
Abstract
Objectives:
Rice bran oil (RBO) is a major source of monounsaturated fatty acid and gamma-oryzanol, which may assist in lowering blood lipids and oxidative stress. This study examined the effects of RBO containing different amounts of gamma-oryzanol on blood lipid, antioxidant, and inflammatory markers.
Materials and methods:
A total of 59 hyperlipidemic subjects completed the study. They were divided into four groups: RBO1 (4,000 ppm gamma-oryzanol, n = 14), RBO2 (8,000 ppm gamma-oryzanol, n = 15), RBO3 (11,000 ppm gamma-oryzanol, n = 15), and control (soybean oil, n = 15). The assigned oil (30 mL) was incorporated into three cooked meals each day for 4 weeks. Anthropometrical measurements and blood samples were taken to evaluate body weight, body composition, lipid parameters, antioxidant status, and inflammatory markers before and after the intervention.
Results:
Compared with the control, consumption of RBO significantly decreased low-density lipoprotein cholesterol (LDL-C) levels (percentage change: −0.8% [control]; −8% [RBO1]; −11.8% [RBO2]; and −12.2% [RBO3], p = 0.012) with the greatest change found in RBO2 and RBO3. In addition, antioxidant status also improved significantly. Levels of oxygen radical absorbance capacity (ORAC) and ferric reducing antioxidant power (FRAP) increased after consumption of a diet with RBO compared with consumption of a diet with soybean oil (ORAC: −2.7% [control]; 4.1% [RBO1]; 8.6% [RBO2]; and 10.1% [RBO3], p < 0.001; FRAP: −4.4% [control]; 4.7% [RBO1]; 7.4% [RBO2]; and 7.6% [RBO3], p < 0.001).
Conclusions:
RBO with gamma-oryzanol could decrease LDL-C levels and increase antioxidant capacity in hyperlipidemic subjects. Therefore, RBO consumption may reduce cardiovascular disease risk factors.
Introduction
Cardiovascular disease (CVD) was ranked as the first most important cause of death worldwide in 2015 by the World Health Organization (WHO). Approximately 17.7 million people were reported to die from CVD, with the highest prevalence found in developing countries. In addition, the number affected is expected to increase to 23.6 million people within 15 years. 1 Obesity, oxidative stress, and chronic inflammation are major contributors to CVDs, especially in hyperlipidemic subjects. 2
Consumption of healthy food is one of the best ways to prevent the development of CVD or to relieve its severity. Recently, rice bran oil (RBO) has become popular due to its healthy components and properties. RBO is extracted from the outer bran layer of the rice grain. 3 It is a rich source of monounsaturated fatty acid and antioxidant compounds such as gamma-oryzanol, tocopherols, tocotrienols, and phytosterols. 4 Previous studies have reported the health benefits of gamma-oryzanol on blood lipid reduction and elevation of antioxidant capacity in vitro and in vivo. 5 –7 Kennedy et al. revealed that the intake of RBO along with canola oil in the ratio of 80:20 for 30 days resulted in lowered levels of total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), and triglyceride (TG). 8 The effect of RBO on TC and LDL-C was also found in the study conducted by Zavoshy et al. They speculated that RBO may decrease levels of TC and LDL-C by inhibiting HMG-CoA reductase, the enzyme involved in cholesterol synthesis. 9 Moreover, RBO has been shown to protect against oxidative stress and inflammation. 10,11 Rao et al. showed that RBO can reduce serum concentrations of C-reactive protein (CRP), an indicator of acute inflammation, and interleukin-1β. 10
Therefore, RBO has the potential to reduce CVD risk factors. However, clinical studies of the effect of consuming meals cooked using RBO with varied gamma-oryzanol concentrations on lipid profiles and antioxidant status are limited. Therefore, it was aimed to investigate the effects of RBO consumption on biochemical parameters of CVD risk, as well as to determine whether the concentrations of gamma-oryzanol affect blood lipid levels, and antioxidant and inflammatory markers among hyperlipidemic adults.
