
Abstract
Introduction:
Main cardiovascular parameters such as heart rate (HR), blood pressure, and myocardial oxygen consumption (MOC) are tightly regulated by a multifactorial, nonlinear control system. Increased HR because of physical activity is often accompanied by an increase in blood pressure. Postural changes have an effect on the baroreceptors, and stretching exercises and isometric contractions modulate muscle mechanoreceptors eliciting increases in blood pressure. However, a hot environment increases the core temperature inducing vasodilation and plasma volume changes that might contribute to a drop in blood pressure. During the practice of Bikram yoga, all these factors converge and little is known about the resulting changes in blood pressure and MOC.
Methods:
Sixteen apparently healthy female volunteers, regular practitioners of Bikram yoga, were evaluated during a 90 min session. Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured immediately after each posture and HR was measured continuously during the practice.
Results:
HR and estimated MOC increased significantly over baseline during the exercise (+62.3% and +63.6%, respectively). HR mean value across the entire Bikram yoga session was 126.6 ± 14.3 bpm reaching a maximum of 168.1 ± 20.2 bpm. SBP was not significantly increased over baseline at any time during the practice with a mean value of 117.0 ± 10.1 mmHg and DBP was significantly decreased over baseline most of the time (−10.1%, mean 71.2 ± 7.3 mmHg) with particular decline toward the end of the practice during the floor postures.
Conclusions:
DBP during the practice of Bikram yoga was significantly different from that previously reported for nonheated Hatha yoga for normotensive subjects. Further studies evaluating the same group at both conditions are needed to better characterize the magnitude of the changes in HR, SBP, DBP, and MOC.
Introduction
Hatha yoga consists of a combination of isometric muscular contractions, stretching exercises, relaxation techniques, and breathing exercises that makes it different from any other mode of physical activity. 1 However, similar to other physical activities, the practice of Hatha yoga elicits acute increases in heart rate (HR) and myocardial oxygen consumption (MOC), although to a smaller extent. 2
Hot yoga refers to yoga exercises performed under hot and humid conditions. It is often associated with Bikram yoga, a variant of Hatha yoga involving a standardized series of 26 physical postures (asanas) and 2 breathing exercises (pranayamas) performed to an instructional dialog in a room conditioned at 40.6°C and 40% humidity for 90 min. 3
Bikram yoga has become more and more popular, partly because its instructors affirm that its habitual practice favors detoxification and elimination of impurities through perspiration. 4 In addition, it has been postulated that during a typical session a regular subject could burn up to 1000 kcal, although scientific studies have shown that the average expenditure is 286 kcal. 5 Other studies demonstrated that the usual practice of Bikram yoga increases muscle strength, endurance, flexibility, improves body composition, balance, agility, and coordination. 3 Hunter et al. have shown a significant improvement in the endothelial function after 8 weeks of Bikram yoga practice, 6 as well as an increase in the elastic compliance of the arteries 7 and improved glucose tolerance in obese adults with impaired glucose tolerance. 8 In a later study, only a nonsignificant tendency to increase the endothelium-dependent vasodilatation was observed after 12 weeks of Bikram yoga, whereas this increase was found to be significant when the same postures were practiced at thermoneutral conditions. 9 Despite all the proven benefits, the American Council on Exercise recently published a study raising concerns about the safety of Bikram yoga because of the high core temperatures achieved by some of the participants during the study. 10
Four studies have investigated the medium-term (8 weeks to 1 year) effects of Bikram yoga practice on resting HR and blood pressure (BP) in normotensive adults and none of them reported significant changes over time. 7,11 –13 However, in nonheated yoga, where the literature is more extensive and includes more subjects, several studies reported that yoga effectively reduced BP in both normotensive and hypertensive subjects. 14
In the short term, physical activity produces an increase in HR and MOC. Postural changes induce rapid changes in the blood distribution in the body, acting on cardiopulmonary baroreceptors, which produce a suppression of the sympathetic vasoconstrictor effect. In addition, stretching exercises induce an increase in BP and sympathetic nervous system activity by modulating muscle mechanoreceptors. Likewise, the isometric muscle contraction causes mechanical compression of blood vessels that contributes to the BP increase. 15 On the contrary, techniques of relaxation and meditation are able to lower BP, antagonizing the effects mentioned before. 16,17
