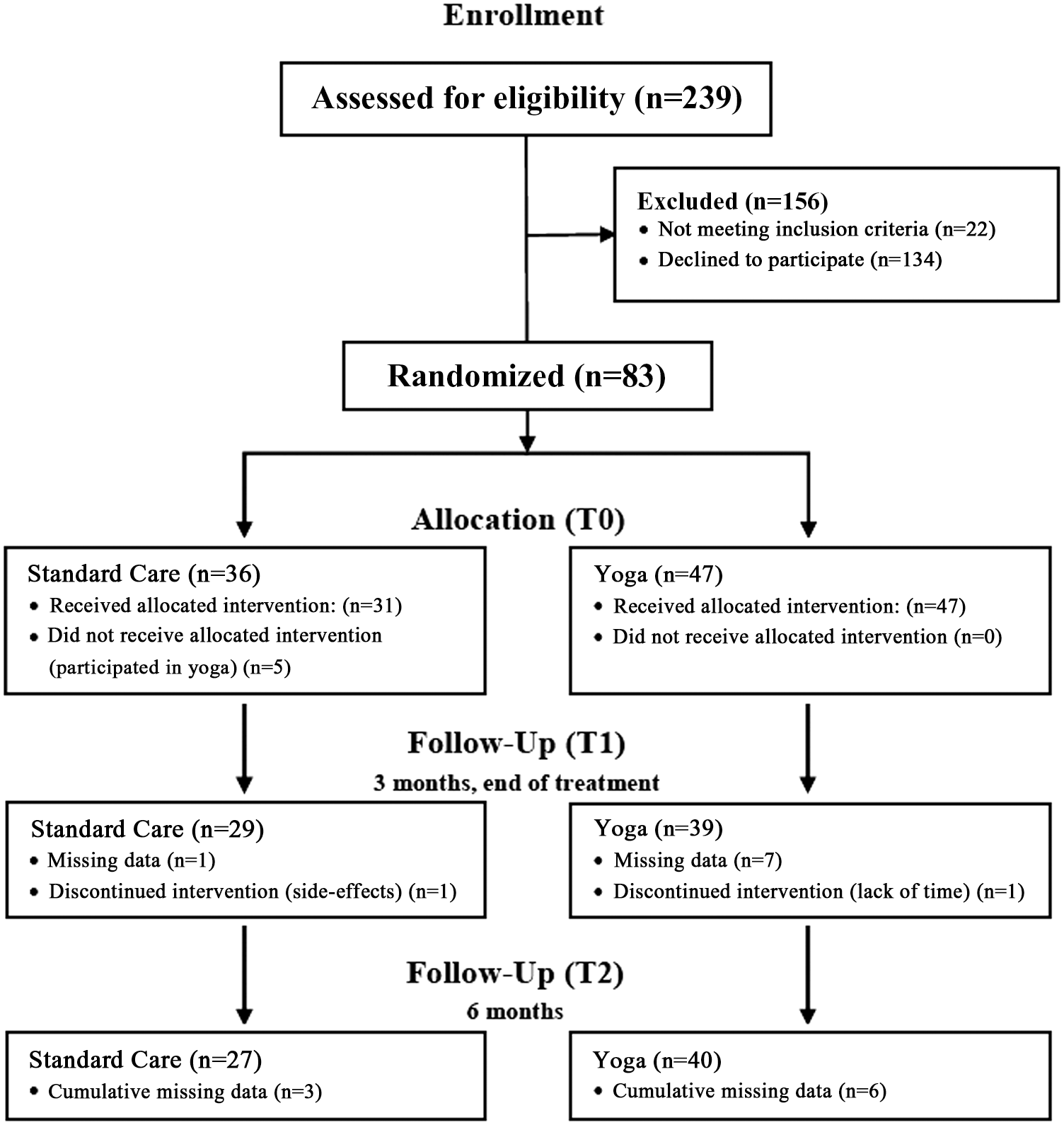
Flow chart of women in the study.
Of those excluded, 22 did not meet the inclusion criteria and 134 declined participation for several reasons (not interested in yoga [n = 29], too much to participate in a study [n = 16], too long a travel distance to the hospital [n = 12], and unknown reason [n = 77]). After 4 years, it was decided to stop recruitment for the study ending up with a total of 83 women that were randomized in the study (Fig. 1). Since women enrolled were stratified into 4 strata, each with a random block size of 10, it happened by coincidence that more women were allocated to the yoga program (n = 47) than to SC (n = 36). Five women in SC did not receive the allocated intervention as planned, but participated in the yoga program during the course of the study. Furthermore, two women (yoga program: n = 1; SC: N = 1) dropped out of the study (Fig. 1).