Materials and Methods
This study was approved by the Ethical Review Committee for Human Research, Faculty of Public Health, Mahidol University (MUPH 2017-162). Furthermore, this study was conducted in accordance with the Declaration of Helsinki on human subjects.
Sample size calculation
The power calculation was based on the ability to detect a 5% difference in LDL-C in the primary analysis of the RBO versus the control, assuming a 10% standard deviation (SD) of effect (α = 0.05 and β-1 = 0.8) and an anticipated dropout rate of 10%. To satisfy these specifications, 60 subjects were required and were recruited.
Subjects
Sixty subjects aged 20–60 years were recruited at the Department of Nutrition, Faculty of Public Health, Mahidol University. The inclusion criterion was fasting LDL-C level of >100 mg/dL. Subjects had no diabetes, kidney or liver disease. Subjects who were smokers, pregnant or nursing, or regular users of a pharmaceutical or dietary supplements that affect lipid levels were excluded.
Study design and dietary intervention
This was a randomized double-blind controlled study. A total of 60 subjects with hyperlipidemia were randomly divided into four groups. The three treatment groups RBO1 (n = 15), RBO2 (n = 15), and RBO3 (n = 15) received freshly cooked meals that contained RBO that had 4000, 8000, and 11,000 ppm of gamma-oryzanol, respectively. The control group (n = 15) was provided with freshly cooked meals that contained soybean oil. Subjects in all three groups were given three meals a day for 4 weeks. The diet schemes were prepared by research assistants/dietitians and adopted from the Thai Food-based Dietary Guidelines. The daily energy and nutrients provided to each study group are presented in Table 1. The meals supplied a daily intake of 30 mL of RBO or soybean oil and contained 1,600 kcal with 55% of energy derived from carbohydrate, 15% from protein, and 30% from fat. Meals were cooked with the allocated oils and included fried rice with pork, fried fish, Thai soup, and stir-fried vegetables. Research assistants visited subjects to serve every meal (breakfast, lunch, and dinner) and check compliance for consumption of foods as planned by observing subjects at their workplace every day. Subjects were asked to record their daily food intake to determine whether any other foods were consumed.
Energy and Nutrient Contents of Study Diets
MUFA, monounsaturated fatty acid; PUFA, polyunsaturated fatty acid; RBO, rice bran oil; SFA, saturated fatty acid.
Anthropometrical assessments
Subjects were physically examined at the beginning of the study. Body weight and height were measured that were used to calculate body mass index (BMI). Percentage total body fat and blood pressure were also measured.
Laboratory analysis
Blood was drawn from subjects while they were in a fasting state (10–12 h overnight fast) at the beginning and end of the 4-week intervention. Laboratory technicians determined the concentrations of lipids (TC, LDL-C, high-density lipoprotein cholesterol [HDL-C], and TG), antioxidant parameters (oxygen radical absorbance capacity [ORAC] and ferric reducing antioxidant power [FRAP]), and the marker of acute inflammation (high sensitivity-C-reactive protein [hs-CRP]). Lipid profiles were determined by an enzymatic colorimetric assay. Antioxidant capacity was evaluated using ORAC and FRAP assays, which were popular methods and valid measures of antioxidant status in biological sample. hs-CRP was determined by latex immunoturbidimetry assay. Kidney function was assessed by blood urea nitrogen and creatinine. Liver function was assessed by aspartate aminotransferase (AST) and alanine aminotransferase (ALT). All biochemical analyses were carried out at N Health Asia Lab, Bangkok, Thailand, which is a medical laboratory with ISO15189:2007 certification.
Statistical analysis
Statistical package for the social sciences (SPSS) version 18.0 was used to perform all statistical analyses. The data are presented as mean ± SD. Differences between study groups were determined using one-way analysis of variance (ANOVA) and Tukey test. A p-value <0.05 was considered statistically significant.
