
Abstract
Objectives:
This study aims to investigate the effects of t'ai chi and qigong (TCQ) training on severity of obstructive sleep apnea (OSA).
Design:
A prospective, 12-week, single-center, double-blinded, randomized controlled trial.
Setting:
Sleep Disorders Center of Medical Faculty in Istanbul, Turkey.
Subjects:
Fifty adult patients with mild and moderate OSA.
Interventions:
Patients were randomly allocated into either an intervention group or a control group. The intervention group (n = 25) received TCQ training under physiotherapist supervision for 1 h, three times per week, for 12 weeks and a home exercise program was provided for another 2 days. The control group (n = 25) received only a home exercise program for 12 weeks, 5 days per week.
Outcome measures:
All patients were assessed before and after the exercise program. Objective parameters of sleep were measured by polysomnography, while subjective parameters of sleep were assessed using the Epworth Sleepiness Scale (ESS) and the 3-factor Pittsburgh Sleep Quality Index (PSQI). Pulmonary functions were assessed with a pulmonary function test; health-related quality of life was evaluated through the Short Form-36.
Results:
In the intervention group, there was a statistically significant decrease in the apnea–hypopnea index (AHI) (p = 0.001) and percentage and duration of stage N2 sleep (p = 0.041 and p = 0.037, respectively), while there was a statistically significant increase in percentage and duration of stage N3 sleep when compared with the controls (p = 0.048 and p = 0.043, respectively). There was a statistically significant decrease in the ESS, PSQI sleep efficiency, and total scores (p = 0.001, p = 0.003, and p = 0.003, respectively).
Conclusions:
Our study results suggest that TCQ training may reduce AHI and daytime sleepiness, while improving subjective sleep quality, in patients with mild and moderate OSA.
Introduction
Obstructive sleep apnea (OSA) is a clinical condition characterized by repetitive obstruction of the upper airway during sleep. 1 In OSA patients, snoring is the most frequently reported nocturnal symptom along with daytime sleepiness. If left untreated, OSA may lead to serious health problems, including cognitive disorders, 2 cardiovascular diseases, 3 type 2 diabetes, and early mortality. 4
Epidemiological studies have demonstrated that physically active individuals have a lower risk of OSA compared with the less physically active individuals. 5 Furthermore, interest in exercise training has been rapidly increasing in patients with OSA. According to the summary results of a meta-analysis 6 exploring this topic, exercise training in patients with OSA significantly reduces the apnea–hypopnea index (AHI) and provides a significant improvement in sleep quality and daytime sleepiness independent of body mass index (BMI). This suggests the possible role of exercise in the treatment of sleep apnea.
T'ai chi (TC) is a traditional Chinese martial art and, currently, it is commonly used for health benefits. 7,8 Having many different forms, TC is a combined exercise consisting of slow coordinated movements with varying weight, postural alignment, and synchronized deep breaths, which includes many mental and physical elements. TC has been designed to stretch and strengthen the body; improve the flow of blood 9,10 and other fluids in the body such as lung secretion, 11 lymph fluid, 12 renal functions, 13 and endocrine secretions 14 –17 ; and raise awareness regarding balance, proprioception, and the way the body moves in space. 7 Qigong exercises form a basis for TC and regulate the mind, body, and breathing similar to TC, and these exercises have been shown to improve fatigue, anxiety, depressive symptoms, and sleep disorders. 18,19
In previous studies, long-term TC exercises were shown to positively affect physical function, exercise capacity, and psychological status, as well as support, in the treatment of chronic diseases. 20 However, there appear to have been very few studies that have explored the effects of t'ai chi and qigong (TCQ) training in patients with OSA.
In the present study, therefore, we aim to investigate the effect of TCQ training on OSA severity and to examine changes in the several objective and subjective parameters affecting sleep and quality of life in patients with OSA.
Methods
Study design
This was a 12-week, single-center, double-blind, randomized controlled trial.
Study participants
Between January 2016 and January 2017, a total of 50 patients with mild (AHI: 5–15) and moderate (AHI: 15–30) OSA, as assessed by all-night polysomnography (PSG) at the Sleep Disorders Center, Department of Pulmonology, Medical Faculty Hospital, Bezmialem Vakif University, were included in this study.