Miles et al. measured arterial BP, HR, stroke volume, and cardiac output during a nonheated Hatha yoga practice consisting of 23 postures including standing postures (SPs), floor postures (FPs), and inversion postures. 1 This study found that systolic blood pressure (SBP), mean arterial pressure, and diastolic blood pressure (DBP) increased significantly during the yoga postures, with the magnitude of the increase being greatest during SPs. The elevation in BP as a result of yoga practice and other similar exercises was associated with increases in cardiac output and HR. Moreover, the vast majority of physical exercises induce in normotensive and hypertensive subjects, a BP increase, especially at peak effort, which is followed by a multifactorial-induced reduction, even below resting values, occurring 5 min after exercise cessation. 18
Some authors claim that BP may rise during Bikram yoga practice, 19 but no scientific study has been performed to demonstrate this point. In addition to all the factors influencing BP during the practice of nonheated yoga, the high ambient temperature of a hot yoga room could have a crucial role in lowering BP by inducing vasodilation. Moreover, when the internal temperature rises to the point of causing heat stress, BP control might be compromised. 20
Monitoring of BP during exercise is a challenging task. 21 Manual cuff auscultation is the most commonly employed method because it is easy and does not require expensive automated equipment. However, it requires the presence of a trained operator close to each participant that can lead to misleading readings because of the “white coat effect” 22 and makes it difficult to measure multiple participants simultaneously. Another method of measuring exercise BP is the volume clamp that enables beat-by-beat monitoring and is accurate at low exercise intensity and for assessing acute BP changes such as with tilt table testing but is less reliable at high exercise intensities. 21,23 Automated sphygmomanometers and oscillometric devices validated to measure BP during exercise are also available as well as medical grade smart oscillometric BP monitors that, integrated with smartphones, are able to collect continuous, accurate BP data in real time, minimally intrusively and for multiple subjects at a time.
The present descriptive observational study aims to evaluate the physiologic responses of BP, HR, and MOC during a Bikram yoga session using wearable sensors. The working hypothesis is that HR, SBP, DBP, and MOC will increase during the practice of Bikram yoga.
Materials and Methods
Participants
Apparently healthy women who had been practicing Bikram yoga for at least 1 month at the time of the study were recruited through fliers posted at the Bikram yoga center where the study was conducted. Exclusion criteria included the following: heart disease, kidney disease, diabetes, and drug, alcohol or tobacco consumption 6 h before the yoga class.
Ethics, consent, and permissions
Informed written consent was obtained from all the participants. This study was approved by the Scientific Ethics Committee of the Faculty of Medicine of the Pontificia Universidad Catolica de Chile on November 8, 2016 (Project 16-271) and had the consent of the director of the yoga center where it was performed.
Protocol
The study was performed during a regular Bikram yoga class to reduce artifacts from a research environment. Participants were regular practitioners at the yoga center where the study took place, thus they were habituated to the environment. Before entering the room, a health survey was applied to each participant aimed to collect personal morbidity antecedents, smoke, alcohol, and drugs consumption and level of experience in the practice of Bikram yoga and other physical activities. In addition, height and weight were measured by a calibrated tall meter and an iHealth® Core smart scale. Body mass index (BMI) was calculated from these measurements. At the end of this assessment, a wireless iHealth BP5 blood pressure monitor was placed around the bare upper arm of each participant, 3 cm above the elbow fold, according to the user manual of the manufacturer. Moreover, a Polar® model H7 HR sensor was placed on the chest. Then, resting, standing, and sitting SBP, DBP, and HR were measured to determine baseline values.
Once the participants completed the health evaluation, they entered the yoga room to perform a regular 90 min Bikram yoga class. The class consisted of a series of SPs and a series of FPs repeated twice (Fig. 1). Participants were allowed to drink water at the “official water break” taking place after Eagle pose (SP4) (Fig. 1), and any time after it, always between postures. During the 90 min, HR was recorded continuously while BP was measured immediately after the second set of each posture, for a total of 24 systolic and diastolic values. iHealth BP5 monitors take approximately 45 sec for inflation, deflation, and reading. BP and HR were measured with the minimum possible intervention using smart sensors controlled by Bluetooth from the researchers' smartphones that were kept outside the room separated with a glass door, thereby allowing to keep track of the practice (Fig. 2). All data were recorded on the smartphone controlling the device. Special measures were taken for handling and saving data to preserve the identities of the participants.

SPs and FPs performed during a 90 min Bikram yoga session. FPs, floor postures; SPs, standing postures.