Results
Characteristics of subjects at baseline
A total of 80 participants were screened for eligibility and 60 participants were randomized and entered into the study (Fig. 1). General characteristics are presented in Table 2. There were no significant differences in age, weight, BMI, body fat, blood pressure, kidney and liver function, lipid profiles, and antioxidant and inflammatory markers between the four groups (RBO1, RBO2, RBO3, and control) at baseline. One subject in the RBO1 group dropped out due to common cold; thus, a total of 59 subjects (98.33%) completed the study. All subjects who completed the study were able to follow the study protocol and consumed the meals as planned.
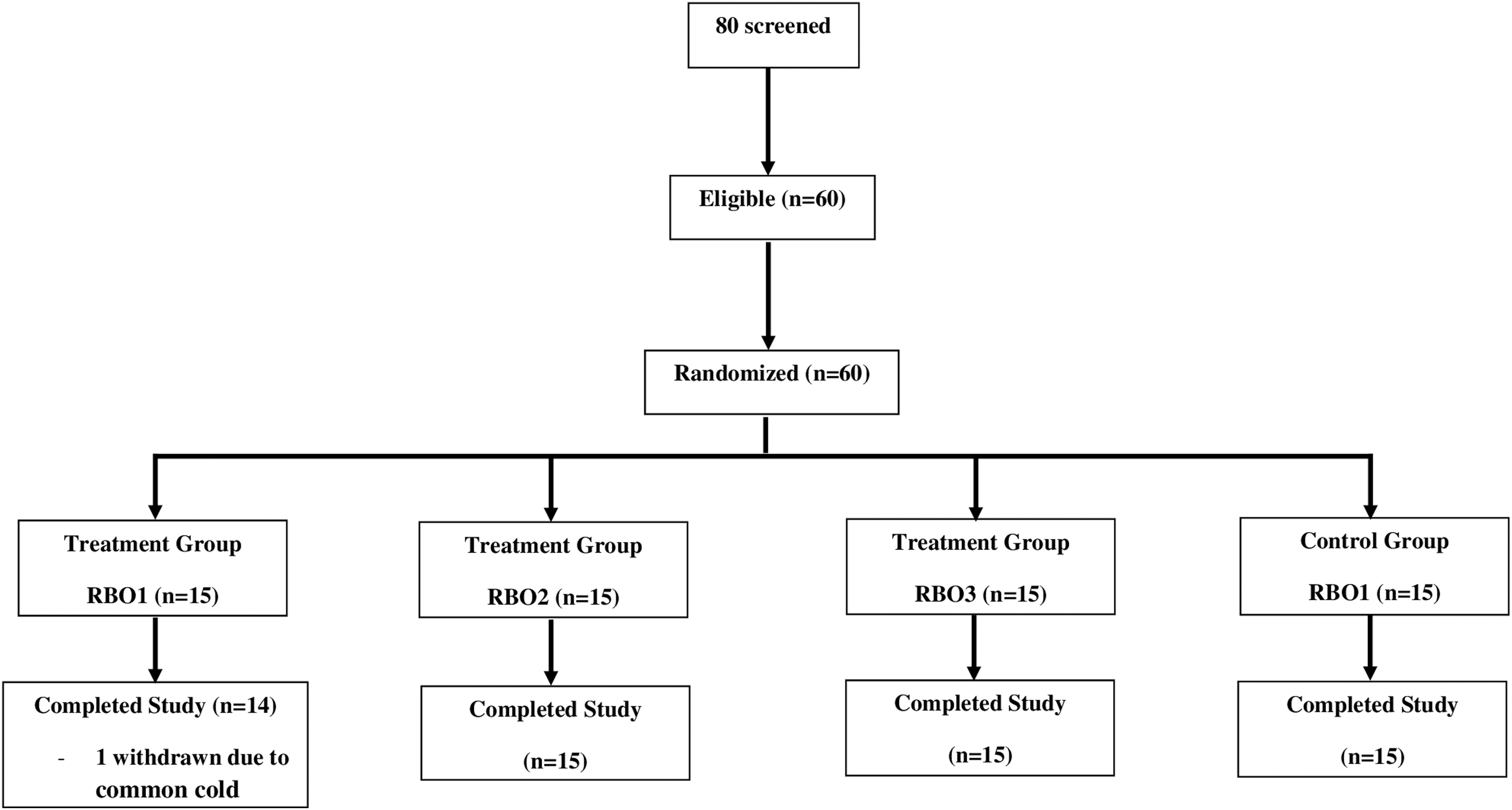
Study design and flow diagram. RBO, rice bran oil.