As shown in Table 2, about two-third of the women in both groups had undergone lumpectomy, and about one-third mastectomy. All women received chemotherapy, the majority in both groups before surgery (neoadjuvant). PP analysis demonstrated that groups were comparable with respect to most demographic characteristics, except for scheduled adjuvant hormone therapy and higher treatment preference for SC in women in the yoga group (Table 2).
p-values < 0.05 are presented in bold.
Data are mean (SD) or n (%), p-values of continuous variables are calculated with t-tests, p-values of categorical variables are calculated with chi-square tests.
SC, standard care.
Fatigue
As shown in Table 3, the primary outcome, general fatigue (dimension of MFI) was significantly higher in the yoga group at T0, compared with SC only. Upon PP analysis, a significant increase in general fatigue was observed from T0 to T1 in SC (p = 0.006), but not in the yoga group (p = 0.175). However, no significant difference was observed in general fatigue between the groups at T1 (Table 3). At T2, general fatigue remained high in SC. With respect to other dimensions of MFI and FQL, both groups were comparable at T0. Significant differences in the domains of fatigue (both MFI and FQL) were found within the groups at either T1 or T2 months, compared with T0 (Table 3). However, for none of these other fatigue subscales significant differences could be observed between the groups at T1 or T2 (Table 3).
p-values < 0.05 are presented in bold.
Differences calculated for MFI subscales with t-test, for FQL subscales with Mann–Whitney U test.
ANCOVA, analysis of covariance; FQL, Fatigue Quality List; MFI, Multidimensional Fatigue Inventory; SC, standard care; T0, baseline; T1, 3 months; T2, 6 months.
Additional (ANCOVA) analyses demonstrated that for three domains of MFI, there was a significant interaction between the intervention effect over time and the age of women, that is, the higher the age the higher the score on MFI (physical fatigue: p = 0.0316, reduced activity: p = 0.0017, reduced motivation: p = 0.0099). Subsequent (ANCOVA) subgroup analyses for age groups (cutoff point: <53 vs. ≥53 years) did not demonstrate significant differences between the yoga and SC group in MFI and FQL domains. Further additional subgroup analyses with respect to specific tumor types and type of surgery and the primary outcome general fatigue did not demonstrate any significant differences between the two groups (results not shown). However, sample sizes in the subgroup analysis were probably too small to detect any possible significant differences.
Quality of life
As shown in Table 4, both groups significantly differed at baseline with respect to emotional, cognitive, and social functioning, as well as the subscales, body image, and future perspectives of the QLQ-BR23. Overall, EORTCs functional scales global health status, physical functioning, and role functioning decreased from T0 to T1 in both groups, and returned to baseline levels at T2, indicating recovery of women's quality of life after chemotherapy. Women in the yoga group significantly improved on emotional functioning at T1 (p = 0.045) and T2 (p = 0.001). No changes were observed in both groups with respect to cognitive and social functioning. Overall, there were no significant differences at T1 or T2 between the two groups (ANCOVA) regarding any of the EORTCs functional scales (Table 4). With respect to EORTCs symptom scales, women in the yoga group reported significantly less nausea and vomiting compared with SC at T2 (p = 0.004), but not at T1 (p = 0.807). There were no significant differences between both groups (ANCOVA) on any of the other EORTCs symptom scales or EORTC QLQ-BR23 domains (Table 4).
p-values < 0.05 are presented in bold.
Differences calculated with t-test.
T0: Intervention interaction term is significant, p = 0.048 and effect size is 0.059.
T0: Intervention interaction term is significant, p = 0.038 and effect size is 0.065.
ANCOVA, analysis of covariance; EORTC-QLQ-C-30, 30-item Quality of Life Questionnaire-C of the European Organization for Research and Treatment of Cancer; SC, standard care; T0, baseline; T1, 3 months; T2, 6 months.
Psychological distress
Both groups differed significantly at T0 with respect to anxiety and depression, the yoga group being worse (Table 5). Anxiety improved significantly in time in the yoga group (T1 and T2, compared with T0), but not in SC (Table 5). However, no significant differences were observed between the two groups with respect to anxiety at T1 and T2 (Table 5). A significant difference between the two groups (ANCOVA) was found for depressive symptoms at T1, in favor of yoga (Table 5). The impact of events score was not significantly different between the yoga and SC group (Table 5).
p-values < 0.05 are presented in bold.
Differences calculated with t-test.
ANCOVA, analysis of covariance; HADS, Hospital Anxiety Depression Scale; IES, Impact of Events Scale; SC, standard care; T0, baseline; T1, 3 months; T2, 6 months.