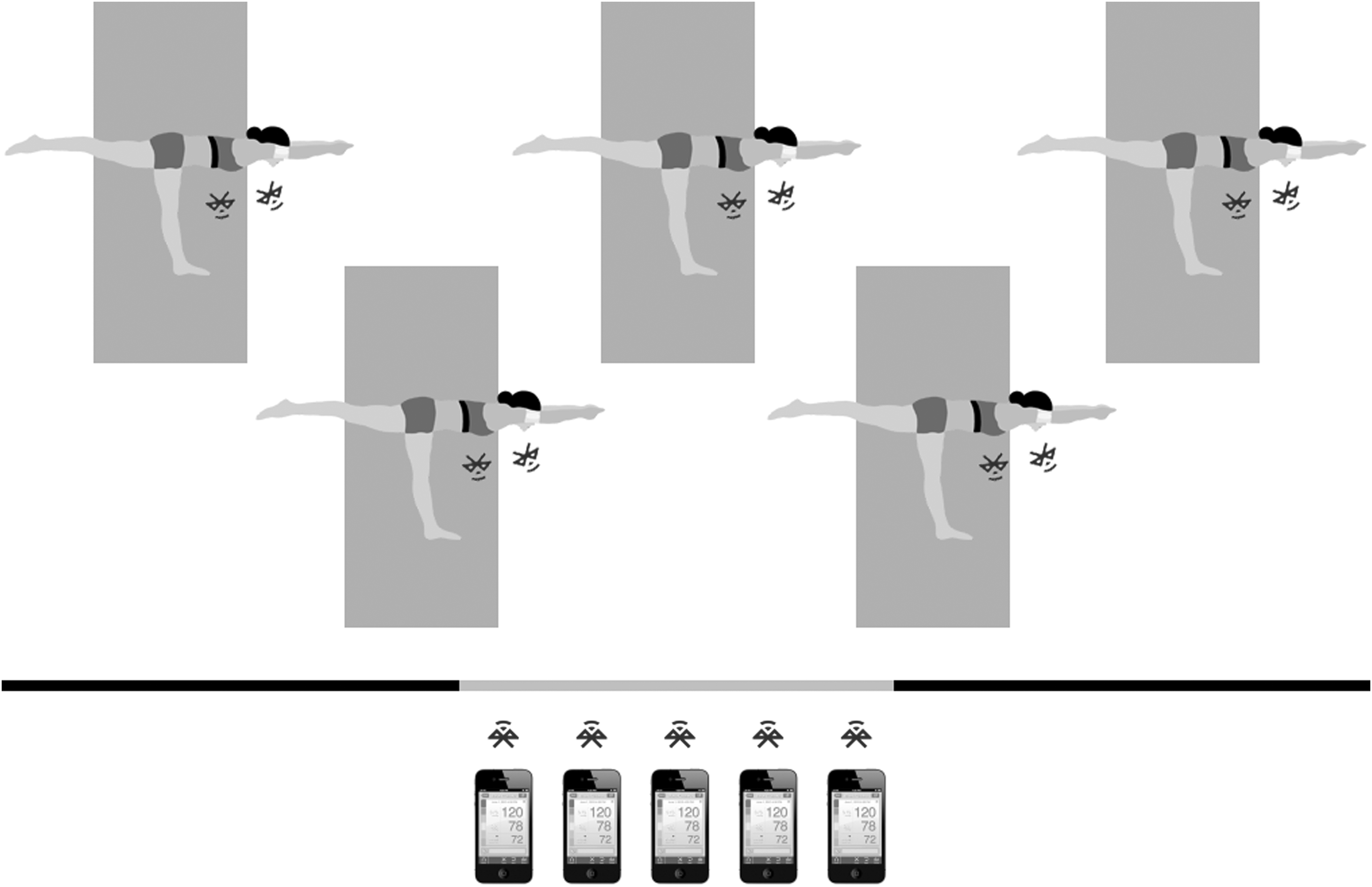
Room configuration. The participants wear a Bluetooth blood pressure cuff and a Bluetooth HR monitor during a regular Bikram yoga session. These monitors send the signals to the researchers' smartphones placed outside the room and separated by a glass door. HR, heart rate.
Monitoring devices
The iHealth BP5 is a wireless upper arm automated oscillometric BP monitor. It has been CE-marked for use in the European Union and has been approved by the Food and Drug Administration. Moreover, it has been validated according to the European Society of Hypertension International Protocol (ESH-IP) revision 2010. The iHealth BP5 passed all phases of the revision and showed a mean ± standard deviation (SD) device–observer difference of −1.21 ± 5.87 mmHg for SBP and −1.04 ± 5.28 mmHg for DBP, which represents a BP measurement accuracy for self/home monitoring in the general population. 24 The device communicates with the smartphone through Bluetooth. Inflation and deflation are automated and started by a command from the smartphone. Results of measurements (SBP, DBP, and HR) are transferred to the iHealth My Vitals application on the smartphone and the data were later downloaded to a data file for processing.