These 50 patients were randomly allocated into either an intervention group or a control group. The intervention group (n = 25) received TCQ training under physiotherapist supervision for 1 h, three times per week, for 12 weeks and a home exercise program was provided for another 2 days. The control group (n = 25) received only the home exercise program for 12 weeks, 5 days per week.
Inclusion criteria were as follows: subjects with a recent diagnosis and untreated mild and moderate OSA (30 ≥ AHI ≥5), between the ages of 30 and 65 years, a BMI of ≤35 kg/m2, and being physically inactive—defined as irregular exercise habit (<2 exercise sessions/week). Subjects who were excluded from the study were those with severe OSA (AHI ≥30); those having OSA treatments (continuous positive airway pressure (CPAP), oral devices, nasal surgery, tennis ball/positional therapy, diuretic, etc.); those taking hypnotic or sedative medications; those with a morphological defect (facial malformation, etc.), which can cause sleep disorders; those with a history of smoking or alcoholism; those having orthopedic, neurological, or musculoskeletal problems, which impede exercising; pregnant women; and those with uncompensated clinical conditions such as chronic obstructive pulmonary disease, interstitial pulmonary disease, heart failure, or rheumatic and psychiatric illnesses.
This randomized controlled study was approved by the Ethics Committee of Non-Interventional Clinical Trials, Institute of Medical Sciences, Medipol University, Istanbul, Turkey. All participants signed written informed consent forms. The study was conducted in accordance with principles of the Declaration of Helsinki.
Outcome measures
All assessments were performed before the start of the exercise program and at week 12, following completion of the program. The PSG (M.E.A.) and pulmonary function test (PFT) (L.K.) results were evaluated by pulmonologists. The Epworth Sleepiness Scale (ESS), Pittsburgh Sleep Quality Index (PSQI), and the Short Form-36 (SF-36) questionnaire were completed by each patient.
Polysomnography
PSG was performed using the Compumedics E 3142 PSG device (Compumedics, Inc., Melbourne, Vic., Australia). Participants were prepared for recording with a standard PSG montage. 21 An electroencephalogram (C3/M2, C4/M1, O1/M2, O2/M1), bilateral electrooculogram, and submentalis electromyogram (EMG) were used to assess sleep stages, which were scored according to the Rechtschaffen and Kales criteria. 21 For respiration, nasal flow was assessed using a nasal cannula with a pressure transducer; a thermistor was used for oral and nasal respiration. Thoracic and abdominal movements were measured using inductance plethysmography, oxyhemoglobin saturation was measured using pulse oximetry, and snoring was measured with a tracheal microphone. Sleep position was determined using a position sensor. An electrocardiogram (V2 modified) was used to access heart rate variability. An anterior tibial EMG was also used to detect periodic limb movements.
Apnea was defined as the complete interruption of airflow for more than 10 sec, while hypopnea was defined as at least a 30% reduction in the oronasal airflow for 10 sec or more, with at least 3% oxygen desaturation compared with previous breathing events or development of arousal. AHI was obtained by dividing the total number of apnea and hypopnea episodes by the total sleep time. 21 OSA severity is defined as mild for AHI ≥5 and <15; moderate for AHI ≥15 and ≤30; and severe for AHI >30/h. 21 The arousal index was calculated as the number of arousals per hour of sleep. 21 PSG was scored by a pulmonologist who was blinded to the other experimental data and to randomization.
Pulmonary function tests
PFTs were performed using the ZAN 100 USB″ (nSpire Health GmbH, Germany) spirometer and applied according to the American Thoracic Society and European Respiratory Society guidelines. 22
Epworth sleepiness scale
The ESS is a questionnaire containing eight items that measure the likelihood of dozing during typical daytime activities. 23 The ESS score (the sum of eight-item scores, 0–3) can range from 0 to 24. Higher ESS scores indicate higher average sleep propensity in daily life. 23
Short form-36
The SF-36 is one of the most common generic measures of quality of life. It is not specific to any age, 24 illness, or treatment group. 25 –28 The total score ranges between 0 and 100 with its eight items, including physical functioning, physical status, general health, vitality, social functioning, emotional status, mental health, and bodily pain. Higher scores indicate a better health status. 28
Pittsburgh Sleep Quality Index
The PSQI is a questionnaire that evaluates sleep quality and patterns according to seven components, including subjective quality of sleep, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleep medication, and daytime dysfunctions. 29 The questions are scored between 0 and 3, and higher scores indicate poor quality of sleep. 29 Sleep quality was analyzed based on the 3-factor PSQI model proposed by Cole et al. 30 Confirmatory analysis performed by those authors yielded three factors: factor 1, sleep efficiency (sleep duration and sleep efficiency components); factor 2, sleep quality (subjective sleep quality, sleep latency, and sleep medication use components); and factor 3, daily disturbances (sleep disturbances and daytime dysfunction components). Similarly, we used a 3-factor PSQI model in our study.