General Characteristics and Blood Chemistry of Subjects at Baseline
Values are means ± SD. There were no significant differences between the four groups at baseline.
AST, aspartate aminotransferase; ALT, alanine aminotransferase; BUN, blood urea nitrogen; FRAP, ferric reducing antioxidant power; HDL-C, high-density lipoprotein cholesterol; hs-CRP, high sensitivity-C reactive protein; LDL-C, low-density lipoprotein cholesterol; ORAC, oxygen radical absorbance capacity; RBO, rice bran oil; SD, standard deviation; TE, trolox.
Effects of RBO with varied gamma-oryzanol on lipid profiles
Significant postintervention differences in weight change between each of the study groups were not observed (−0.86 ± 0.99 kg [RBO1]; −0.78 ± 1.28 kg [RBO2]; −0.73 ± 1.95 kg [RBO3]; and −0.17 ± 0.66 kg [control group], p = 0.474). The effects of RBO consumption on lipid profiles are presented in Table 3 and Figure 2. RBO containing varied amounts of gamma-oryzanol significantly decreased the levels of LDL-C compared with the soybean oil control (−0.8% [control]; −8% [RBO1]; −11.8% [RBO2]; and −12.2% [RBO3], p = 0.012). Daily consumption of 8,000 ppm gamma-oryzanol (RBO2) and 11,000 ppm gamma-oryzanol (RBO3) reduced LDL-C levels more than daily consumption of 4,000 ppm gamma-oryzanol (RBO1) (p < 0.05). However, there was no significant difference between the reduction in LDL-C after daily consumption of 8,000 ppm gamma-oryzanol (RBO2) versus daily consumption of 11,000 ppm gamma-oryzanol (RBO3). There were no significant changes in the levels of TC, HDL-C, and TG (p = 0.063, p = 0.358, and p = 0.174, respectively). However, the levels of TC in the RBO groups showed a downward trend after the intervention.

Effects of rice bran oil with varied gamma-oryzanol on lipid profiles. a–cValues with different superscripts are significantly different from each other (p < 0.05). HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol. Color images are available online.
Lipid Profile of Subjects at Before and After Intervention
Values are means ± SD.
Comparison of mean change between four groups; significant differences at p < 0.05.
HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; RBO, rice brain oil; SD, standard deviation.
Effects of RBO with varied gamma-oryzanol on antioxidant and inflammatory status
The effects of RBO consumption on antioxidant markers are presented in Figure 3. RBO containing varied amounts of gamma-oryzanol significantly increased the levels of ORAC compared with the soybean oil control (−2.7% [control]; 4.1% [RBO1]; 8.6% [RBO2]; and 10.1% [RBO3], p < 0.001). Daily consumption of 8,000 ppm gamma-oryzanol (RBO2) and 11,000 ppm gamma-oryzanol (RBO3) increased ORAC levels more than daily consumption of 4,000 ppm gamma-oryzanol (RBO1) (p < 0.05). Furthermore, consumption of RBO containing gamma-oryzanol significantly increased the levels of FRAP compared with the soybean oil control (−4.4% [control]; 4.7% [RBO1]; 7.4% [RBO2]; and 7.6% [RBO3], p < 0.001). However, there were no significant differences in FRAP increase between the three RBO groups after the intervention. Regarding the indicator of inflammation, there were no significant changes in the levels of hs-CRP (p = 0.807).