The HR monitor used in this study (Polar model H7) is electrode based and its accuracy has been confirmed showing a 0.99 (0.987–0.991 for 95% confidence interval) correlation coefficient agreement with standard ECG recording. 25
Data analysis
The maximum, minimum, mean, SD, coefficient of variation (CV), and SEM of the HR (bpm), SBP and DBP (mmHg), and the rate pressure product (RPP; bpm·mmHg) that estimates MOC 26 were calculated for each subject after every posture. In addition, a Student's t test for paired samples was used to compare the baseline values with the values obtained throughout the class. The Fligner–Killeen test was used to compare the variances of the measurements during the SPs versus the FPs.
Pearson's correlation coefficient was used to evaluate associations between BP and HR. Similarly, we searched for correlations between baseline, maximum, minimum, and mean SBP, DBP, HR, age, and BMI. Synchronization and accuracy of the two methods used for assessing HR (Polar H7 and iHealth BP5) were evaluated by cross-correlation analysis of the signals; r values were used to estimate synchronization intensity. The significance for each of the tests was set at p < 0.05.
Results
Sixteen volunteers were recruited (age: 40.3 ± 8.2 years, BMI: 25.8 ± 5.8 kg/m−2 ). Baseline values for HR, SBP, and DBP were 77.6 ± 8.8 bpm, 122.2 ± 13.3 mmHg, and 79.2 ± 12.1 mmHg, respectively. The BP monitors of two participants presented difficulties connecting to the smartphones and failed to receive most of the signals to take measurements. Therefore, these two participants were excluded from the study. For the rest of the participants, some of the measurements