Participants' expectations and adequate relief
At T1, confidence in fatigue reduction and amount of expected fatigue reduction were significantly increased in the yoga group compared with the SC group (Table 6). Actual experienced fatigue reduction (adequate relief) was reported in a significantly higher percentage of women in the yoga group (51%), compared with the SC group (19%) at T1 (p < 0.001) (Table 6).
p-values < 0.05 are presented in bold.
The p-value of “Experienced sufficient fatigue reduction” is calculated using the chi-square test, Mann–Whitney U test is used for the variables “confidence in fatigue reduction” and “expected fatigue reduction.”
ANCOVA, analysis of covariance; SC, standard care; T0, baseline; T1, 3 months.
Return to work
Before start of the study, most women in both groups had paid work (yoga: 84%; SC: 72%). At T1, the majority of women had stopped working (yoga: 71%, SC: 73%). At T2, the percentage of women that had returned to work was considerably higher in the yoga (53%) compared with the SC group (23%). Women that had not returned to work was lower in the yoga (21%) compared with the SC group (42%). In one-third of the participants, data on working status were lacking (yoga: 26%, SC: 35%).
Participation in the yoga program
Fifty percent of women in the yoga group participated in all 12 classes as offered during the study. In total, 87% of women in the yoga group participated in at least eight or more classes in the yoga program. Reasons for not being able to participate in all classes offered were: feeling too ill (25%), other appointments (10%), or travel distance to the hospital where the yoga program was given (6%).
In semistructured interviews with women in the yoga group at T1, 45% of the women expressed that yoga improved their fatigue complaints. As one woman expressed, “I experience more energy after having participated in the program.” Women were also asked which possible other effects they experienced with yoga. The majority (87%) expressed that the yoga program had supported them in feeling better, more relaxed, and at ease. As one woman expressed, “I experience less anxiety and panic.” Or another woman: “I experienced calmness during yoga class.” To have contact and meet with other women was also mentioned as one of the benefits of yoga by many women (49%). Other effects of yoga were better dealing with cancer treatment (23%), better breathing (13%), and better sleeping (13%).
Adverse events
A total of 57 adverse events were reported by 25 out of 31 (81%) observed women in the yoga group and 45 adverse events were reported by 20 out of 25 (80%) observed women in the SC group. The remaining 20% of women in both groups reported that they either had no obvious/remarkable side effects or no obvious/remarkable side effects that interfered with their cancer treatment. Most commonly reported adverse events were peripheral neuropathy (yoga: n = 8; SC: n = 7), fatigue (yoga: n = 6; SC: n = 6), and nausea (yoga: n = 5; SC: n = 4). All adverse events were assessed as likely to be caused by chemotherapy or other SC. None of the adverse events was assessed as being related to the yoga program.
Discussion
Major findings
The present study demonstrated that participation in a yoga program during chemotherapy does not significantly reduce fatigue in women compared with SC only. These results are in line with two recently published studies on the effects of yoga during (neo)adjuvant treatment in women with breast cancer. 33,34 In a study from Germany, it was demonstrated that during chemotherapy, fatigue improved upon a physical exercise intervention but not upon an Iyengar Yoga intervention. 34 A study from the United States of America reported no significant difference in fatigue levels over time between women with breast cancer who were undergoing chemotherapy and followed a Tibetan yoga program, a stretching program, or SC. 33
The yoga program had some beneficial effects in women regarding secondary outcomes, compared with SC. A significant effect was observed with respect to reduction in nausea and vomiting with yoga versus SC after 6 months. Since it is known that nausea and vomiting negatively impacts health-related quality of life of women with breast cancer, 35 it is of interest to further investigate the effects of yoga programs on reduction of these side effects.
Furthermore, women in the yoga program had significantly less depressive symptoms and more adequate relief (51%) compared with women receiving SC only (19%) at 3 months. It seems unlikely that this difference was due to treatment expectations, since expectation with SC was found to be higher in the YBSR group. The fact that more women in the YBSR program experienced adequate relief compared with SC, could explain the observation that after 6 months considerably more women in the YBSR program had returned to work (53%), compared with SC (23%). These findings, however, have to be interpreted with caution since numbers were small and data of some participants were missing. Very little is known about effects of yoga on return to work of breast cancer survivors. 36 Further studies on the possible beneficial effects of yoga on occupational rehabilitation are therefore recommended.