Exercise program
TCQ exercises
The intervention group received a supervised TCQ training program for 3 days per week, 1 h per day, for 12 weeks. Patient leaflets, containing pictures of the same movements and same duration, were prepared, and patients were instructed to perform exercises at home for 2 days. The supervisor is a physiotherapist (G.Y.G.) who was a trainee of an instructor with 17 years of experience on Level II TC and Zhan Zhuang Chi Kung. 31 The TCQ training program was developed in collaboration with the instructor (Table 1). 32 –34 Before starting the exercises, Tan Tien breathing was taught and exercises were performed through this breathing technique. Tan Tien lies 3 cm below the navel, one-third of the way into the body. The participant slowly inhales through the nose toward the navel and exhales through the nose. 32
T'ai Chi and Qigong Training Program
Exercises performed using Tan Tien breathing.
Training program lasts for 60 min, including rests.
TCQ, t'ai chi and qigong.
The training program lasted for 60 min, including rests. The TCQ training was performed within intensity ranges of 11–13 (light to somewhat hard) as per the Borg ratings of the Perceived Exertion Scale. 35 Exercises were performed in a standing position with four to six participants in each group in the exercise room at the pulmonary rehabilitation unit of the University Hospital.
Home exercise program
The home exercise program was administered to the control group. All patients were informed about the exercises, which were demonstrated by applied training. The home exercise program consisted of breathing and posture exercises (Table 2). An exercise schedule was given to each patient and they were instructed to perform the exercise for 12 weeks, 5 days weekly. Patients were asked to note the exercise days in their exercise diaries. The patients were scheduled for monthly telephone follow-ups.
Control Group Home Exercise Program
Although no change in OSA severity was expected in the control group, the simple exercise program that was provided was designed to increase the motivation of patients, facilitate their follow-up, and increase their adherence to the study.
Randomization
After eligible patients were enrolled in the study by the pulmonologist (M.E.A.), they were directed to the pulmonary rehabilitation unit. Allocation was implemented there using a numbered series of 50 prefilled envelops specifying group assignment, which had been previously generated by the statistician using a computer-based program. Neither the physicians who evaluated the patients nor the patients themselves were aware of which patients belonged to the training or the control group.
Statistical analysis
Based on the results of previous exercise training studies, 36 it was calculated that the study and control groups should have 22 cases each to detect a 4.18 change in AHI with 80% power and 95% confidence interval. Statistical analysis was performed using the Statistical Package for Social Sciences (SPSS) for Windows, version 21.0, software (IBM Corp., Armonk, NY). Normally distributed continuous data are expressed as mean ± standard deviation, while non-normally distributed continuous data are expressed as median [interquartile range]. Descriptive variables were expressed in percentage (%). A one-sample Kolmogorov–Smirnov test was used to analyze the normality of distribution. To compare intragroup pre- and postintervention data, the Wilcoxon signed-rank test was used for non-normally distributed data, while a paired sample t-test was used for normally distributed continuous data. To compare intergroup differences, the Mann–Whitney U test was used for non-normally distributed data, while an independent samples t test was used for normally distributed continuous data. A chi-square test was used to compare nominal variables. All data were analyzed for the intention-to-treat (ITT) effect. The ITT analysis contained all participants, including those who were not fully compliant and those who had missing outcome data. A p-value of <0.05 was considered statistically significant.
Results
Participant characteristics
A summary of participant flow is provided in Figure 1. Of 50 participants, 31 were males and 19 were females. Demographic and clinical characteristics of all participants are shown in Table 3. There was no statistically significant difference in BMI values and neck circumferences between the groups (p > 0.05), while the mean age of the intervention group was found to be significantly higher than the control group (p = 0.041).