were also lost because of Bluetooth connection problems but worked well most of the time. The HR measurements obtained with the iHealth monitor showed good agreement with those obtained by the Polar monitor assessed by Pearson's correlation coefficient and cross-correlation analysis (r > 0.99).
HR was highly variable across postures but it was significantly elevated over baseline (+62.3%) during the whole practice with a mean value of 126.6 ± 14.3 bpm. Figure 3 provides the average of the HR for all the participants during the yoga session. The first half of the recording corresponds to the SPs and the second part corresponds to the FPs (see Fig. 1 for the name of each posture). Both SPs and FPs clearly modified HR response with significantly higher HR observed during SPs (16.4%; 142.8 ± 11.9 vs. 122.7 ± 6.5 bpm; p = 0.003). The average maximum value across participants occurred during triangle pose (SP9) and was 168.1 ± 20.2 bpm.
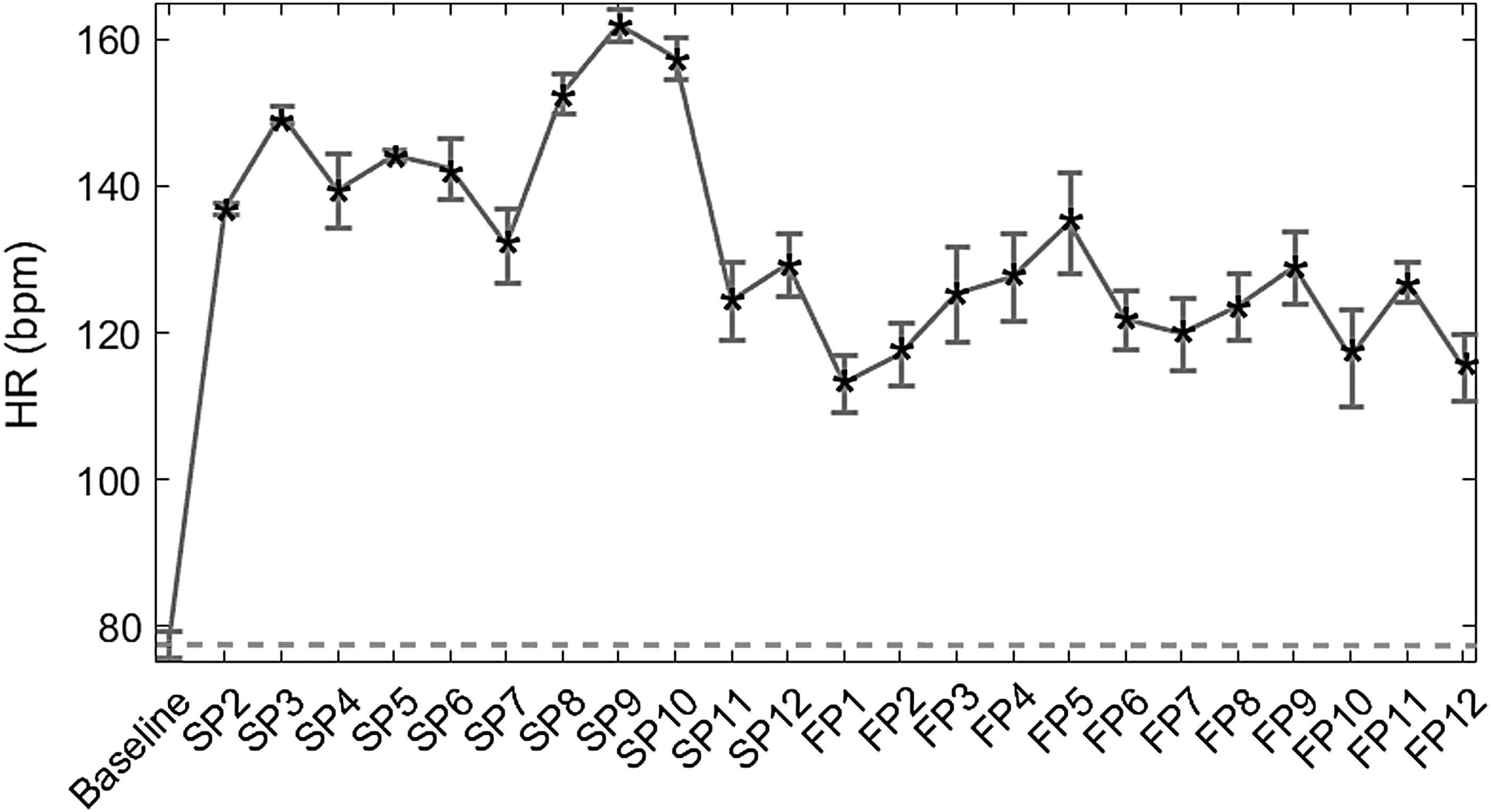
HR (bpm; mean ± SEM) of all volunteers at baseline and after every posture during the Bikram yoga session. The segmented line indicates the baseline value, curve with error bar corresponds to the mean and SEM HR after every posture and markers (*) indicate statistical differences (p < 0.05) versus baseline values. FP, floor posture; SEM, standard error of the mean; SP, standing posture.
SBP mean values from all volunteers after every posture are given in Figure 4. Despite all SBP mean values being below the baseline, which was measured immediately before the session, only after the last posture the SBP was significantly lower than baseline (−22.9%; 94.2 ± 10.1 mmHg; p = 0.02). The mean SBP value across the session was 117.0 ± 10.1 mmHg.