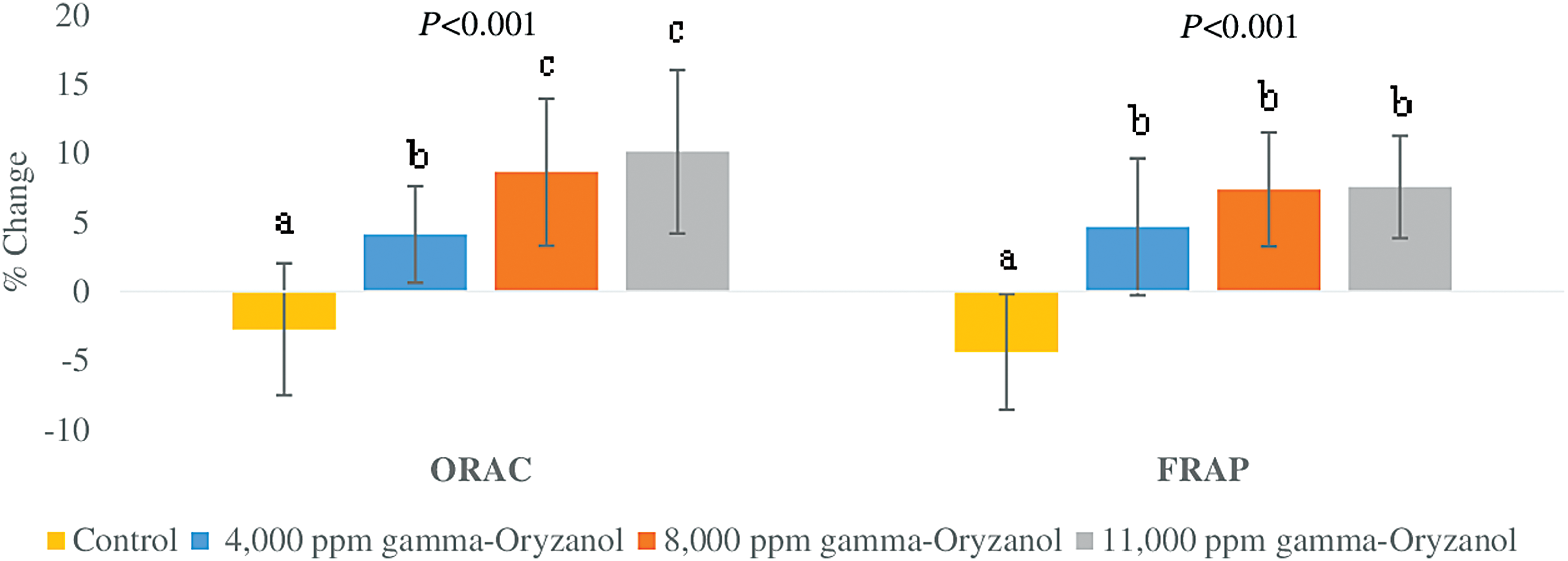
Effects of rice bran oil with varied gamma-oryzanol on antioxidant status. a–cValues with different superscripts are significantly different from each other (p < 0.05). FRAP, ferric reducing antioxidant power; ORAC, oxygen radical absorption capacity. Color images are available online.
Discussion
RBO has been recognized as a healthy oil for cardiovascular health because of its lipid lowering properties. The major phytochemical found in RBO, gamma-oryzanol, has been shown to improve levels of blood lipids and reduce oxidative stress. Thus, it possibly reduces CVD risk factors. In this study, the effect of RBO with varied amounts of gamma-oryzanol on biochemical markers related to CVD is determined. It is shown that daily consumption of RBO-enriched meals containing 4,000, 8,000, and 11,000 ppm gamma-oryzanol for 4 weeks can decrease LDL-C levels and increase ORAC and FRAP in hyperlipidemic subjects. However, the changes in LDL-C at the end of 4 weeks were not clinically significant. This may be due to the duration of the intervention.