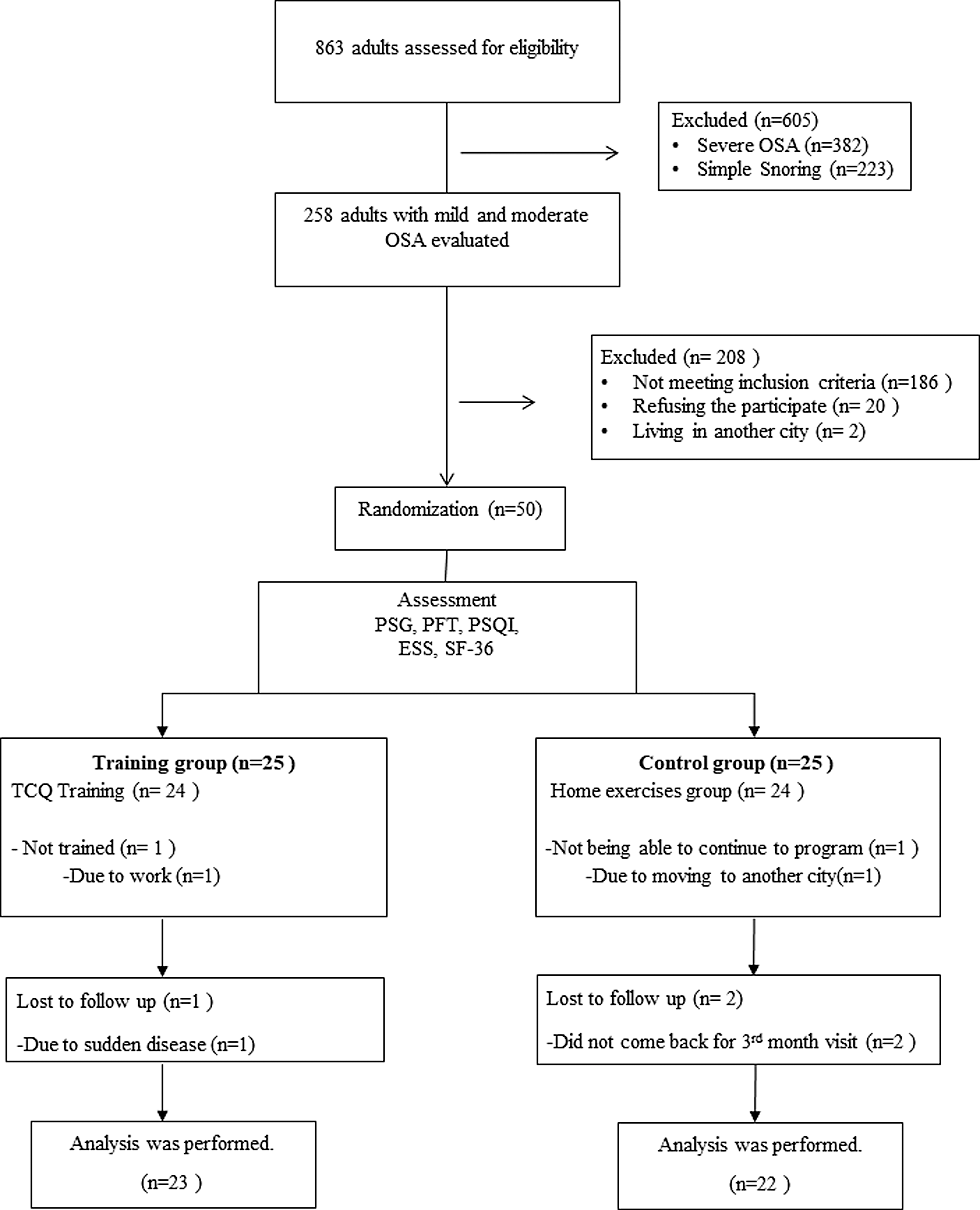
Flow chart. ESS, Epworth Sleepiness Scale; OSA, obstructive sleep apnea; PFT, pulmonary function test; PSG, polysomnography; PSQI, Pittsburgh Sleep Quality Index; SF-36, Short Form-36; TCQ, t'ai chi and qigong.
Demographic and Clinical Characteristics of Patient Groups
Indicates statistically significant results.
BMI, body mass index; OSA, obstructive sleep apnea; SD, standard deviation.
After the program, in the intervention group, the mean BMI was 30.36 ± 2.98 kg/m2, and in the control group, it was 29.32 ± 3.19 kg/m2, indicating no significant difference between the groups (p > 0.05). In addition, there was no significant difference in neck circumferences between the intervention group and control group: 39.16 ± 2.68 cm in the intervention group and 39.72 ± 2.83 cm in the control group (p > 0.05).