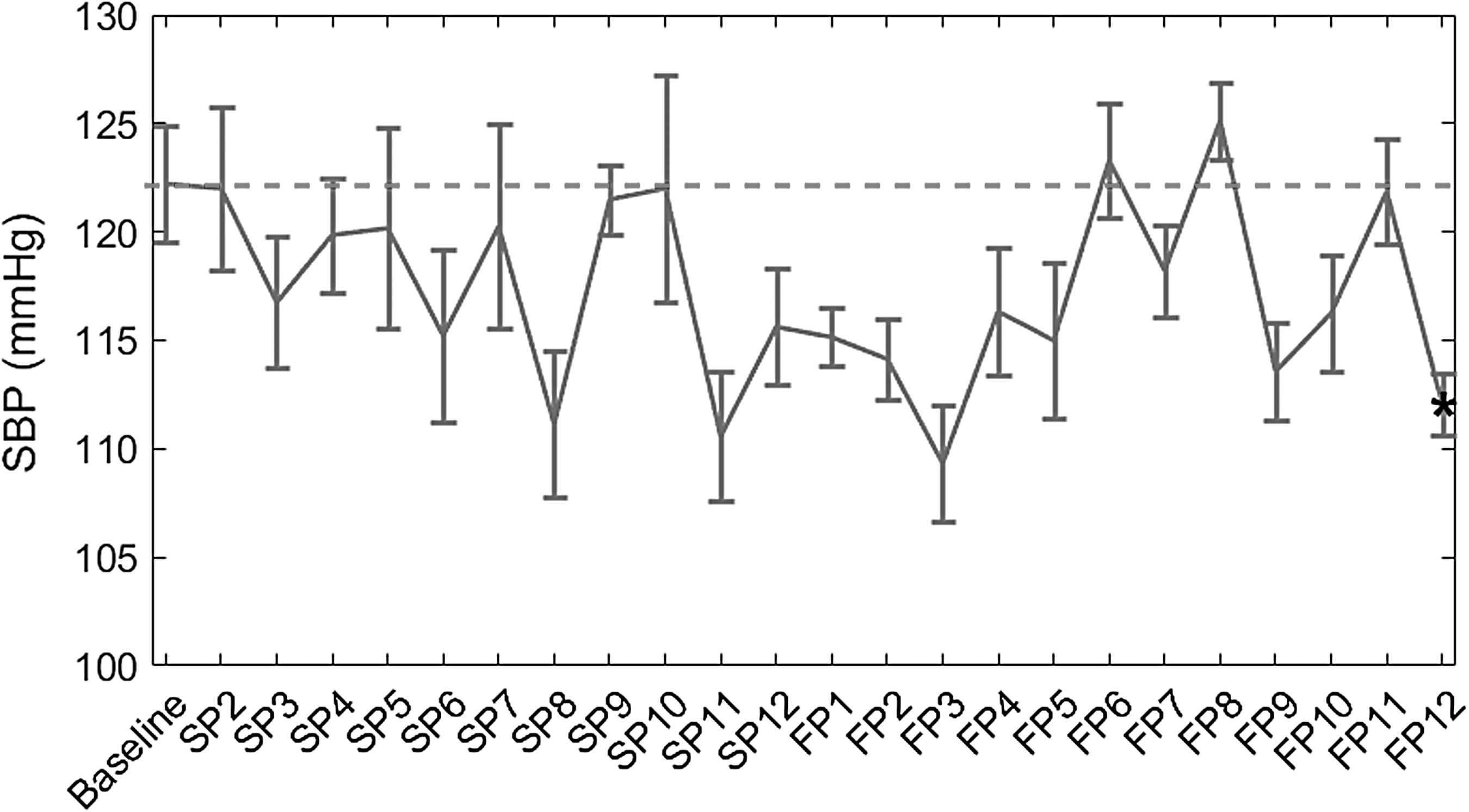
SBP (mmHg; mean ± SEM) of all volunteers at baseline and after every posture during the Bikram yoga session. The segmented line indicates the baseline value, curve with error bar corresponds to the mean and SEM SBP after every posture and markers (*) indicate statistical differences (p < 0.05) versus baseline values. Only the mean SBP after the last posture was statistically lower than the baseline. FP, floor posture; SBP, systolic blood pressure; SEM, standard error of the mean; SP, standing posture.
DBP during the Bikram yoga practice was lower than baseline most of the time (−10.1%; mean 71.2 ± 7.3 mmHg; p = 0.002) with particular decline toward the end of the session, during the FPs. Figure 5 shows with an asterisk the postures with a significant decrease. Dispersion values (SD and CV) for SBP and DBP were statistically higher for the SPs than for the FPs as revealed by the Fligner–Killeen test for homogeneity of variances.
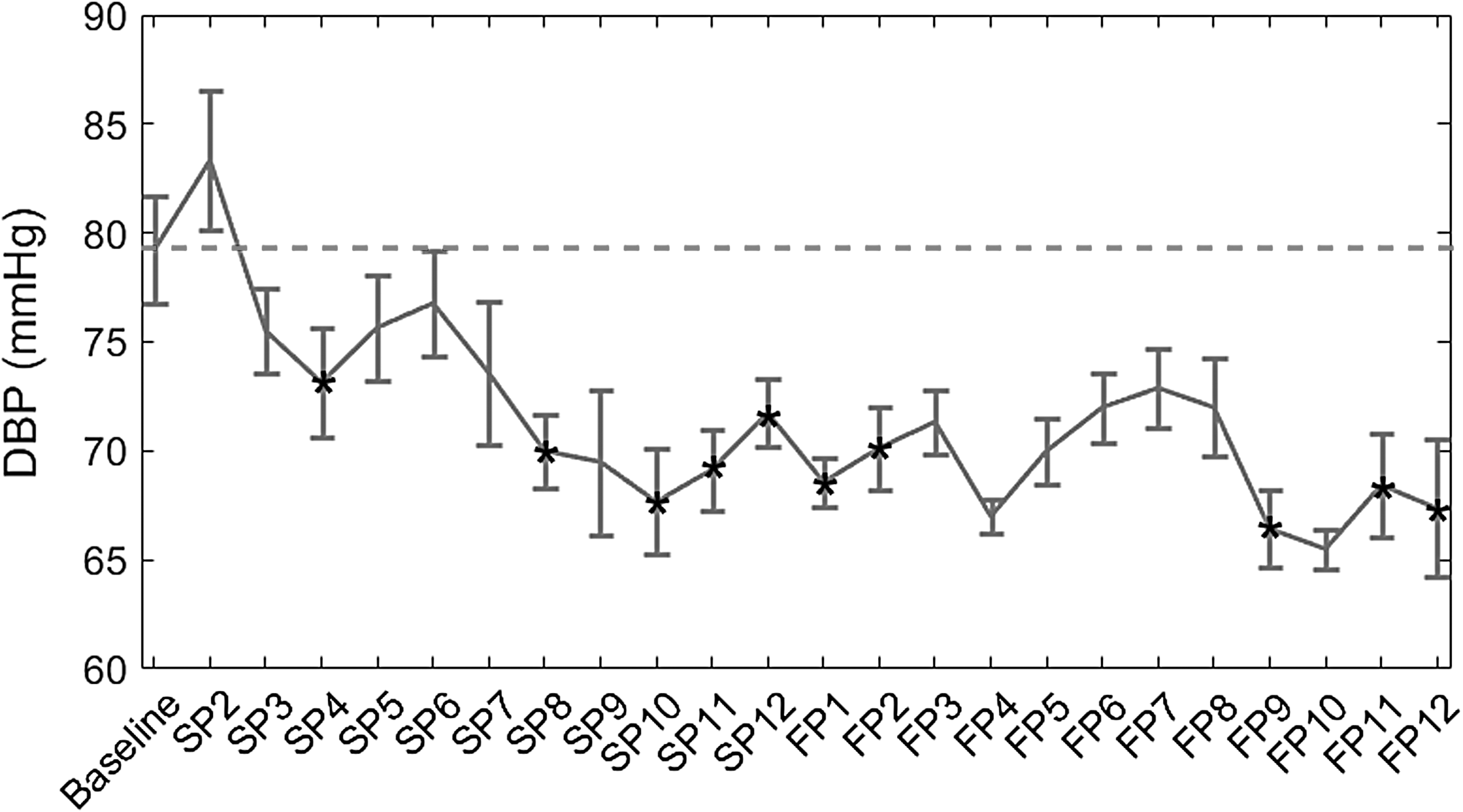
DBP (mmHg; mean ± SEM) of all volunteers at baseline and after every posture during the Bikram yoga session. The segmented line indicates the baseline value, curve with error bar corresponds to the mean and SEM DBP after every posture and markers (*) indicate statistical differences (p < 0.05) versus baseline values. Mean DBP after postures SP4, SP8, SP10, SP11, SP12, FP1, FP2, FP9, FP11, and FP12 was significantly lower than baseline. DBP, diastolic blood pressure; FP, floor posture; SEM, standard error of the mean; SP, standing posture.