Limitations
There are several limitations of the present study that need further reflection. First of all, recruitment of women in the study was extremely challenging. Inclusion of women at three study centers during a period of 4 years was still not sufficient to reach the estimated sample size. Similar recruitment problems were identified in the two previously published trials studying the effect of yoga programs in women with breast cancer undergoing chemotherapy. 33,34 Furthermore, Chaoul et al. 33 reported that ∼22% of patients dropped out of the study and another 20% did not provide follow-up data. In the study by Lotzke et al., 34 a dropout percentage as high as 59% was reported. It therefore appears that participation in a RCT during chemotherapy might be too exhausting for women with breast cancer.
Another limitation of the present study was that due to prestratification, block size of randomization and inclusion at three study centers, more women were randomized to the yoga program than to SC. This resulted in an imbalance of participants between the two groups. The large difference in group size probably explained the finding that the two comparison groups differed at baseline for several primary and secondary outcome parameters. Overall, women in the yoga program seemed to be doing worse at baseline than women in SC. The finding that more women in the yoga group experienced adequate relief compared with SC, could therefore possibly be explained by the fact that levels of fatigue were higher at baseline in the yoga group.
Furthermore, since five women in the control group had participated in the yoga intervention under investigation, this study did not follow common recommendations to perform an intention-to-treat analysis. Instead a PP analysis was performed to exclude those women in the control group with protocol violations. In the PP analysis missing data were not imputed. Follow-up data on the primary outcome were missing for 17% of the women in the yoga and 6% in the SC group at T1, and 15% in the yoga and 13% in the SC group at T2. Additional analysis demonstrated that there were no systematic differences with regard to clinical characteristics between those women who provided follow-up data or those women that had missing data, thereby minimizing concerns of a biased sample in the PP analysis. However, due to the underpowered and imbalanced study, results have to be interpreted with caution.
Practical implications
Although this study did not demonstrate a significant effect of the yoga program in the reduction of fatigue as measured using MFI, it was interesting to note that the yoga program had beneficial effects for women with regard to greater adequate relief and earlier return to work. Since the yoga program was found to be safe and appreciated by the majority of women, based on individual preferences, women may therefore consider to participate in yoga-based supportive programs during chemotherapy. However, further research is needed before definite recommendations can be made whether to participate in a yoga-based supportive program during chemotherapy to effectively manage breast cancer-related fatigue.
Since the present study and two previously published RCTs 33,34 all demonstrated difficulties with recruitment as well as keeping women in the study, the methodology of an RCT does not seem to be the most suitable design to further investigate the effects of yoga during chemotherapy. It would be of interest for future research to routinely evaluate outcomes of integrative oncology programs for women with breast cancer, 37,38 which include yoga, and subsequently investigate changes in the occurrence of side effects, such as fatigue, nausea, and vomiting.
In such more pragmatic observational studies, it could also be investigated for which subgroup of breast cancer patients yoga might be the most beneficial. A previous Cochrane review showed that there is sufficient evidence from RCTs to conclude that yoga is an effective modality to reduce cancer-related fatigue in breast cancer survivors who have completed cancer treatment, so after completing chemotherapy. 39 In addition to yoga, mindfulness-based stress reduction has also been demonstrated to reduce fatigue in women after breast cancer treatment, although reduction in fatigue was only observed in the short term. 40 A supportive intervention that seems to effectively reduce fatigue in women with breast cancer during chemotherapy is exercise. 41,42 A moderate- to high-intensity combined resistance and aerobic exercise program was demonstrated to significantly reduce fatigue in women with breast cancer undergoing adjuvant chemotherapy compared with SC. 43
Conclusions
No significant effect on fatigue was demonstrated in this study compared with SC of a Dru-based yoga program offered to women with breast cancer receiving chemotherapy with curative intent. The present study suffered from several limitations. Further studies are warranted to investigate favorable effects of yoga on fatigue before definite conclusions can be drawn. Furthermore, results of our study offer a starting point for investigating the effect of yoga on other relevant endpoints, such as occupational rehabilitation and nausea/vomiting.
Footnotes
Acknowledgments
The authors would like to thank all women who have participated in this study. They also express their gratitude to those that have contributed to the study: Clementine Vos, Lucile de Zeeuw, Gerrie Steijaert-van Eerbeek of CLYMS (Harderwijk), Roberto Tobon Morales, Gerda Kroon, Jenneke Klunder, Caroline Celie, Pauline Groeneveld, Nienke van de Broek, Judith Amsing, Mariska Scheuer of St Jansdal Hospital (Harderwijk), Sissi Grosfeld of Alexander Monro Hospital (de Bilt), and Lisa Wobma of Flevo Hospital (Almere). They thank Ellen van der Pol for assisting in data entry and analysis. This study was funded by Pink Ribbon (Grant: 2011,W016.C97).
Author Disclosure Statement
No competing financial interests exist.