Polysomnography
Intra- and intergroup comparisons of PSG parameters of the groups before and after the exercise training are shown in Table 4.
Intra- and Intergroup Comparisons of Polysomnography of Patient Groups Before and After the Exercise Training
Data are presented as mean ± SD, non-normally distributed continuous data are presented as median [interquartile range].
Indicates statistically significant results.
AHI, apnea–hypopnea index; Mean SaO2 Dest, mean SaO2 desaturation; PSG, polysomnography; RemL, Rem latency; SaO2, arterial oxygen saturation; SD, standard deviation; SE, sleep efficiency; SL, sleep latency; Stage R, rapid eye movement sleep; TST, total sleep time.
In the study, our primary outcome was AHI, which was reduced by −5.51 ± 7.28 in the TCQ training group (<0.001), whereas it increased by 1.68 ± 8.22 in the control group (p > 0.05). Compared with the control group, TCQ training resulted in a significant reduction by 7.18 ± 2.19 in AHI (p = 0.001) (Fig. 2). In the lowest SaO2, there was no significant difference between groups (p > 0.05), but there was a significant increase following the TCQ training program (p = 0.040). There was also a significant increase in percentage and duration of stage N3 sleep in the intervention group versus control group (p = 0.048 and p = 0.043, respectively), as well as a significant decrease in percentage and duration of stage N2 sleep (p = 0.041 and p = 0.037, respectively). However, no significant differences were found in sleep parameters in the control group after the exercise program (p > 0.05).

Individual change of AHI from baseline to treatment. AHI, apnea–hypopnea index.
PFT, PSQI, ESS, and SF-36
There were no significant differences in the scores of PFT, PSQI, ESS, and SF-36 parameters between the two groups at baseline (p > 0.05). Intragroup and intergroup comparison of PFT, subjective sleep quality, and health-related quality of life questionnaire results, before and after the exercise training for the groups, is shown in Table 5.
Intra- and Intergroup Comparisons of Pulmonary Function Test, Three Factors: Pittsburgh Sleep Quality Index, Epworth Sleepiness Scale, and Short Form-36 Results Before and After the Exercise Training
Data are presented as mean ± SD.
Indicates statistically significant results.
DD, daily disturbance; ESS, Epworth Sleepiness Scale; FVC, forced vital capacity; FEV1, forced expiration volume in one second; FEV1/FVC, ratio of forced expiration volume in one second to forced vital capacity; PCS, physical component summary; PEF, peak expiratory flow; PFT, pulmonary function test; PSQI, Pittsburgh Sleep Quality Index; MCS, mental component summary; SD, standard deviation; SF-36, Short Form-36; SE, sleep efficiency; SQ, sleep quality.
There were no significant differences in the PFT and SF-36 results in the training and control groups following the exercise training (p > 0.05). In the intervention group, however, there were statistically significant decreases in the 3-factor PSQI: sleep quality (p = 0.017), daytime dysfunction (p < 0.001), and total score (p < 0.001). In the control group, there was no significant change in the 3-factor PSQI. In addition, we found statistically significant decreases in sleep efficiency (p = 0.042) and total score (p = 0.003) in comparison with the control group.
In the intervention group, there was a statistically significant decrease in ESS scores (p < 0.001) after the TCQ training, while there was no change in the control group. In a group comparison, there was a statistically significant improvement in the ESS score of the intervention group (p = 0.001).
Discussion
Our findings indicate that compared with those in a home exercise group, those enrolled in a 12-week training program of TCQ experienced significant decreases in severity of OSA and daytime sleepiness, and it improved subjective quality of sleep in patients with mild and moderate OSA.
The AASM recommends exercising as a behavioral treatment option for patients with OSA. 37 A community-based, large cohort analysis demonstrated that effective and regular physical activity was associated with reduced prevalence of OSA. 5 A meta-analysis of research on the effects of exercise on the treatment of OSA also led to the conclusion that exercise training significantly decreased the severity of OSA and that this decrease was achieved without any change in body weight. 6 In this meta-analysis, exercises applied in the studies included were mostly moderate in intensity. In our study, we obtained a 30% change in the AHI compared with the baseline in the TCQ training group without any BMI reduction. TCQ training is considered mild to moderate aerobic exercise at 1.6–4.6 metabolic equivalents registering 50%–74% maximal heart rate, depending on the age of the individual and the intensity of practice. 38 Despite decreased intensity of exercise, similar physiological results were obtained with moderate exercises. The reason for this may be that TCQ training includes respiratory and relaxation components such as body–mind exercises as well as physical components.