In this study, the subjects were at high risk of developing CVD. On average, the BMI of all subjects was classified as overweight/obese (BMI ≥23.0 kg/m 2 ), according to the BMI criteria for Asians set by the WHO. 12 Mean blood lipid levels were also at levels considered to be borderline high risk (TC ≥200 mg/dL and LDL-C ≥ 130 mg/dL). 13 Besides, a previous study reported that obesity and dyslipidemia are the crucial factors in inducing oxidative stress and the release of proinflammatory cytokines, both risk factors for CVD. 14
Rice bran is a by-product of the rice milling process. 15,16 The amount of oil that can be extracted from rice bran is about 17%. 17 In general, RBO is used widely for cooking and baking. It is reported to be a rich source of bioactive phytonutrients with anti-inflammatory and antioxidant properties. 4 Gamma-oryzanol is a major phytonutrient component of rice bran, which is made from a mixture of triterpenyl esters of ferulic acid and sterols. 16
The possible mechanism of action by which gamma-oryzanol reduces LDL-C is through the inhibition of HMG-CoA reductase, a key enzyme involved in cholesterol synthesis in the liver. Moreover, sterols in the gamma-oryzanol molecule may decrease cholesterol absorption. 9,18 –23 In addition, Jolfaie et al. reported that gamma-oryzanol may decrease blood lipid level by inducing the release of cholesterol 7-alpha-hydroxylase (CYP7A1), an enzyme that plays a role in maintaining cholesterol level. 24,25 Furthermore, the LDL-C lowering effect of RBO in this study may be similar to that of Chen and Cheng. They found that RBO was able to increase LDL receptors in an animal model. 26
In this study, it is found that daily consumption of meals containing RBO significantly increased serum antioxidant power, ORAC, and FRAP. Consistent with these data, Rao et al. showed that RBO elevated antioxidant capacity in an animal model. 10 Shih et al. showed that RBO increased levels of antioxidant parameters: hepatic glutathione, superoxide dismutase, catalase, and thiobarbituric acid reactive substance. 27 The antioxidant properties might be due to gamma-oryzanol, which is a major bioactive compound in RBO. Dhavamani et al. found that after removing gamma-oryzanol from RBO, antioxidant capacity in rats was lessened. 28 Furthermore, gamma-oryzanol was shown to disrupt the excretion of proinflammatory cytokines, for example, CRP. 29 In an animal study, levels of CRP significantly dropped after a diet containing RBO. 10 However, a significant change in hs-CRP levels was not found in this study.
Based on the result, concentrations of 8,000 ppm gamma-oryzanol and 11,000 ppm gamma-oryzanol in RBO can reduce LDL-C levels and enhance ORAC more than those of 4,000 ppm gamma-oryzanol. However, there was no significant difference between the concentrations of 8,000 ppm gamma-oryzanol and 11,000 ppm gamma-oryzanol in RBO. Therefore, 8,000 ppm gamma-oryzanol in RBO may be a sufficient dose for consumption to get the most effective health benefits in lowering LDL-C and increasing ORAC. Regarding FRAP, not a significant difference was found in FRAP increase between the three RBO groups. This could indicate that gamma-oryzanol can eliminate oxygen radicals better than ferric radicals.
Although a limitation of this study was its small sample size, it was a randomized double-blind controlled design, and the diets were designed and provided by dietitians. Moreover, the results from food records showed that the participants did not eat more food outside of the study, indicating a good compliance. The findings suggest that the daily consumption of meals made with RBO, containing gamma-oryzanol, may be beneficial in lowering LDL-C and improving antioxidant status.
Conclusions
The consumption of 30 mL RBO with 4,000, 8,000, and 11,000 ppm gamma-oryzanol daily for 4 weeks can improve CVD risk factors by decreasing LDL-C levels and increasing antioxidant capacity (ORAC and FRAP) in hyperlipidemic subjects. The greatest effects were found in the subjects who consumed meals made with RBO containing 8,000 and 11,000 ppm gamma-oryzanol. Therefore, RBO may be a functional food for cardiovascular health.
Footnotes
Acknowledgments
The authors thank Dr. Carol Hutchinson, Department of Nutrition, Faculty of Public Health, Mahidol University, Bangkok, Thailand, for reading and editing the article. This study was funded by Thai Edible Oil Co. Ltd. and also partially supported for publication by the China Medical Board (CMB), Faculty of Public Health, Mahidol University, Bangkok, Thailand.
Author Disclosure Statement
No competing financial interests exist.