MOC estimated by RPP shows that SPs increase the median of the mean MOC values by 76.6% over the baseline, whereas FPs increase it by 51.7% (Fig. 6). The median MOC values at SPs (16,828 ± 1742 bpm·mmHg) and FPs (14,450 ± 1017 bpm·mmHg) were statistically elevated over baseline (9528 ± 1742 bpm·mmHg), which represent 76.6% (p < 0.001) and 51.7% (p < 0.001) increase, respectively. MOC values were also significantly different between SPs and FPs (16.5%; p = 0.009).

Box plots for myocardial oxygen consumption (bpm·mmHg) estimated by HR and DBP product at baseline, SP, and FP Bikram yoga postures. Central rectangle spans the first quartile to the third quartile. The horizontal line inside the rectangle shows the median and whiskers above and below the box show the locations of the minimum and maximum. DBP, diastolic blood pressure; FP, floor posture; HR, heart rate; SP, standing posture.
BMI showed a weak and nonsignificant correlation with baseline SBP (r = 0.3; p > 0.05) but it showed a significantly strong correlation (r > 0.7; p < 0.015) with the minimum, maximum, and average SBP during the yoga practice.
Discussion
This study evaluated HR, BP, and RPP during the practice of a Bikram yoga session using wearable sensors, revealing that the increased environment temperature induced significant changes in DBP compared with the previously reported response to similar exercises at ambient temperature (23°C–25°C). The use of wearable sensors made possible to perform the study in the yoga studio where the participants practice regularly, thereby reducing artifacts because of research or clinical environments and allowing to monitor multiple participants simultaneously, minimizing the variability of the results.