There are several possible mechanisms by which exercise can modulate sleep-disordered breathing. One possibility exists that exercise during wakefulness may improve upper airway dilator function (e.g., motor tone or strength) during sleep. 39 Other possibilities include exercise-induced reorganization of parapharyngeal fat distribution, alterations in control of breathing, and arousal threshold. 40 In recent years, the pathogenesis of OSA has also been focused on rostral fluid shift at night. According to this hypothesis, during the daytime, fluid accumulates in the interstitial and intravascular spaces of legs due to gravity. Lying down at night, fluid shifts rostrally toward the neck, where it may narrow the upper airway, predisposing it to upper airway collapse and OSA. 41 Studies have been conducted to examine the effect of exercise on overnight fluid shift. 42,43 Mendelson et al.'s 43 randomized controlled trial on patients with coronary artery disease and OSA showed that 4 weeks of moderate aerobic exercise training reduced the AHI (34%) by reducing the amount of fluid displaced from the legs into the neck overnight, despite the absence of any improvement in physical fitness or weight loss. In our study, overnight fluid shift was not measured, but lack of a significant change in the time spent in the supine position in PSG suggests that the decrease in AHI is due to the effect of TCQ exercise on overnight fluid shift. In sum, TCQ exercise may have affected OSA severity by all of the possible mechanisms mentioned above. Yet, the most salient point is that TCQ has similar effects to moderate-intensity aerobic exercises even though it has mild to moderate exercise intensity. This can be explained by the fact that in addition to physical components of TCQ, the deep breathing component as a body–mind exercise generates changes in the upper airway.
The effects of exercise training on PSG parameters in addition to AHI are not clear. Kline et al. 44 reported significant improvements in the oxygen desaturation index and N3 sleep, as well as AHI, with 12 weeks of exercise training. In a different study, 45 a 6-month, long-term exercise training program improved the AHI, but no changes occurred in other parameters. In our study, in addition to the AHI, there were significant improvements in stage N2 and N3 sleep. Based on the fact that stages N1 and N2 comprise superficial sleep, and N3 is the resting stage known as deep sleep, 46 the sleep of patients in the intervention group was found to be deepened. This change in the sleep stages may result from meditative characteristics of TCQ exercises. Providing mentally and physically relaxing TCQ exercises may have supported the change in sleep stages by reducing the sympathetic outputs. In the control group, there was a modest increase in the AHI of patients. Although this increase is not significant, it may still disrupt the patient's sleep, resulting in a decrease in deep sleep and consequent increase in superficial sleep.
There are a few limitations to this study worth noting. While improvements in the severity of OSA, daytime sleepiness, and quality of sleep were observed with TCQ training, we are yet unable to investigate the long-term outcomes. As no physiological assessment was performed to explain the effect of TCQ on OSA (fluid shift or muscle/fat distribution of upper airways), the extent to which we can make definitive statements is limited. Furthermore, in this randomized controlled study, we evaluated the severity of sleep apnea in a multidirectional way using objective and gold standard measurements in the clinical setting. To the best of our knowledge, this is the first study to investigate the effect of TCQ training on OSA; however, further studies are required to confirm these findings and to establish a definite conclusion.
In conclusion, our study results show that TCQ exercises may reduce the AHI values of mild and moderate OSA patients, regardless of BMI, and provide deeper sleep, improving subjective sleep quality and daytime sleepiness. Based on these results, we suggest that TCQ training may be an alternative method to conventional modalities in OSA treatment.
Footnotes
Acknowledgments
The authors would like to thank Melih Zeren, PhD (PT), for his support in writing the manuscript. The authors are indebted to Esra Pehlivan, PhD (PT), and Arif Balcı (PT), for their assistance with data collection. They also thank Tai Chi and Qi Gong Healing Institute Board member Master (instructor) Tarik Tekman for his valuable contribution to the TCQ training program. Patients' PFT and PSG expenses were supported by the Research Fund of Bezmialem Vakif University (Project No: 12.2015/5).
Author Disclosure Statement
No competing financial interests exist.