HR response to a Bikram yoga session was previously studied by Pate 5 and the results found here are very close to those reported earlier. Namely, HR pattern showed a steady increase in its values during SPs, reaching its peak at triangle pose in both studies. After this, it decreases until the beginning of the FPs from where it stays steady until the end of the session. This response is similar in pattern to that reported for nonheated Hatha yoga 1 ; however, the mean and maximum values are higher for Bikram yoga. These results strongly suggest a higher and more intense demand on HR because of the increased environmental temperature. This is not surprising since passive heat stress alone (i.e., nonexercise) can significantly increase HR and cardiac output. 20
To the authors' knowledge, this is the first time that BP is measured during the practice of Bikram yoga. Our hypothesis was that HR, SBP, DBP, and MOC would increase during the practice of Bikram yoga. However, it is remarkable that, despite the isometric exercises that often increase BP and the higher demand on HR compared with similar exercises at ambient temperature, 1 the SBP remained unchanged and the DBP experienced a significant drop. These responses differ to the significant increases in both SBP and DBP reported by Miles et al. 1 during the practice of Hatha yoga at ambient temperature, and probably denote the decrease in peripheral vascular resistance and blood redistribution induced by the peripheral vasodilatation because of the high environmental temperature. 18,27 –30 Dehydration can be an additional factor contributing to the decrease in BP. We did not quantify fluid intake or sweat rate during the session but, despite free access to fluids during class, low consumption was reported in previous studies. 31 The combination of dehydration and hyperthermia during exercise in the heat causes an inability to maintain cardiac output and BP. 32 Moreover, the state of meditation that can occur during a yoga session may contribute to the decrease in BP by means of the relaxation response. 33,34
For healthy adults, a body's rise in skin temperature induces vasodilatation with a consequent temporary decrease of BP. 27,28,35 Shin et al. 36 studied the BP response to 10 min of hot-tub immersion at 40°C in a group of patients with treated hypertension and in a control group normotensive subjects. For both groups, SBP and DBP fell during immersion and they returned toward baseline within 10 min after the subjects left the hot tub. The duration of the immersion was relatively short and the core temperature of the subjects was not reported, so different responses could be expected for longer or different types of heat therapies (e.g., sauna bathing). However, several works have shown that sauna bathing is safe for healthy people and for most people with coronary heart disease with stable angina pectoris or old myocardial infarction. 37 Moreover, recent studies showed that frequent heat therapy or sauna bathing reduces the risk of elevated BP, 35,38 and fatal cardiovascular and all-cause mortality events. 39
Nonetheless, sudden exposure to cold after heat therapies activates the sympathetic nervous system and causes an increase in HR and constriction of cutaneous blood vessels. 37 Another mechanism that could affect the regulation of BP, beside the activation of the sympathetic nervous system, is the activation of the renin–angiotensin–aldosterone system in abrupt decreases in ambient temperature, which could generate a hypertensive emergency. 40 This is of great importance since the temperature drop experience after a Bikram yoga session can be higher than 20°C. This sharp decrease in the environmental temperature can cause, mainly in people with a history of cardiovascular disease, a sharp increase in BP. It remains for future research to study BP response after leaving the conditioned room and assess whether there is any risk of pressure rise because of sudden changes in temperature.
It is also important to evaluate the MOC during the Bikram yoga session. This parameter increased together with HR since SBP remained stable and confirms that SPs are the most demanding postures during Bikram yoga. 41
Another relevant finding of this study is the correlation among BMI and SBP during the yoga practice despite the lack of correlation with resting SBP. Measurements of resting BP often show spuriously elevated values because of anxiety, which decreases the reproducibility of the results and their usefulness for predicting future hypertension. This finding supports the study by Miyai et al., 42 which showed that better test–retest reliability can be achieved by BP assessment during an exercise test. BMI is a risk for hypertension; therefore, the elevated SBP during exercise could be an indicator of a higher risk of developing future hypertension for the subjects with higher BMI.
The main limitation of this study is the lack of a direct comparison with a nonheated Bikram yoga class and the relatively small number of participants. Moreover, water intake quantification along with weight measurements after the class would have been of interest to obtain data on water loss and correlate hydration levels to changes in BP.
Conclusions
The cardiovascular response pattern during the practice of Bikram yoga is significantly different from that reported for nonheated Hatha yoga. Namely, there is a significant decrease in DBP and no significant variation in SBP, despite a higher HR than during the practice of nonheated Hatha yoga. The decrease in BP can be explained by a combination of factors such as the vasodilatation of the arteries because of the high temperature. Further studies evaluating the same group at both conditions are needed to better characterize the magnitude of the cardiovascular changes.
Footnotes
Acknowledgments
This work was supported by FONDECYT grant No. 1181094. The authors thank Constanza Gardella, director of the studio Bikram Yoga Peñalolen, for her patience and flexibility and the participants themselves without whom this work would not have been possible.
Author Disclosure Statement
No competing financial interests exist.